Unusual endoscopic appearance of Crohn's disease ... - Publicatio
Unusual endoscopic appearance of Crohn's disease ... - Publicatio
Unusual endoscopic appearance of Crohn's disease ... - Publicatio

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
LETTER TO THE EDITOR<br />
<strong>Unusual</strong> Endoscopic<br />
Appearance <strong>of</strong> Crohn’s<br />
Disease: Another Face <strong>of</strong><br />
a Multifaceted Disease<br />
To the Editor:<br />
Crohn’s <strong>disease</strong> (CD) is a clinically<br />
heterogeneous condition, with various<br />
clinical presentations in different<br />
patients. Endoscopic and transsectional<br />
radiological imaging remains the mainstay<br />
<strong>of</strong> evaluation and management <strong>of</strong><br />
the <strong>disease</strong>. The most characteristic<br />
(‘‘elementary’’) <strong>endoscopic</strong> lesions <strong>of</strong><br />
CD are pseudopolyp, healed ulceration,<br />
frank erythema, frankly swollen<br />
mucosa, aphthoid ulceration, superficial<br />
or swallow ulceration, deep ulceration,<br />
and nonulcerated or ulcerated stenosis. 1<br />
Although the most frequently observed<br />
location <strong>of</strong> CD is the ileum and the<br />
right side <strong>of</strong> the colon, a solely cecal<br />
location with a tumor-like <strong>endoscopic</strong><br />
feature has never been described in the<br />
literature.<br />
A 27-year-old female was admitted<br />
to our clinic in September 2010<br />
with 2 weeks history <strong>of</strong> right lower<br />
abdominal pain, nausea, and two loose<br />
stools daily. Her medical history was<br />
remarkable for an appendectomy in<br />
2008. On physical examination mild<br />
ileocecal tenderness was observed. The<br />
laboratory findings showed a moderately<br />
elevated C-reactive protein level<br />
<strong>of</strong> 49.7 mg/L and erythrocyte sedimentation<br />
rate <strong>of</strong> 36 mm/h. Abdominal<br />
ultrasonography included wall thickening<br />
<strong>of</strong> the cecum with enlarged lymph<br />
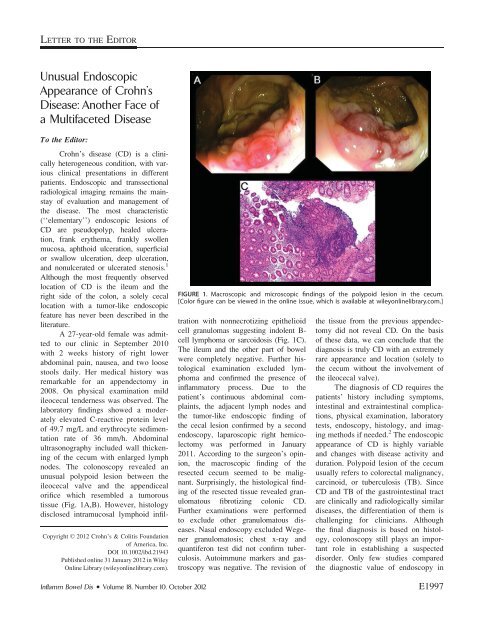
nodes. The colonoscopy revealed an<br />
unusual polypoid lesion between the<br />
ileocecal valve and the appendiceal<br />
orifice which resembled a tumorous<br />
tissue (Fig. 1A,B). However, histology<br />
disclosed intramucosal lymphoid infil-<br />
Copyright VC 2012 Crohn’s & Colitis Foundation<br />
<strong>of</strong> America, Inc.<br />
DOI 10.1002/ibd.21943<br />
Published online 31 January 2012 in Wiley<br />
Online Library (wileyonlinelibrary.com).<br />
FIGURE 1. Macroscopic and microscopic findings <strong>of</strong> the polypoid lesion in the cecum.<br />
[Color figure can be viewed in the online issue, which is available at wileyonlinelibrary.com.]<br />
tration with nonnecrotizing epithelioid<br />
cell granulomas suggesting indolent Bcell<br />
lymphoma or sarcoidosis (Fig. 1C).<br />
The ileum and the other part <strong>of</strong> bowel<br />
were completely negative. Further histological<br />
examination excluded lymphoma<br />
and confirmed the presence <strong>of</strong><br />
inflammatory process. Due to the<br />
patient’s continuous abdominal complaints,<br />
the adjacent lymph nodes and<br />
the tumor-like <strong>endoscopic</strong> finding <strong>of</strong><br />
the cecal lesion confirmed by a second<br />
endoscopy, laparoscopic right hemicolectomy<br />
was performed in January<br />
2011. According to the surgeon’s opinion,<br />
the macroscopic finding <strong>of</strong> the<br />
resected cecum seemed to be malignant.<br />
Surprisingly, the histological finding<br />
<strong>of</strong> the resected tissue revealed granulomatous<br />
fibrotizing colonic CD.<br />
Further examinations were performed<br />
to exclude other granulomatous <strong>disease</strong>s.<br />
Nasal endoscopy excluded Wegener<br />
granulomatosis; chest x-ray and<br />
quantiferon test did not confirm tuberculosis.<br />
Autoimmune markers and gastroscopy<br />
was negative. The revision <strong>of</strong><br />
the tissue from the previous appendectomy<br />
did not reveal CD. On the basis<br />
<strong>of</strong> these data, we can conclude that the<br />
diagnosis is truly CD with an extremely<br />
rare <strong>appearance</strong> and location (solely to<br />
the cecum without the involvement <strong>of</strong><br />
the ileocecal valve).<br />
The diagnosis <strong>of</strong> CD requires the<br />
patients’ history including symptoms,<br />
