Strangulated inguinal hernia - nietoeditores.com.mx
Strangulated inguinal hernia - nietoeditores.com.mx
Strangulated inguinal hernia - nietoeditores.com.mx

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
* Departamento de Cirugía General, Hospital General Gaudencio<br />
González Garza, Centro Médico la Raza, Instituto Mexicano del<br />
Seguro Social, Mexico, D.F., Mexico<br />
Correspondence:<br />
Ernesto Manuel Góngora-Gómez<br />
Querétaro 144-412, Col. Roma, Deleg. Cuauhtémoc<br />
CP 06700, Mexico, D.F., Mexico<br />
Tel: (0155) 10844747 Ext. 7401<br />
E-mail: <strong>hernia</strong>gongora@gmail.<strong>com</strong><br />
Received for publication: 9-14-2011<br />
Accepted for publication: 3-28-2012<br />
abstract<br />
Cir Cir 2012;80:331-341<br />
<strong>Strangulated</strong> <strong>inguinal</strong> <strong>hernia</strong><br />
Ernesto Manuel Góngora-Gómez<br />
Background: <strong>Strangulated</strong> <strong>inguinal</strong> <strong>hernia</strong> (SIH) has an overall prevalence of 1.3% in adults, affecting mainly senile<br />
patients, with a high incidence of morbidity and mortality. There are more than 13 different surgical techniques for treatment,<br />
but none has proven to be more effective than the others.<br />
methods: The present observational, longitudinal and prospective study carried out at Hospital General, Centro Medico<br />
La Raza in Mexico City proposes a new surgical technique to treat SIH. Between December 2000 and August 2010,<br />
43 adult patients with SIH were consecutively subjected to preperitoneal mesh repair and exploratory laparotomy (PPMR<br />
and ELAP), a personal modification by the author to the Stoppa-Rives technique. Several variables were studied.<br />
results: There was zero mortality. There were no cases of <strong>inguinal</strong> recurrence or reintervention. One patient developed<br />
a granuloma at the surgical site. There were three cases of superficial wound infection, six cases of inguinoscrotal seroma,<br />
and one case of incisional <strong>hernia</strong>.<br />
discussion: There is no international consensus on the treatment of SIH although it is interesting to analyze the studies<br />
published during the last two decades and to observe the results. Studies that propose a preperitoneal approach with<br />
mesh demonstrate the best results by reducing morbidity and mortality.<br />
Conclusions: Preperitoneal mesh repair and exploratory laparotomy reduce the rate of morbidity and mortality in the<br />
treatment of SIH. Inguinal <strong>hernia</strong>s must be repaired at the time of diagnosis to avoid strangulation.<br />
Key words: strangulated <strong>inguinal</strong> <strong>hernia</strong>, preperitoneal mesh repair, exploratory laparotomy<br />
introduction<br />
The worldwide prevalence of strangulated <strong>inguinal</strong> <strong>hernia</strong><br />
(SIH) is 0.3–2.9% of all <strong>inguinal</strong> <strong>hernia</strong>s in adults. 1-3<br />
Primary <strong>hernia</strong>s strangulate more than recurrent and small<br />
<strong>hernia</strong>s more than large <strong>hernia</strong>s at a ratio of 5:1. 4 The risk<br />
of <strong>hernia</strong> strangulation is greatest during the first 3 months<br />
of its appearance 5 and occurs at an average age of 69 years<br />
with no difference between genders. The right side is most<br />
affected (2:1). Indirect <strong>hernia</strong>s be<strong>com</strong>e strangulated more<br />
than direct and femoral <strong>hernia</strong>s; the latter are more frequent<br />
in females. 6<br />
Before the use of mesh in <strong>inguinal</strong> <strong>hernia</strong> surgery there<br />
were no reports on morbidity of SIH because there was<br />
practically no short- or long-term follow-up on management<br />
of these cases. However, there were reports on mortality<br />
as follows: in 1959, Rogers 7 reported 26%, in 1960<br />
Nyhus et al. 8 reported 33%, in 1975 Read 9 reported 25%,<br />
in 1994 Pans and Jacquet 10 reported 17%, in 2000 Steinke<br />
and Zellweger 11 reported 25% and Harouna et al. 12 reported<br />
40%. After the advent of mesh, the mortality index has been<br />
reduced to 1–3%, whereas the reported incidence of recurrence<br />
is 0–4%, surgical wound infection 5–21%, and seroma<br />
3–15%. 13-15<br />
Some femoral, and mainly the obturator, <strong>hernia</strong>s be<strong>com</strong>e<br />
chronically sporadically trapped (especially in females).<br />
Isolated reports exist on the morbidity and mortality index<br />
of the latter when they cause acute episodes of occlusion<br />
and constitute a surgical emergency.<br />
From the time that plastic prostheses began to be used in<br />
the management of abdominal wall <strong>hernia</strong>, mainly <strong>inguinal</strong>,<br />
