

Drug hypersensitivity: questionnaire Special article
Drug hypersensitivity: questionnaire Special article
Drug hypersensitivity: questionnaire Special article

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
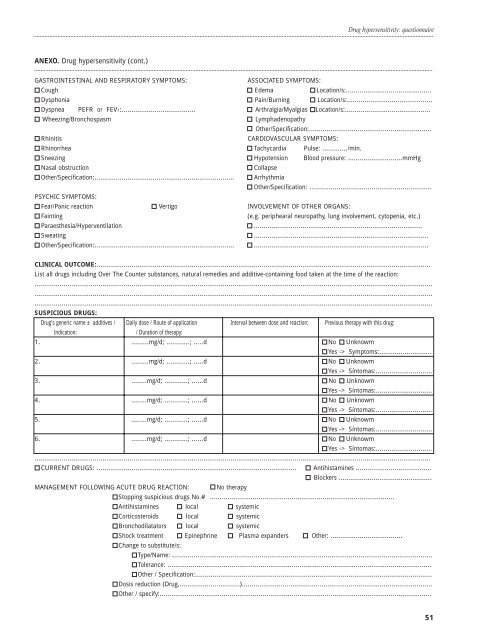
ANEXO. <strong>Drug</strong> <strong>hypersensitivity</strong> (cont.)<br />
<strong>Drug</strong> <strong>hypersensitivity</strong>: <strong>questionnaire</strong><br />
GASTROINTESTINAL AND RESPIRATORY SYMPTOMS: ASSOCIATED SYMPTOMS:<br />
Cough Edema Location/s:............................................<br />
Dysphonia Pain/Burning Location/s:............................................<br />
Dyspnea PEFR or FEV1:...................................... Arthralgia/Myalgias Location/s:............................................<br />
Wheezing/Bronchospasm Lymphadenopathy<br />
Other/Specification:...............................................................<br />
Rhinitis CARDIOVASCULAR SYMPTOMS:<br />
Rhinorrhea Tachycardia Pulse: ............./min.<br />
Sneezing Hypotension Blood pressure: ............................mmHg<br />
Nasal obstruction Collapse<br />
Other/Specification:........................................................................<br />
PSYCHIC SYMPTOMS:<br />
Arrhythmia<br />
Other/Specification: ...............................................................<br />
Fear/Panic reaction Vertigo INVOLVEMENT OF OTHER ORGANS:<br />
Fainting (e.g. periphearal neuropathy, lung involvement, cytopenia, etc.)<br />
Paraesthesia/Hyperventilation .......................................................................................<br />
Sweating ..........................................................................................<br />
Other/Specification:........................................................................ ..........................................................................................<br />
CLINICAL OUTCOME:............................................................................................................................................................................<br />
List all drugs including Over The Counter substances, natural remedies and additive-containing food taken at the time of the reaction:<br />
.............................................................................................................................................................................................................<br />
.............................................................................................................................................................................................................<br />
.............................................................................................................................................................................................................<br />
SUSPICIOUS DRUGS:<br />
<strong>Drug</strong>’s generic name ± additives / Daily dose / Route of application Interval between dose and reaction: Previous therapy with this drug:<br />
Indication: / Duration of therapy:<br />
1. .........mg/d; ............; .....d No Unknowm<br />
Yes -> Symptoms:...........................<br />
2. .........mg/d; ............; .....d No Unknowm<br />
Yes -> Síntomas:.............................<br />
3. ........mg/d; ............; ......d No Unknowm<br />
Yes -> Síntomas:.............................<br />
4. ........mg/d; ............; ......d No Unknowm<br />
Yes -> Síntomas:.............................<br />
5. ........mg/d; ............; ......d No Unknowm<br />
Yes -> Síntomas:.............................<br />
6. ........mg/d; ............; ......d No Unknowm<br />
Yes -> Síntomas:.............................<br />
............................................................................................................................................................................................................<br />
CURRENT DRUGS: .......................................................................................................<br />
MANAGEMENT FOLLOWING ACUTE DRUG REACTION: No therapy<br />
Antihistamines .......................................<br />
Blockers ................................................<br />
Stopping suspicious drugs No.# ...............................................................................................<br />
Antihistamines local systemic<br />
Corticosteroids local systemic<br />
Bronchodilatators local systemic<br />
Shock treatment<br />
Change to substitute/s:<br />
Epinephrine Plasma expanders Other: .....................................<br />
Type/Name: ......................................................................................................................................<br />
Tolerance: ........................................................................................................................................<br />
Other / Specification:..........................................................................................................................<br />
Dosis reduction (<strong>Drug</strong>................................)..................................................................................................<br />
Other / specify:............................................................................................................................................<br />
51














