Dysphagia Screening: Bedside Application and Mechanics of ...
Dysphagia Screening: Bedside Application and Mechanics of ...
Dysphagia Screening: Bedside Application and Mechanics of ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>Dysphagia</strong> <strong>Screening</strong>: <strong>Bedside</strong><br />
<strong>Application</strong> <strong>and</strong> <strong>Mechanics</strong> <strong>of</strong><br />
<strong>Screening</strong> Tools<br />
Jeff Edmiaston, M.S. CCC-SLP<br />
January 31, 2012
Objectives<br />
<strong>Screening</strong> Tool <strong>Mechanics</strong><br />
Specific <strong>Screening</strong> Tools<br />
<strong>Bedside</strong> <strong>Application</strong>
<strong>Screening</strong> in Acute Stroke
+<br />
_________<br />
8
8<br />
+ 0<br />
_________<br />
8
+ + + + +<br />
____ ____ _____ _____ _____<br />
8 8 8 8 8
0 1 2 4 5<br />
+ 8 + 7 + 6 + 4 + 3<br />
____ ____ _____ _____ _____<br />
8 8 8 8 8
What’s in a Screen?<br />
15 Screens Reviewed<br />
38 different components identified<br />
Variation in length<br />
Most Simple-1 Item<br />
Most Complex-16 items
Liquid Trial-93%<br />
Level <strong>of</strong> Alertness-33%<br />
Dysarthria-20%<br />
Aphasia-20%<br />
Facial Symmetry-27%<br />
Tongue Symmetry/Fx-27%<br />
Palatal Fx-20%<br />
Gag-20%<br />
Voluntary Cough-20%<br />
Positioning-7%<br />
Salivary Management-27%<br />
Respiratory Fx-20%<br />
Vocal Quality-27%<br />
Swallowing Complaints-13%<br />
Pulse Oximetry-7%<br />
Stroke Location-7%<br />
Nasal Regurgitation-7%<br />
Eyes Reddening/Tearing-7%<br />
Pneumonia Hx-7%<br />
H/O Coughing with P.O.-20%<br />
Oral Intake (Volume)-7%<br />
Oral Intake (Rate)-7%<br />
NPO Status-7%<br />
Voice after Swallowing-20%<br />
Confusion/Cognitive-7%<br />
Solid Trial-13%<br />
Pharyngeal Sensation-7%<br />
Stroke Severity-7%<br />
Cooperation-7%<br />
Auditory Comprehension-7%<br />
Cough Reflex-13%<br />
Intubation/Recent Extubation-7%<br />
Food Pocketing-7%<br />
Suctioning Required-7%<br />
Other-7%
Specific Screens
3 oz Water Swallow Test<br />
Give patient 3 oz water to drink uninterrupted from a<br />
cup<br />
Observe for 1 minute after the swallow<br />
Coughing<br />
Wet/Hoarse Vocal Quality<br />
*Depippo K, Holas M, Reding M: Validation <strong>of</strong> the 3-oz water swallow test for aspiration following stroke. Arch Neurol. 1992;49:1259-1261<br />
*Suiter D, Leder S.:Clinical utility <strong>of</strong> the 3-ounce water swallow test. <strong>Dysphagia</strong> 2008, 23: 244-250
Burke <strong>Dysphagia</strong><br />
Screen
Burke <strong>Dysphagia</strong> Screen<br />
Pass/Fail<br />
Failure on any one item results in failure<br />
*DePippo K, Holas M, Reding M: The burke dysphagia screening test: validation <strong>of</strong> its use in patients with stroke. Arch Phys Med Rehabil 1994;<br />
75:1284-1286
Massey<br />
<strong>Bedside</strong><br />
Form
Massey <strong>Bedside</strong> <strong>Screening</strong><br />
Complete Pre-Assessment Form<br />
Administer single teaspoon <strong>of</strong> water<br />
60cc glass <strong>of</strong> water<br />
*Massey R, Jedlicka D.: The Massey <strong>Bedside</strong> Swallowing Screen. J. Neurosci Nurs. 2002; 34(5):252-253; 257-260
Timed<br />
Test
Timed Test<br />