a revolution in surgical techniques began and thereby its<br />
terminology, coining new concepts such as “with tension”<br />
to refer to the traditional techniques by Bassinni, McVay,<br />
Halsted, and Shouldice and “tension free” to refer to the<br />
Volume 80, No. 4, July-August 2012 331
new techniques that used prosthetic mesh such as Lichtenstein,<br />
Stoppa, Mesh-Plug, PHS, etc. With the advent of the<br />
mesh, a revolution in the management of <strong>hernia</strong>s began,<br />
mainly in the groin. Prior to these changes there were at<br />
least nine procedures with “tension” suggested for management<br />
of SIH. After the onset of mesh prostheses, new<br />
“tension free” techniques have been incorporated, with application<br />
of the mesh anteriorly, preperitoneally, 21-23 or with<br />
laparoscopic techniques. 24-28 Currently, there are more than<br />
13 procedures re<strong>com</strong>mended for management of SIH.<br />
This study once again proposes the preperitoneal repair<br />
with mesh and exploratory laparotomy, confirming its advantages<br />
and favorable results because it resolves the <strong>hernia</strong><br />
as well as the damage caused by the ensuing strangulation<br />
by achieving the following:<br />
a) Access to both <strong>inguinal</strong> regions by the Cheatle-Henry<br />
technique<br />
b) Reduction of the sac and its contents<br />
c) Application of the prosthetic material and of a drainage<br />
system in the preperitoneal region<br />
d) Wide approach of the abdominal cavity that allows assessment<br />
of the damage, observation of the existence<br />
of unsuspected con<strong>com</strong>itant <strong>hernia</strong>s, identification of<br />
the number and degree of lesions in the internal organs,<br />
facilitation of intestinal de<strong>com</strong>pression, performance<br />
of the pertinent enterostomy and anastomosis or bowel<br />
rest if required and, finally, for washing and draining<br />
the cavity in case of intestinal leak and generalized<br />
peritonitis<br />
e) One sole repair technique for all types of <strong>inguinal</strong> <strong>hernia</strong>s<br />
by the application of mesh in the preperitoneal<br />
space, which allows for correction of all <strong>hernia</strong> defects<br />
in the inguinocrural region, eliminating the need to apply<br />
a different technique for each <strong>hernia</strong> type<br />
f) No specialized training necessary because all surgeons<br />
can perform the procedure and the use of sophisticated<br />
equipment is not required (such as the laparoscope) or<br />
a long learning curve<br />
g) The only option for advanced cases (gangrene of the<br />
soft tissues or great intestinal dilation) that require<br />
debridement, orchiectomy, bowel de<strong>com</strong>pression, and<br />
relaxing incisions to enlarge the orifice and free the<br />
trapped organ<br />
Early diagnosis, overall evaluation of the patient’s status<br />
and timely treatment are the keys for prognosis as well as<br />
intensive fluid replacement, adequate antibiotic use, nasogastric<br />
de<strong>com</strong>pression of the abdomen, kidney monitoring<br />
and correction of coagulation parameters and other existing<br />
health issues due to the multipathological nature of these<br />
patients. These objectives must be met promptly, during the<br />
first 2–4 h prior to the surgical event.<br />
Góngora-Gómez EM<br />
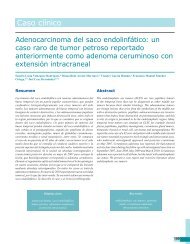
Details of the surgical technique: preperitoneal mesh repair<br />
and exploratory laparotomy (Figure 1)<br />
A midline infraumbilical incision was made close to the<br />
symphysis pubis and after dissection by planes the preperitoneal<br />
space was entered without opening the peritoneum.<br />
Ipsilateral traction was carried out over the muscular wall to<br />
expose by blunt dissection the posterior wall of the affected<br />
groin (the surgeon has the option to primarily explore the<br />
contralateral groin in search of suspected or unidentified<br />
con<strong>com</strong>itant <strong>hernia</strong>s) 29 and the site of <strong>hernia</strong> strangulation<br />
was located to manually reduce it with traction and internal<br />
and external gentle countertraction. If such a reduction is<br />
not possible, relaxing incisions should be made to widen the<br />
neck of the <strong>hernia</strong>. In case of indirect <strong>hernia</strong>, the epigastric<br />
vessels should be cut and ligated, protecting the sac and its<br />
contents so as to not open it. A cut is made in the internal<br />
ring between 11 and 12 o’clock in an oblique superomedial<br />
direction, resecting the fibers of the ligament of Hesselbach<br />
and the conjoined tendon (Figure 2). In the direct <strong>hernia</strong><br />
