Inflating Characteristics of Swan-Ganz Catheter Balloons: Clinical ...
Inflating Characteristics of Swan-Ganz Catheter Balloons: Clinical ...
Inflating Characteristics of Swan-Ganz Catheter Balloons: Clinical ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>Inflating</strong> <strong>Characteristics</strong> <strong>of</strong> <strong>Swan</strong>-<strong>Ganz</strong> <strong>Catheter</strong> <strong>Balloons</strong>:<br />
<strong>Clinical</strong> Considerations<br />
Jean Francois Hardy, MD, and Jean Taillefer, MD<br />
The dangers associated with overdistension <strong>of</strong> bal-<br />
loon-tipped pulmonary arterial catheters are well<br />
known. A patient was brought to the operating room<br />
for emergency coronary artery bypass graft with a<br />
femorally inserted balloon-tipped pulmonary artery<br />
catheter. We wondered if some form <strong>of</strong> extension tub-<br />
ing could be used to inflate the balloon intraopera-<br />
tively to monitor the wedge pressure because the in-<br />
flating site is out <strong>of</strong> reach. This prompted us to<br />
undertake the present in vitro study <strong>of</strong> the inflating<br />
characteristics <strong>of</strong> the balloon <strong>of</strong> the pulmonary arterial<br />
catheter and to determine if it is possible to safely use<br />
extension tubings for these procedures.<br />
Materials and Methods<br />
We studied six used but not resterilized balloon-tipped<br />
pulmonary arterial catheters (three 93A-131-7F ther-<br />
modilution and three 93-114-7F monitoring <strong>Swan</strong>-<br />
<strong>Ganz</strong> catheters by Edwards Corporation). Using a<br />
standard 3-ml syringe, we inflated the balloon with<br />
1.5 ml <strong>of</strong> room-temperature air. We determined the<br />
critical volume <strong>of</strong> air, i.e., the volume at which max-<br />
imal resistance was felt just before balloon inflation<br />
began, and the diameter <strong>of</strong> the completely inflated<br />
balloon with a Vernier scale. We repeated the mea-<br />
surements using 32.5-cm (Cobe pressure monitoring<br />
tubing 40-101-001) and 183-cm (Cobe pressure mon-<br />
itoring tubing 40-10&001) rigid extension tubing fixed<br />
to the inflating port <strong>of</strong> the balloon. We verified the<br />
reproducibility <strong>of</strong> the measurements with a brand-<br />
new catheter.<br />
The internal volume <strong>of</strong> all tubings and stopcocks<br />
was measured by fluid filling: the average internal<br />
volume <strong>of</strong> the pulmonary arterial catheter inflating<br />
lumen was 0.4 ml, the short extension tubing 0.8 ml,<br />
Received from the Montreal Heart Institute, 5000 East Belanger<br />
Street, Montreal, Quebec, Canada, HIT 1C8. Accepted for publi-<br />
cation October 1, 1982.<br />
Address correspondence to Dr. Taillefer.<br />
8 1983 by the International Anesthesia Research Society<br />
ANESTH ANALG 363<br />
1983;62: 363-4<br />
the long tubing 4.6 ml, and the stopcock 0.35 ml. The<br />
volume <strong>of</strong> balloon-tipped pulmonary arterial cathe-<br />
ters was measured by fluid immersion (Archimedes’<br />
principle).<br />
The pressure-volume curve <strong>of</strong> a typical catheter<br />
was determined using an appropriately calibrated<br />
pressure transducer (Bentley Trantec model 800).<br />
Finally, the measured volumes were compared with<br />
the theoretical critical volume (using Boyle’s law), the-<br />
oretical inflating volume, and balloon volume in order<br />
to cross-check our results.<br />
Results<br />
Without extension tubing, 0.75 ml <strong>of</strong> air consistently<br />
initiated inflation <strong>of</strong> the balloon (Table 1) compared<br />
to 1.2 2 0.1 ml with the short tubing (Table 2) and<br />
3.25 5 0.25 ml with the long one (Table 3). The in-<br />
flated balloon had a volume <strong>of</strong> 1.0 ml using the stan-<br />
dard technique with the short extension set, and 1.1<br />
ml using the long one.<br />
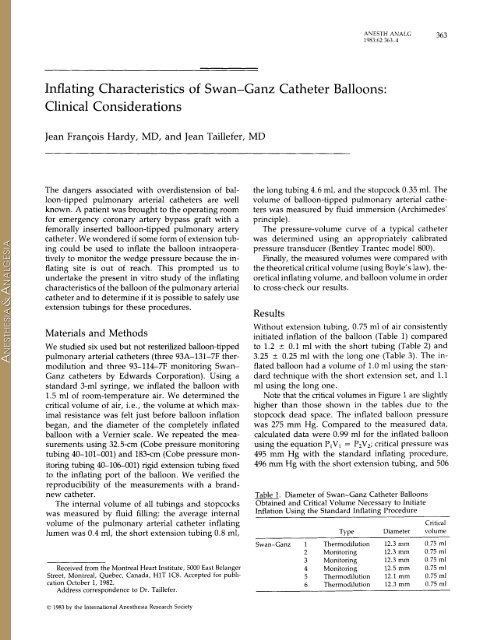
Note that the critical volumes in Figure 1 are slightly<br />
higher than those shown in the tables due to the<br />
stopcock dead space. The inflated balloon pressure<br />
was 275 mm Hg. Compared to the measured data,<br />
calculated data were 0.99 ml for the inflated balloon<br />
using the equation P,Vl = P,V,; critical pressure was<br />
495 mm Hg with the standard inflating procedure,<br />
496 mm Hg with the short extension tubing, and 506<br />
Table 1. Diameter <strong>of</strong> <strong>Swan</strong>-<strong>Ganz</strong> <strong>Catheter</strong> <strong>Balloons</strong><br />
Obtained and Critical Volume Necessary to Initiate<br />
