High Dose Statins Should be Used in Most Acute Ischemic Stroke
High Dose Statins Should be Used in Most Acute Ischemic Stroke
High Dose Statins Should be Used in Most Acute Ischemic Stroke

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>High</strong> <strong>Dose</strong> <strong>Stat<strong>in</strong>s</strong><br />
<strong>Should</strong> <strong>be</strong> <strong>Used</strong> <strong>in</strong><br />
<strong>Most</strong> <strong>Acute</strong> <strong>Ischemic</strong><br />
<strong>Stroke</strong> Patients<br />
Majaz Moonis MD,FRCP, DM<br />
Department of Neurology<br />
UMass Memorial Medical Center
Why Use <strong>Stat<strong>in</strong>s</strong> Before or After AIS<br />
Reduce the risk of recurrent stroke<br />
Reduce Mortality<br />
Improve Outcome of <strong>Stroke</strong><br />
Primary and secondary prevention of MI,<br />
s<strong>in</strong>ce many patients have elevated LDL<br />
and unrecognized CAD
<strong>Stat<strong>in</strong>s</strong> Reduce Infarct Size<br />
Irrespective of the etiology of ischemic<br />
stroke, use of stat<strong>in</strong>s has <strong>be</strong>en associated<br />
with reduced <strong>in</strong>farct size and a more<br />
favorable outcome 1<br />
Cl<strong>in</strong>ically, greater reperfusion and <strong>be</strong>tter<br />
outcomes 2<br />
<strong>Stat<strong>in</strong>s</strong> given with<strong>in</strong> 4 weeks of stroke onset<br />
improve stroke outcome at 90 days<br />
compared to subjects not given stat<strong>in</strong>s 3<br />
Cardiovasc Pharmacol Ther. 2008;13(1): 72, <strong>Stroke</strong>,2011;42, <strong>Stroke</strong>:2005:1298
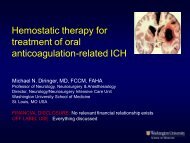
Stat<strong>in</strong> use and relative reperfusion.<br />
Stat<strong>in</strong> Use <strong>in</strong> Associated with Better<br />
Reperfusion and <strong>be</strong>tter outcomes<br />
Patients on stat<strong>in</strong>s had a greater<br />
reperfusion<br />
and a significantly <strong>be</strong>tter stroke outcome<br />
∆NIHSS 8.8 vs 4.4(p=o.28)<br />
The stat<strong>in</strong> group had significantly greater<br />
IHD compared to those not on stat<strong>in</strong>s<br />
Reperfusion correlated with <strong>be</strong>tter outcome<br />
<strong>Stroke</strong>,2011;42:1307<br />
Copyright © American Heart Association<br />
Ford A L et al. <strong>Stroke</strong> 2011;42:1307-1313
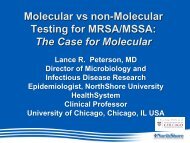
Biffi A et al. <strong>Stroke</strong> 2011;42:1314<br />
Meta-analysis forest plot.
<strong>Stat<strong>in</strong>s</strong>: RIS or Incident <strong>Stroke</strong><br />
HPS: In patients with IHD, Simvastat<strong>in</strong> 40mg/d<br />
reduced all cause mortality by 23%<br />
This was evident <strong>in</strong> all groups except those with preexist<strong>in</strong>g<br />
stroke<br />
IHD patients without preexist<strong>in</strong>g stroke <strong>be</strong>nefited <strong>in</strong><br />
prevention of <strong>in</strong>cident stroke<br />
SPARCL: In patients without known IHD,<br />
Atorvastat<strong>in</strong> 80mg/d reduced<br />
RIS 16% , TIA 27%, MI 33%<br />
Trend towards reduced severity of Non-Fatal <strong>Stroke</strong><br />
HPSCG(2002), Lancet 360(9362):7-22::Goldste<strong>in</strong> LB et al. <strong>Stroke</strong> 2009;40: 3526
Type of Major Vascular<br />
Event<br />
Simvastat<strong>in</strong> Allocated<br />
(N=10,269)<br />
Placebo Allocated<br />
(N=10,267)<br />
Nonfatal MI 357 (3.5%) 574 (5.6%)<br />
Coronary death 587 (5.7%) 707 (6.9%)<br />
Subtotal: major<br />
coronary event<br />
898 (8.7%) 1212 (11.8%)<br />
Nonfatal stroke 366 (3.6%) 499 (4.9%)<br />
Fatal stoke 96 (0.9%) 119 (1.2%)<br />
Subtotal: any stroke 444 (4.3%) 585 (5.7%)<br />
Coronary revascular 513 (5.0%) 725 (7.1%)<br />
Noncoronary<br />
revascular<br />
Subtotal: any<br />
revascular<br />
450 (4.4%) 532 (5.2%)<br />
939 (9.1%) 1205 (11.7%)
Cardioembolic <strong>Stroke</strong><br />
207 patients with IS and LDL < 100 mg/dl<br />
<strong>Stroke</strong> Distribution: CE 40%, AS 12% , SV 14%<br />
<strong>Stat<strong>in</strong>s</strong> 100, No <strong>Stat<strong>in</strong>s</strong>: 107<br />
31% discharged home with a good outcome<br />