intestinal and extraintestinal complications,<br />
physical examination, laboratory<br />
tests, endoscopy, histology, and imaging<br />
methods if needed. 2 The <strong>endoscopic</strong><br />
<strong>appearance</strong> <strong>of</strong> CD is highly variable<br />
and changes with <strong>disease</strong> activity and<br />
duration. Polypoid lesion <strong>of</strong> the cecum<br />
usually refers to colorectal malignancy,<br />
carcinoid, or tuberculosis (TB). Since<br />
CD and TB <strong>of</strong> the gastrointestinal tract<br />
are clinically and radiologically similar<br />
<strong>disease</strong>s, the differentiation <strong>of</strong> them is<br />
challenging for clinicians. Although<br />
the final diagnosis is based on histology,<br />
colonoscopy still plays an important<br />
role in establishing a suspected<br />
disorder. Only few studies compared<br />
the diagnostic value <strong>of</strong> endoscopy in<br />
Inflamm Bowel Dis Volume 18, Number 10, October 2012 E1997
Farkas et al<br />
CD and intestinal TB. One <strong>of</strong> them<br />
found that anorectal lesions, longitudinal<br />
ulcers, aphthous ulcers, and a cobblestone<br />
<strong>appearance</strong> are significantly<br />
more common in CD, and involvement<br />
<strong>of</strong> fewer than four segments, a patulous<br />
ileocecal valve, transverse ulcers,<br />
and pseudopolyps were more frequent<br />
in intestinal TB. 3 The study <strong>of</strong> Makharia<br />
et al 4 revealed that skip lesions <strong>of</strong><br />
the colon (66% vs. 16.9%, P < 0.001),<br />
aphthous ulceration (54.7% vs. 13.2%,<br />
P < 0.001), linear ulceration (30.1%<br />
vs. 7.5%, P ¼ 0.005), and superficial<br />
ulceration (50.9% vs. 16.9%, P <<br />
0.001) were significantly more frequent<br />
in patients with CD compared to<br />
patients with intestinal TB. Cobblestoning<br />
<strong>of</strong> the colonic mucosa was<br />
only seen in CD (16.9% vs. 0%, P <<br />
0.001). Nodularity <strong>of</strong> the colonic<br />
mucosa was significantly more common<br />
in patients with TB than in those<br />
E1998<br />
with CD (49% vs. 24.5%, P ¼ 0.01).<br />
According to this study, colonic<br />
involvement was significantly more<br />
common in CD than in TB; however,<br />
there was no difference in the ileal or<br />
ileocolonic locations. In our case, the <strong>endoscopic</strong><br />
<strong>appearance</strong> <strong>of</strong> the cecum suggested<br />
most likely colonic tumor or intestinal<br />
TB and least likely CD, since<br />
none <strong>of</strong> the abovementioned diagnostic<br />
<strong>endoscopic</strong> findings were detected. Such<br />
an unusual macroscopic <strong>appearance</strong> <strong>of</strong><br />
CD has not been published before.<br />
Klaudia Farkas, MD, PhD*<br />
György Lazar, MD, PhD †<br />
Laszlo Tiszlavicz, MD, PhD ‡<br />
Laszlo Krenacs, MD, PhD §<br />
Ferenc Nagy, MD, PhD*<br />
Zoltan Szepes, MD, PhD*<br />
Tibor Wittmann, MD, PhD*<br />
Tamás Molnár, MD, PhD*<br />
Inflamm Bowel Dis Volume 18, Number 10, October 2012<br />
*First Department <strong>of</strong> Medicine<br />
University <strong>of</strong> Szeged, Szeged, Hungary<br />
† Department <strong>of</strong> Surgery<br />
University <strong>of</strong> Szeged, Szeged, Hungary<br />
‡ Department <strong>of</strong> Pathology<br />
University <strong>of</strong> Szeged, Szeged, Hungary<br />
§ Second Department <strong>of</strong> Medicine<br />
University <strong>of</strong> Szeged, Szeged, Hungary<br />
REFERENCES<br />
1. Mary JY, Modigliani R. Development and<br />
validation <strong>of</strong> an <strong>endoscopic</strong> index <strong>of</strong> the severity<br />
for Crohn’s <strong>disease</strong>: a prospective multicentre<br />
study. Gut. 1989;30:983–989.<br />
2. Bernstein CN, Fried M, Krabshuis JH, et al.<br />
World Gastroenterology Organization practice<br />
guidelines for the diagnosis and management<br />
<strong>of</strong> IBD in 2010. Inflamm Bowel Dis. 2010;16:<br />
112–124.<br />
3. Lee YJ, Yang SK, Byeon JS, et al. Analysis <strong>of</strong><br />
colonoscopic findings in the differential diagnosis<br />
between intestinal tuberculosis and Crohn’s<br />
<strong>disease</strong>. Endoscopy. 2006;38:592–597.<br />
4. Makharia GK, Srivastava S, Das P, et al. Clinical,<br />
<strong>endoscopic</strong>, and histological differentiations<br />
between Crohn’s <strong>disease</strong> and intestinal tuberculosis.<br />
Am J Gastroenterol. 2010;105:642–651.