GCS >13<br />
Able to sit up<br />
5-10ml <strong>of</strong> water to ensure safety<br />
100-150ml as quickly as possible<br />
Number <strong>of</strong> swallows counted<br />
Timed<br />
Abnormal=outside the 95% prediction interval for age<br />
<strong>and</strong> sex or qualitative elements <strong>of</strong> coughing during or<br />
voice change after the test<br />
*Hinds NP, Wiles CM: Assessment <strong>of</strong> swallowing <strong>and</strong> referral to speech <strong>and</strong> language therapists in acute stroke. QJ Med 1998; 91:829-835
“Any Two”<br />
Administer following liquid bolus amounts:<br />
5ml<br />
10ml<br />
20ml<br />
Administer twice for a total <strong>of</strong> 70ml
“Any Two”<br />
Presence <strong>of</strong> any two <strong>of</strong> the following indicators:<br />
Abnormal volitional cough<br />
Abnormal gag reflex<br />
Dysphonia<br />
Dysarthria<br />
Cough after swallow<br />
Voice changes after swallow<br />
*Daniels S, Lindsay B, Mahoney M, Foundas A: Clinical predictors <strong>of</strong> dysphagia <strong>and</strong> aspiration risk: outcome measures in acute stroke patients.<br />
Arch Phys Med Rehabil 2000; 81: 1030-1033
Barnes Jewish Hospital Stroke <strong>Dysphagia</strong><br />
Screen (BJH-SDS)<br />
5 items, each scored present/absent<br />
Presence <strong>of</strong> one, screen is failed<br />
Failed screen-NPO with speech consult<br />
Passed screen-Regular diet<br />
*Edmiaston J, Tabor Connor L, Loehr L, Nassief A.: Validation <strong>of</strong> a dysphagia screening tool in acute stroke patients. Am J Crit Care, 2010; 19(4): 357-<br />
364.
BJH-SDS
MetroHealth <strong>Dysphagia</strong> Screen<br />
Administered in the Emergency Department<br />
Pass/Fail Criteria<br />
No liquid or solid trials administered
MetroHealth <strong>Dysphagia</strong> Screen<br />
1. Is alertness level insufficient to remain awake for 10 minutes while<br />
sitting upright?<br />
2. Is voice weak, wet, or abnormal in any way? (If cannot speak, circle<br />
yes)<br />
3. Does the patient drool?<br />
4. Is speech slurred?<br />
5. Is the patient’s cough weak or inaudible? (If cannot cough, circle yes)<br />
________________________________________________<br />
One or more “yes” answers are considered a positive screen for possible<br />
dysphagia<br />
*Schrock J, Bernstein J, Glasenapp M, Drogell K, Hanna J.: A novel emergency department dysphagia screen for patients presenting with<br />
acute stroke. Academic Emergency Medicine 2011; 18:584-589
Modified Mann Assessment <strong>of</strong> Swallowing<br />
Ability<br />
No food trials<br />
Scoring system: 0-100<br />
Specific task instructions<br />
Score 95, start oral diet <strong>and</strong> progress as tolerated,<br />
monitor first oral intake. Consult SLP if issues<br />
Score ≤ 94, NPO <strong>and</strong> consult SLP<br />
*Antonios N, Mann G, Crary M, Miller L, Hubbard H, Hood K, Samb<strong>and</strong>am R, Xavier A, Silliman S.: Analysis <strong>of</strong> a physician tool for evaluation<br />
dysphagia on an inpatient stroke unit: The Modifed Mann Assessment <strong>of</strong> Swallowing Ability. Journal <strong>of</strong> Stroke <strong>and</strong> Cerebrovascular Diseases; 2010<br />
19(1): 49-57.