Inflation Using the Standard <strong>Inflating</strong> Procedure<br />
Type<br />
Diameter<br />
<strong>Swan</strong>-<strong>Ganz</strong> 1 Thermodilution 12.3 mm<br />
2 Monitoring 12.3 mm<br />
3 Monitoring 12.3 mm<br />
4 Monitoring 12.5 mm<br />
5 Thermodilution 12.1 mm<br />
6 Thermodilution 12.3 mm<br />
Critical<br />
volume<br />
0.75 ml<br />
0.75 ml<br />
0.75 ml<br />
0.75 ml<br />
0.75 ml<br />
0.75 nil
364 ANESTH ANALG<br />
1983;62:363-4<br />
Table 2. <strong>Inflating</strong> Volume and Critical Volume Using a<br />
32.5-cm Extension Tube<br />
~~<br />
Diameter with<br />
<strong>Inflating</strong> Critical standard<br />
volume volume inflation<br />
<strong>Swan</strong>-<strong>Ganz</strong> 1 1.8 ml 1.3 ml 11.3 mm<br />
2 1.7 ml 1.1 ml 11.8 mm<br />
3 1.7 ml 1.1 ml 11.5 mm<br />
4 1.7 ml 1.1 ml 11.5 mm<br />
5 1.7 ml 1.1 ml 11.7 mm<br />
6 1.7 ml 1.2 ml 11.3 mm<br />
Last column is the diameter obtained with an inflating volume <strong>of</strong> 1.5 ml.<br />
mm Hg with the long one. The theoretical volume<br />
required to inflate the balloon to its normal 0.99-ml<br />
capacity at 275 mm Hg is 1.8 ml with the short ex-<br />
tension and 3.17 ml with the long one. The internal<br />
volume <strong>of</strong> the extension set at which the inflation<br />
volume is equal to the critical volume was calculated<br />
at 4.16 ml.<br />
Discussion<br />
The diameters obtained using the standard inflation<br />
technique were quite uniform (12.2 5 0.2 mm) and<br />
comparable to the specifications listed in the manu-<br />
facturer’s leaflet (13 mm) (1); we were impressed with<br />
the high reproducibility <strong>of</strong> the measurements.<br />
Very high pressures are necessary to initiate the<br />
inflation <strong>of</strong> the balloon (k 500 mm Hg). When the<br />
inflation is completed the pressure inside the balloon<br />
drops to 275 mm Hg, which is in accordance with<br />
previous reports (2,3), but to our knowledge these<br />
high inflation pressures have not been reported before.<br />
When the short extension set is used, the critical<br />
volume is reasonably less than the inflating volume.<br />
The measured and the calculated inflating volumes<br />
Table 3. <strong>Inflating</strong> Volume and Critical Volume Using a<br />
183-cm Extension Tube<br />
<strong>Inflating</strong> Critical<br />
volume volume<br />
<strong>Swan</strong>-<strong>Ganz</strong> 1 3.3 ml 3.0 ml<br />
2 3.5 ml 3.4 ml<br />
3 3.5 ml 3.3 ml<br />
4 3.5 ml 3.3 ml<br />
5 3.5 ml 3.5 ml<br />
6 3:5 ml 3.5 mi<br />
Diameter with<br />
standard<br />
inflation<br />
8F<br />
8F<br />
8F<br />
8F<br />
8F<br />
8F<br />
mmHg<br />
500 1<br />
CLINICAL REPORTS<br />
PRESSURE - VOLUME CURVE VARIATION<br />
ACCORDING TO THREE DIFFERENT TUBING LENGTHS<br />
joow<br />
:/<br />
, I , ,<br />
/<br />
0<br />
0 1 2 3 4 cm3<br />
Figure 1. Pressure-volume curve variation using three different<br />
lengths <strong>of</strong> tubing.<br />
are identical. However, when using the long exten-<br />
sion set, the critical volume is usually equal or slightly<br />
less than the inflation volume. Furthermore, the cal-<br />
culated inflation volume is smaller than the measured<br />
critical volume meaning that overinflation is inevitable.<br />
We can draw three conclusions from the data.<br />
1. Physicians using balloon-tipped pulmonary arterial<br />
catheters must realize that they can generate<br />
very high pressures (2500 mm Hg) with the simple<br />
compression <strong>of</strong> 1.5 ml <strong>of</strong> air. These can lead to<br />
serious complications if the catheter is, for example,<br />
in a permanent wedge position.<br />
2. Short extension tubings with low internal volume<br />
may be used safely, and standard inflating volumes<br />
produce a clinically acceptable inflation.<br />
Should one wish to obtain full inflation <strong>of</strong> the balloon,<br />
the specific tubings must be tested before use<br />
in a clinical situation.<br />
3. Long extension tubings should not be used as<br />
overinflation is unavoidable.<br />
We thank Dr. Martin Morissette for his editorial review and Mrs.<br />
Leila Geadah and Ginette Bleau for their secretarial assistance.<br />
References<br />
1. <strong>Swan</strong>-<strong>Ganz</strong> flow directed monitoring catheters, package insert.<br />
Edwards Laboratories. Ref. 108328 3 Rev. B.<br />
2. Barash PG, Nardi D, Hammond G. <strong>Catheter</strong> induced pulmonary<br />
artery perforation-mechanisms, management, and modifica-<br />
tion. J Thorac Cardiovasc Surg 1981;82:5-12.<br />
3. Eisenkraft JB, Eger I1 EI. Nitrous oxide and <strong>Swan</strong>-<strong>Ganz</strong> cathe-<br />
ters. Anesth Analg 1982;61:308-9.