the cut is made between 10 and 11 o’clock and over the<br />
posterior fascia of the union of the rectus and transverse<br />
muscles (posterior face of the conjoined tendon or ligament<br />
of Henle) (Figure 3).<br />
If the <strong>hernia</strong> is femoral, the cut will be oblique in the<br />
iliopubic tract at its insertion at the ligament of Cooper<br />
(Gimbernat ligament) medially. It should be noted that the<br />
femoral vessels are found adjacent in the external lateral<br />
sense and in the lateral superior direction the epigastrics<br />
emerge. Exposure and cutting maneuvers should be done<br />
gently and precisely (Figure 4).<br />
If an obturator <strong>hernia</strong> is found, the cut should be made in<br />
the endopelvic fascia below the ligament of Cooper medially<br />
and inferior to avoid the obturator vessels and nerves<br />
(Figure 5).<br />
Once the sac and its contents are freed, it is retracted<br />
towards the abdomen without opening it, in order to avoid<br />
contamination. If reduction of the sac is impossible (because<br />
it is intimately adhered) it can be ligated and cut at<br />
the level of the neck avoiding as much as possible escape of<br />
the contents to the preperitoneal space, leaving the inguinoscrotal<br />
remnant of the sac attached. This will be exhaustively<br />
washed and will allow exteriorization of one of the<br />
drainage tubes closed to suction (in case a perforated sac<br />
is found, with evident contamination due to the presence<br />
of an abscess and/or intestinal leak, a mesh should not be<br />
applied and Nyhus type fascial repair will be done). A piece<br />
of polypropylene mesh not less than 10 × 12 cm should be<br />
placed before parietalization of the spermatic cord, suturing<br />
it with nonabsorbable monofilament material to the pubic<br />
tubercle, Cooper’s ligament, iliopsoas fascia and conjoined<br />
332 Cirugía y Cirujanos
<strong>Strangulated</strong> <strong>inguinal</strong> <strong>hernia</strong><br />
Midline incision<br />
Perforated sac<br />
Abscess and intestinal leak<br />
in <strong>inguinal</strong> region. Do not<br />
apply<br />
Fascial type Nyhus repair<br />
Contralateral<br />
preperitoneal exploration<br />
Preperitoneal exploration<br />
Groin pathology<br />
Reduction of sac<br />
Not opened<br />
Integral sac<br />
Apply polypropylene mesh<br />
parietalization of the cord<br />
Installation of closed<br />
drainage<br />
Approach abdominal cavity<br />
according to midline,not<br />
Exploration and evaluation<br />
of damage<br />
Resection and intestinal<br />
anastomosis, closed technique<br />
Solution for other damages<br />
¿lavage?/cavity drainage?<br />
Closure of wall with<br />
aseptic technique<br />
Presence of <strong>hernia</strong><br />
Absence of <strong>hernia</strong><br />
figure 1. Algorithm of surgical technique: preperitoneal repair with mesh and exploratory laparotomy.<br />
Unilateral<br />
prosthesis<br />
Adherence of sac<br />
section at the level of the<br />
neck; avoid leaks<br />
Leave residual sac in situ<br />
Volume 80, No. 4, July-August 2012 333
figure 2. Incision in ligament of Hesselbach.<br />
tendon. A closed drain is then installed, which is exteriorized<br />
from below and inside the anterior superior iliac spine<br />
(the surgeon decides on the exit site according to the type<br />
of case). This type of drainage has decreased the number<br />
of hematomas reported in other studies. We now proceed<br />
(but not earlier) to opening the peritoneum via the midline<br />
to <strong>com</strong>plete the approach by means of a laparotomy. Using<br />
this route, the cavity is explored to evaluate the damage and<br />
its repair. Resection of the affected organs is performed and<br />
anastomosis, if the damage is intestinal. This exposure will<br />
allow washing of the cavity and draining, if necessary. In<br />
some cases de<strong>com</strong>pression of the dilated intestine is obligatory<br />
because if not done it imposes closure under tension of<br />
the cavity. The surgeon will manually de<strong>com</strong>press in retrograde<br />
manner or aspiration through enterotomy. The wall<br />
closure should be <strong>com</strong>pleted using aseptic technique. Also,<br />
the skin edges and epidermis will be left open in case of<br />
peritonitis and according to the surgeon’s judgment.<br />
Emphasis is given to proceed with careful handling of<br />
tissues, judicious use of cautery and suture materials, shorter<br />
operative times, removal of devitalized tissue, use of efficient<br />
drainage and aseptic closure of the cavity. General<br />
figure 3. Incision in ligament of Henle.<br />
Góngora-Gómez EM<br />
anesthesia is ideal for this surgery because it provides adequate<br />
intraoperative relaxation.<br />
Patients and methods<br />