Original Mann Assessment <strong>of</strong> Swallowing Ability<br />
Mann Assessment <strong>of</strong> Swallowing Ability<br />
Alertness 2=No response<br />
to speech<br />
Cooperation 2= No<br />
cooperation<br />
Auditory<br />
Comprehension<br />
2=No response<br />
to speech<br />
Respiration 2=Chest<br />
infection<br />
Respiratory rate<br />
for swallow<br />
1=No independent<br />
control<br />
Aphasia 1=Unable to<br />
assess<br />
Apraxia 1=Unable to<br />
assess<br />
Dysarthria 1=Unable to<br />
assess<br />
5=Difficult<br />
to rouse<br />
Patient Name:_________________________Date:_________________SLP:_______________________<br />
MASA #:_____________ Score:_______________<br />
5=Reluctant 8=Fluctuating<br />
cooperation<br />
4=Occasional<br />
motor response<br />
4=Coarse basal<br />
crepitations<br />
3=Some control<br />
uncoordinated<br />
2=No functional<br />
speech<br />
8=Fluctuates 10=Alert<br />
6=follows simple<br />
conversation<br />
with repetition<br />
6=Fine basal<br />
crepitations<br />
3=Expresses self<br />
in limited manner<br />
short phrase/words<br />
2=Groping/ 3=Speech crude.<br />
inaccurate/partial defective in<br />
or irrelevant response accuracy or speed<br />
2=Speech<br />
unintelligible<br />
Saliva 1=Gross drool 2=Some drool<br />
consistently<br />
Lip seal 1=No closure<br />
unable to assess<br />
Tongue<br />
movement<br />
Tongue<br />
strength<br />
Tongue<br />
coordination<br />
2=Incomplete<br />
seal<br />
2=No movement 4=Minimal<br />
movement<br />
2=Gross<br />
weakness<br />
2=No movement<br />
unable to assess<br />
5=Unilateral<br />
weakness<br />
5=Gross<br />
incoordination<br />
10=<br />
Cooperative<br />
8=follows<br />
10=No deficits<br />
ordinary conversation with noted<br />
little difficulty<br />
8=Sputum in upper<br />
airway<br />
5=Able to control<br />
rate for swallow<br />
4=Mild difficulty<br />
finding words or<br />
expressing ideas<br />
4=Speech accurate<br />
after trial <strong>and</strong> error<br />
Minor searching<br />
movements<br />
3=Speech intelligible 4=Slow with<br />
but obvious defect occasional halting<br />
3=Drooling at<br />
times<br />
3=Unilaterally weak<br />
poor maintenance<br />
6=Incomplete<br />
movement<br />
8=Minimal<br />
weakness<br />
8=Mild<br />
incoordination<br />
4=Frothy/<br />
expectorated<br />
4=Mild impairment<br />
occasional leakage<br />
8=Mild impairment<br />
in range<br />
10=No deficits<br />
noted<br />
10=No deficits<br />
noted<br />
10=Chest<br />
clear<br />
5=No deficits<br />
noted<br />
5=No deficits<br />
noted<br />
5=No deficits<br />
noted<br />
5=No deficits<br />
noted<br />
5=No deficits<br />
noted<br />
10=Full range<br />
<strong>of</strong> motion<br />
Oral<br />
2=Unable to 4=No bolus 6=Minimal chew, 8=Lip or tongue 10=No deficits<br />
preparation<br />
assess<br />
formation, no attempt gravity assisted seal, bolus escape noted<br />
Gag 1=No gag 2=Absent<br />
3=Diminished 4=Diminished 5=Hyperreflexive<br />
unilaterally unilaterally bilaterally<br />
No deficits<br />
Palate 2=No spread 4=Minimal 6=Unilateral 8=Slight<br />
10=No deficits<br />
or elevation movement weakness<br />
asymmetry noted<br />
Bolus clearance 2=No clearance 5=Some<br />
8=Significant clearance 10=Fully<br />
clearance/residue minimal residue<br />
cleared<br />
Oral transit 2=No movement 4=Delay >10 sec. 6=Delay >5 sec 8=Delay >1 sec 10=No deficit<br />
Cough reflex 1=Unable to assess 3=Weak reflexive<br />
5=No deficit<br />
cough<br />
noted<br />
Voluntary<br />
2=No attempt<br />
cough<br />
Voice 2=Aphonic, not<br />
able to assess<br />
5=Attempt<br />
inadequate<br />
8=Attempt<br />
bovine<br />
4=Wet/gurgling 6=Hoarse 8=Mild impairment<br />
slight huskiness<br />
Trach 1=Trach/cuffed 5=Trach/fenestrated 10=No trach<br />
Pharyngeal<br />
phase<br />
Pharyngeal<br />
response<br />
2=No swallow 5=Pooling/gurgling<br />
Incomplete laryngeal<br />
elevation<br />