Patients on <strong>Stat<strong>in</strong>s</strong> had a <strong>be</strong>tter outcome<br />
OR 1.91; p=0.033<br />
These <strong>be</strong>nefits were seen <strong>in</strong> all stroke sub-types<br />
Stead et al: J <strong>Stroke</strong> and Cerebovasc. Dis. 2009; 18:124
Why <strong>High</strong> <strong>Dose</strong> <strong>Stat<strong>in</strong>s</strong> ?<br />
12,689 patients with <strong>Ischemic</strong> <strong>Stroke</strong><br />
Included all stroke sub-types based on ICD-9<br />
codes<br />
Significant reduction <strong>in</strong> mortality <strong>in</strong> stat<strong>in</strong><br />
pretreated and post-stroke stat<strong>in</strong> patients<br />
compared to no stat<strong>in</strong> use<br />
<strong>Stat<strong>in</strong>s</strong> >60mg/d had <strong>be</strong>tter outcomes than<br />
those< 60 mg/d<br />
Cholesterol (TC, LDL) were not predictors<br />
Pleotropic effects were postulated to expla<strong>in</strong><br />
these protective effects<br />
Fl<strong>in</strong>t A C et al. <strong>Stroke</strong> 2012;43:147-154
Pleiotropic Effects of <strong>Stat<strong>in</strong>s</strong><br />
Pleiotropic effects of stat<strong>in</strong>s are dose dependent
<strong>High</strong> <strong>Dose</strong> Stat<strong>in</strong> adm<strong>in</strong>istration early <strong>in</strong> stroke hospitalization is associated with greater<br />
poststroke survival.<br />
Fl<strong>in</strong>t A C et al. <strong>Stroke</strong> 2012;43:147-154
The North Dubl<strong>in</strong> Population <strong>Stroke</strong><br />
Study<br />
448 patients with acute ischemic stroke were on<br />
stat<strong>in</strong>s or <strong>be</strong>gun on stat<strong>in</strong>s < 72 hours.<br />
<strong>Stat<strong>in</strong>s</strong> <strong>be</strong>fore or early after stroke onset resulted<br />
<strong>in</strong><br />
A highly significant prestroke stat<strong>in</strong> survival advantage<br />
(OR for death 0.12, 0.19, 0.26 at 7day,90days,1year; P<<br />
0.006)<br />
<strong>High</strong>ly significant poststroke stat<strong>in</strong>s use and survival (OR<br />
0.04; P=0.003, 0.23; P
<strong>Stat<strong>in</strong>s</strong> are safe for long term use<br />
Mataanalysis of 170,000 patients from 26 RCTs of <strong>in</strong>tensive Lipid<br />
lower<strong>in</strong>g therapy<br />
Death from non vascular causes or cancer did not defer from the stat<strong>in</strong> naive group<br />
Risk of ICH did not defer <strong>be</strong>tween high dose vs low dose stat<strong>in</strong>s<br />
Metaanalysis:66,201 patients:<br />
Outcome ICH did not defer <strong>be</strong>tween stat<strong>in</strong> vs nonstat<strong>in</strong> groups, stat<strong>in</strong>s were protective and<br />
ICH unrelated to TC or LDL<br />
CTTC metaanalysis:>90,000 patients: similar results<br />
SPARCL: <strong>in</strong>creased <strong>in</strong>cidence of hemorrhages, but no difference<br />
<strong>in</strong> symptomatic hemorrhage or mortality.<br />
Predictors of ICH: HTN, previous ICH, older age, microbleeds<br />
Risk of DM: Older women (HPS)<br />
No association with TC or LDL lower<strong>in</strong>g with high dose stat<strong>in</strong>s<br />
and outcomes or bleeds<br />
Lancet 2010;378:1670, Arch. Neurol2012 ;69:46
<strong>Stat<strong>in</strong>s</strong> <strong>Should</strong> <strong>be</strong> <strong>Used</strong> <strong>in</strong> <strong>Most</strong> AIS<br />
Reduce Risk of Recurrent or Incident<br />
ischemic stroke<br />
Reduce risk of MI<br />
Reduce Mortality<br />
Improve outcome of patients with or without<br />
ischemic heart disease<br />
Excellent safety profile at high doses over<br />
long periods of 5-11 years
CONCLUSIONS<br />
Use high dose stat<strong>in</strong>s <strong>in</strong> most AIS<br />
Benificts:Reduce mortality, morbidity and<br />
improve survival by reduc<strong>in</strong>g RIS and MI<br />
Monitor<strong>in</strong>g for DM <strong>in</strong> older women<br />
Caution <strong>in</strong> patients with preexist<strong>in</strong>g ICH<br />
Better control of HTN may further reduce<br />
risk of slight excess of ICH seen <strong>in</strong><br />
SPARCL<br />
A randomized trial is needed to settle the question of IHD with<br />
history of prior stroke