S E C T I O N 1 4 The Skin in Immune, Autoimmune, <strong>and</strong> Rheumatic Disorders Systemic Amyloidosis ICD-9: 277.3 ° ICD-10: E85.3 ■ Amyloidosis is an extracellular deposition in various tissues of amyloid fibril proteins <strong>and</strong> of a protein called amyloid P component (AP); the identical component of AP is present in the serum <strong>and</strong> is called SAP. These amyloid deposits can affect normal body function. ■ Systemic AL amyloidosis, also known as primary amyloidosis, occurs in patients with B cell or plasma cell dyscrasias <strong>and</strong> multiple myeloma in whom fragments of monoclonal immunoglobulin light chains form amyloid fibrils. ■ Clinical features of AL include a combination of macroglossia <strong>and</strong> cardiac, renal, hepatic, <strong>and</strong> gastrointestinal (GI) involvement, as well as carpal tunnel syndrome <strong>and</strong> skin lesions. These occur in 30% of patients, <strong>and</strong> since they occur early 302 in the disease, they are an important clue to the diagnosis. ■ Systemic AA amyloidosis (reactive) occurs in patients after chronic inflammatory disease, in whom the fibril protein is derived from the circulating acute-phase lipoprotein known as serum amyloid A. ■ There are few or no characteristic skin lesions in AA amyloidosis, which usually affects the liver, spleen, kidneys, <strong>and</strong> adrenals. ■ In addition, skin manifestations may also be associated with a number of (rare) heredofamilial syndromes. ■ Localized cutaneous amyloidosis is not uncommon, presents with typical cutaneous manifestations, <strong>and</strong> has no systemic involvement. Systemic AL Amyloidosis ICD-9: 277.3 ° ICD-10: E85 ■ Rare, occurs in many, but not all, patients with multiple myeloma <strong>and</strong> B cell dyscrasia. ■ Skin Lesions: Smooth, waxy papules (Fig. 14-1), also nodules on the face, especially around the eyes (Fig. 14-2) <strong>and</strong> elsewhere. Purpura following trauma, “pinch” purpura in waxy papules (Fig. 14-2) sometimes also involving large surface areas without nodular involvement. Predilection sites are around the eyes, central face, extremities, body folds, axillae, umbilicus, anogenital area. Nail changes: similar to lichen planus (see Section 34). Macroglossia: diffusely enlarged <strong>and</strong> firm, “woody” (Fig. 14-3). ■ Systemic Manifestations: Fatigue, weakness, anorexia, weight loss, malaise, dyspnea; symptoms related to hepatic, renal, <strong>and</strong> GI involvement; paresthesia related to carpal tunnel syndrome, neuropathy. ■ ◐ ■ General Examination: Kidney—nephrosis; nervous system—peripheral neuropathy, carpal tunnel syndrome; cardiovascular—partial heart block, congestive heart failure; hepatic— hepatomegaly; GI—diarrhea, sometimes hemorrhagic, malabsorption; lymphadenopathy. ■ Laboratory: May reveal thrombocytosis >500,000/μL. Proteinuria <strong>and</strong> increased serum creatinine; hypercalcemia. Increased IgG. Monoclonal protein in two-thirds of patients with primary or myeloma-associated amyloidosis. Bone marrow: myeloma. ■ Dermatopathology: accumulation of faintly eosinophilic masses of amyloid in the papillary body near the epidermis, in the papillary <strong>and</strong> reticular dermis, in sweat gl<strong>and</strong>s, around <strong>and</strong> within blood vessel walls. Immunohistochemistry to assess the proportion of kappa <strong>and</strong> lambda light chains.
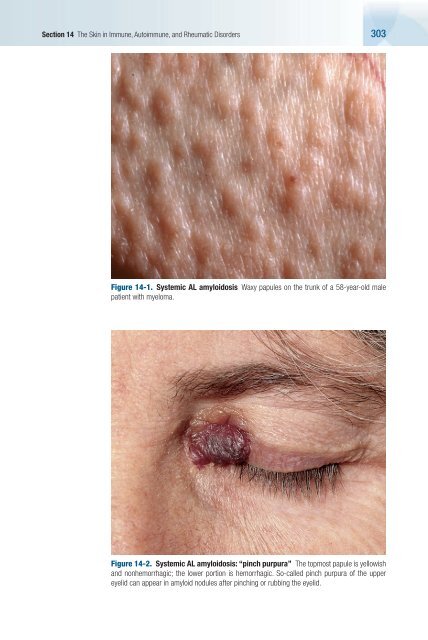
Section 14 The Skin in Immune, Autoimmune, <strong>and</strong> Rheumatic Disorders 303 Figure 14-1. Systemic AL amyloidosis Waxy papules on the trunk of a 58-year-old male patient with myeloma. Figure 14-2. Systemic AL amyloidosis: “pinch purpura” The topmost papule is yellowish <strong>and</strong> nonhemorrhagic; the lower portion is hemorrhagic. So-called pinch purpura of the upper eyelid can appear in amyloid nodules after pinching or rubbing the eyelid.