1=Not coping/<br />
gurgling<br />
5=Cough before<br />
during<br />
or after swallow<br />
8=Mildly restricted<br />
laryngeal elevation<br />
Slow initiation<br />
10=No deficit<br />
noted<br />
10=No deficit<br />
noted<br />
10=No deficit<br />
noted<br />
10=Immediate<br />
laryngeal elevation<br />
Diet recommendations Regular S<strong>of</strong>t Selected s<strong>of</strong>t Mechanical s<strong>of</strong>t Puree No solid<br />
by mouth<br />
Fluid recommendation Regular Thins only Nectar Honey No liquids by mouth
Alertness 10=Alert 8=Drowsy-fluctuating<br />
awareness/alert level<br />
Cooperation 10=Cooperative 8=Fluctuating<br />
cooperation<br />
Respiration 10=Chest clear 8=Sputum in upper<br />
airway<br />
Expressive<br />
Dysphasia<br />
Auditory<br />
Comprehension<br />
Modified Mann Assessment <strong>of</strong> Swallowing Ability<br />
5=No abnormality 4=Mild wording finding<br />
difficulty<br />
10=No abnormality 8=Follows ordinary<br />
conversation with<br />
little difficulty<br />
Dysarthria 5=No abnormality 4=Slow with<br />
occasional hesitation<br />
Saliva 5=No abnormality 4=Frothy/<br />
expectorated in cup<br />
5=Difficult to arouse<br />
by speech or mvmt<br />
5=Reluctant<br />
cooperation<br />
6=Fine basal<br />
crepitations<br />
3=Expresses self in<br />
limited manner<br />
6=Follows simple<br />
conversation<br />
3=Speech intelligible<br />
but defective<br />
2=Coma or<br />
nonresponsvie<br />
2=No cooperation/<br />
response<br />
4=Coarse basal<br />
crepitations<br />
2=No functional<br />
speech<br />
4=Occasional<br />
response<br />
3=Drooling at times 2=Some drool<br />
consistently<br />
2=Suspected<br />
infections/ freq<br />
suction/ respirator<br />
dependent<br />
1=Unable to assess<br />
1=No response<br />
2=Speech unintelligible 1=Unable to assess<br />
1=Gross drooling<br />
Tongue Movement 10=Full R.O.M. 8=Mild impairment 6=Incomplete mvmt 4=Minimal mvmt 2=No movement<br />
Tongue Strength 10=No abnormality 8=Minimal weakness 5=Obvious unilateral<br />
weakness<br />
Gag 5=No abnormality 4=Diminished<br />
bilaterally<br />
Cough Reflex 10-No abnormality 8=Cough attempted<br />
but hoarse in quality<br />
3=Diminished<br />
unilaterally<br />
2=Gross weakness<br />
5=Attempt inadequate 2=No attempt/unable<br />
to perform<br />
2=Absent unilaterally 1=No gag response<br />
Palate 10=No abnormality 8=Slight asymmetry 6=Unilaterally weak 4=Minimal movement 2=No movement
EATS<br />
• Two Phases<br />
Questionnaire<br />
Food/Liquid Trials<br />
• Must show no deficits in both phases to pass screen<br />
Courtney B, Flier L.: RN dysphagia screening, a stepwise approach. Journal <strong>of</strong> Neuroscience Nursing 2009; 41(1):28-38
EATS
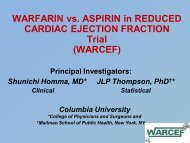
The Gugging Swallow Screen<br />
Includes a semi-solid, liquid, <strong>and</strong> solid trial<br />
Severity scoring system<br />
Allows diet to be altered
Copyright © American Heart Association<br />
Figure I. GUSS.<br />
Trapl M et al. Stroke 2007;38:2948-2952
Trapl M et al. Stroke 2007;38:2948-2952<br />
Copyright © American Heart Association<br />
Figure I Continued.
What Screen Should I Use?
+ + + + +<br />
____ ____ _____ _____ _____<br />
8 8 8 8 8
0 1 2 4 5<br />
+ 8 + 7 + 6 + 4 + 3<br />
____ ____ _____ _____ _____<br />
8 8 8 8 8
Use only odd numbers to answer the question<br />
+ + + + +<br />
____ ____ _____ _____ _____<br />
8 8 8 8 8
Use only odd numbers to answer the question<br />
+ +<br />
_____ _____<br />
8 8
Use only odd numbers to answer the question<br />
5 1<br />
+ 3 + 7<br />
_____ _____<br />
8 8
<strong>Screening</strong> Purpose<br />
Identify individuals with or at risk <strong>of</strong> swallowing<br />
dysfunction following a stroke.
Sensitivity vs. Specificity<br />
Always a trade-<strong>of</strong>f<br />
<strong>Dysphagia</strong> screening is tilted towards sensitivity
The Perfect Screen<br />
Do you have stroke-like<br />
symptoms?
The Perfect Screen<br />
100% Sensitivity to <strong>Dysphagia</strong><br />
0% Specificity to <strong>Dysphagia</strong><br />
Theoretical Result: Never a dysphagia related<br />
complication<br />
<strong>Bedside</strong> Result<br />
6 out <strong>of</strong> 10 patients are angry!
Not all bedsides are the same
BJC Healthcare<br />
1. Alton Memorial<br />
2. Barnes Jewish<br />
3. Barnes Jewish St. Peters<br />
4. Barnes Jewish West County<br />
5. Boone Hospital<br />
6. Christian Hospital<br />
7. Clay County Hospital<br />
8. Missouri Baptist Medical Center<br />
9. Missouri Baptist Sullivan Hospital<br />
10. Northwest Healthcare<br />
11. Parkl<strong>and</strong> Health Center<br />
12. Progress West HealthCare Center<br />
13. Rehabilitation Institute <strong>of</strong> St. Louis<br />
14. St. Louis Children’s Hospital<br />
15. Siteman Cancer Center
Barnes Jewish Hospital
Stroke Fellow<br />
Neuroradiology & Neurosurgery<br />
MRI, Angiography, PET Scanner<br />
Dedicated Stroke Neurologists<br />
Dedicated Stroke Nursing Unit<br />
Dedicated 20 Bed Neuro-ICU with Portable CT<br />
Intra-operative MRI Suite<br />
Two Stroke Nursing Coordinators<br />
Dedicated Stroke Rehabilitation Services (PT,OT, <strong>and</strong><br />
Speech)<br />
Administrative group dedicated to Neurosciences
Clay County Hospital
Factors that may effect screen choice<br />
Availability <strong>of</strong> Speech Pathology<br />
Availability <strong>of</strong> Radiology Services (i.e. Vide<strong>of</strong>luoroscopy)<br />
Volume <strong>of</strong> patients<br />
Nursing numbers
Fewer Resources Available<br />
May be less tolerant <strong>of</strong> false positives<br />
May be more comprehensive<br />
May resemble an assessment rather than screen<br />
Potentially more burden on nursing
More Resources Available<br />
May tolerate false positives<br />
May be less comprehensive (pass/fail)<br />
Potentially less burden on nursing
No Perfect Screen<br />
Perfection= 100% Sensitivity & 100% Specificity<br />
There will be false positives<br />
There will be false negatives<br />
How many <strong>of</strong> each can be tolerated?
What is a good Screen?<br />
Valid<br />
Reliable<br />
Works for your setting
Validity<br />
External<br />
Internal<br />
Criterion<br />
Content<br />
Concurrent<br />
Predictive<br />
Content<br />
Construct<br />
Face
Reliability<br />
Inter-rater Reliability<br />
Test-Retest Reliability<br />
Parallel-Forms Reliability<br />
Internal Consistency
What Works for You?<br />
No numeric value to derive this<br />
Dependent on multiple factors<br />
Specific to a given institution
Making a Decision<br />
Expert Opinion<br />
Data Driven-Dependent on quality <strong>of</strong> data<br />
Group Consensus<br />
Kepner-Tregoe Decision Matrix
Kepner-Tregoe Decision Matrix<br />
Easily<br />
Administered<br />
Valid<br />
Reliable<br />
Easily<br />
Documented<br />
Sensitivity/Spec<br />
ificity (5)<br />
Evidence Based<br />
(10)<br />
Timed Up<br />
<strong>and</strong> Go<br />
Timed Up<br />
<strong>and</strong> Go (R)<br />
Get Up <strong>and</strong><br />
Go<br />
BJC Get Up<br />
<strong>and</strong> Go
Kepner-Tregoe Decision Matrix<br />
Easily<br />
Administered<br />
Timed Up<br />
<strong>and</strong> Go<br />
Timed Up<br />
<strong>and</strong> Go (R)<br />
Get Up <strong>and</strong><br />
Go<br />
BJC Get Up<br />
<strong>and</strong> Go<br />
x x x<br />
Valid x x X X<br />
Reliable x x<br />
Easily<br />
Documented<br />
Sensitivity/Spec<br />
ificity (5)<br />
Evidence Based<br />
(10)<br />
x x x x<br />
5 5 5<br />
10 10 10 10
Sensitivity<br />
>90%<br />
Face Validity<br />
Easy to<br />
administer<br />
Reliable<br />
Concurrent<br />
Validity<br />
Scoring<br />
Severity<br />
Easy to learn<br />
Specificity<br />
>50%<br />
3 oz<br />
water<br />
K-T Analysis <strong>of</strong> Swallow Screens<br />
Massey Timed<br />
Test<br />
Burke<br />
Screen<br />
Metro<br />
Health<br />
Any<br />
Two<br />
EATS Mini<br />
MASA<br />
GUSS BJH<br />
SDS
Barnes Jewish Hospital- KT Matrix
Sensitivity<br />
>90%<br />
Face Validity<br />
Easy to<br />
administer<br />
Reliable<br />
Concurrent<br />
Validity (8)<br />
Scoring<br />
Severity (1)<br />
Easy to<br />
learn (10)<br />
Specificity<br />
>50% (5)<br />
3 oz<br />
water<br />
Massey Timed<br />
Test<br />
Burke<br />
Screen<br />
Metro<br />
Health<br />
Any<br />
Two<br />
EATS Mini<br />
MASA<br />
GUSS BJH<br />
SDS
3 oz<br />
water<br />
Massey Timed<br />
Test<br />
Burke<br />
Screen<br />
Metro<br />
Health<br />
Any<br />
Two<br />
EATS Mini<br />
MASA<br />
GUSS BJH<br />
SDS<br />
Sensitivity<br />
>90% X X X X X X X X X X<br />
Face Validity<br />
X X X X X X X X<br />
Easy to<br />
administer X X X X X X X<br />
Reliable<br />
Concurrent<br />
Validity (8)<br />
Scoring<br />
Severity (1)<br />
Easy to learn<br />
(10)<br />
Specificity<br />
>50% (5)<br />
X X X X X X X X X X
Sensitivity >90%<br />
Face Validity<br />
Easy to administer<br />
Reliable<br />
Concurrent<br />
Validity with<br />
MBS/FEES (8)<br />
Massey Timed Test<br />
Burke<br />
Screen<br />
Any Two BJH SDS<br />
X X X X X<br />
X X X X X<br />
X X X X X<br />
X X X X X<br />
0 0 0 8 8<br />
Scoring Severity<br />
(1) 0 0 0 0 0<br />
Easy to learn (10)<br />
10 10 10 10 10<br />
Specificity<br />
>50% (5) 5 5 0 5 5<br />
TOTAL 15 15 10 23 23
Clay County Hospital-KT Matrix
Sensitivity<br />
>90%<br />
Face<br />
Validity<br />
Easy to<br />
learn<br />
Specificity<br />
>50%<br />
Reliable<br />
Concurren<br />
t Validity<br />
Scoring<br />
Severity<br />
Easy to<br />
administer<br />
3 oz<br />
water<br />
Massey Timed<br />
Test<br />
Burke<br />
Screen<br />
Metro<br />
Health<br />
Any<br />
Two<br />
EATS Mini<br />
MASA<br />
GUSS BJH<br />
SDS
3 oz<br />
water<br />
Massey Timed<br />
Test<br />
Burke<br />
Screen<br />
Metro<br />
Health<br />
Any<br />
Two<br />
EATS Mini<br />
MASA<br />
GUSS BJH<br />
SDS<br />
Sensitivity<br />
>90% X X X X X X X X X<br />
Face Validity X X X X X X X X X X<br />
Easy to learn X X X X X X X X X X<br />
Specificity<br />
>50% X X X X X X X<br />
Reliable<br />
Concurrent<br />
Validity<br />
Scoring<br />
Severity<br />
Easy to<br />
administer
Sensitivity >90%<br />
Face Validity<br />
Easy to learn<br />
Massey<br />
Timed<br />
Test<br />
Metro<br />
Health<br />
Any<br />
Two<br />
Mini<br />
MASA<br />
GUSS<br />
BJH<br />
SDS<br />
X X X X X X X<br />
X X X X X X X<br />
X X X X X X X<br />
Specificity<br />
>50% X X X X X X X<br />
Reliable (2)<br />
2 2 2 2 2 2 2<br />
Concurrent Validity<br />
with MBS/FEES (10) 0 0 10 10 10 10 10<br />
Scoring Severity (8)<br />
0 0 0 0 0 8 0<br />
Easy to administer<br />
(4) 4 4 4 4 4 0 4<br />
TOTAL 6 6 16 16 16 20 16
Conclusion<br />
Much research has been done<br />
Many screens, most are pretty good<br />
When choosing a screen, be objective <strong>and</strong> systematic<br />
There is no “best” screen<br />
The best screen is the one that is best for your institution