From December 1, 2000 to August 31, 2010, 43 adult patients<br />
with SIH underwent emergency surgery consecutively<br />
with preperitoneal repair with mesh and exploratory<br />
laparotomy. Patients were all seen in the Emergency Department<br />
of the General Hospital Medical Center La Raza<br />
in Mexico City. All patients underwent routine screening<br />
studies: blood count, blood chemistry, serum electrolytes,<br />
blood amylase, prothrombin time, partial thromboplastin<br />
time, abdominal x-rays standing and supine and chest xray.<br />
All patients were assessed primarily by an emergency<br />
physician who initiated rehydration therapy, analgesia and<br />
antibiotics. The Department of General Surgery was then<br />
contacted for interconsultation.<br />
334 Cirugía y Cirujanos
<strong>Strangulated</strong> <strong>inguinal</strong> <strong>hernia</strong><br />
figure 4. Incision in ligament of Gimbernat.<br />
results<br />
Average age of the patients was 71 years (range: 26–92<br />
years). There were 18 females and 25 males. There were 33<br />
patients with <strong>com</strong>orbidities with the following being predominant:<br />
hypertension (19 patients), obesity (16 patients),<br />
type 2 diabetes mellitus (8 patients), prostatism (6 patients),<br />
lung disease (6 patients), heart disease (5 patients), and renal<br />
disease (3 patients). There were 33 cases of primary <strong>hernia</strong><br />
and 10 cases of recurrent <strong>hernia</strong> (three with more than<br />
two recurrences). Small <strong>hernia</strong>s (8 cm (9 cases). The right side<br />
was most affected (24 cases) than the left (19 cases). The<br />
time of evolution since the first symptoms appeared until<br />
the time of surgery was 46.2 h (9–90 h); 39 patients had<br />
signs of intestinal obstruction and 24 patients had signs of<br />
peritoneal irritation. There were 19 cases of dehydration.<br />
Leukocytosis >10,000 was demonstrated in 28 patients and<br />
bandemia in 12 patients. Dermoepidermal changes were<br />
present in five cases (one with scrotal gangrene). X-rays of<br />
the abdomen showed air fluid levels in 36 patients, bowel<br />
loop dilation in 39 patients, free fluid in the cavity in eight<br />
patients, and intestinal wall edema in 28 cases. All patients<br />
were subjected to preperitoneal surgical repair with mesh<br />
figure 5. Incision in the endopelvic fascia below Cooper’s ligament.<br />
and exploratory laparotomy. We chose the Gilbert-Rutkow<br />
classification (because it was the most practical and <strong>com</strong>plete<br />
in our estimation) to group the <strong>hernia</strong>s of our patients:<br />
type II (8 cases); type III (14 cases); type IV (6 cases), type<br />
V (1 case), type VI (5 cases) and type VII [9 cases (female<br />
predominance with 7 cases and 2 cases of males)]. There<br />
were also con<strong>com</strong>itant <strong>hernia</strong>s found: six contralateral, one<br />
ipsilateral, two umbilical and two postincisional. There<br />
were four Richter <strong>hernia</strong>s identified and one Amyand. 30<br />
Resection was carried out on 34 patients due to necrosis,<br />
although in some cases there was <strong>com</strong>promise of more than<br />
one organ: small intestine in 18 cases (all with involvement<br />
of some segment of the ileum and that was resolved with<br />
end-to-end anastomosis in two planes), <strong>hernia</strong> lipoma in 13<br />
cases, <strong>hernia</strong> sac in 19 cases, omentum in eight cases, epiploic<br />
appendix in four cases, testicle in three cases, colon in<br />
two cases (the cecum in one case that required an ileostomy<br />
and sigmoid in the second case that required colostomy of<br />
Volume 80, No. 4, July-August 2012 335
the descending colon); the cecal appendix of the Amyand<br />
case was excised despite vascular recuperation. There were<br />
nine cases without resection because the trapped organs recovered<br />
their viability. There was also more than one organ<br />
found trapped: small intestine 6, colon 5 (two of the cecum<br />
and three of sigmoid), and omentum 5 (Table 1).<br />
Peritonitis due to intestinal leakage occurred in four cases,<br />
all of which were managed with scrupulous washing of the<br />
cavity, application of Saratoga-type drains in both parietocolic<br />
gutters and management with double or triple antibiotic.<br />
One case of intestinal leak was due to cecal perforation<br />
(the case that required ileostomy) and the other three were<br />
leaks from the small intestine. After segmental bowel resection,<br />
anastomosis with aseptic technique was performed<br />
in two planes. A preperitoneal <strong>inguinal</strong> drain was placed<br />
in 24 patients and intraabdominal in ten patients (four of<br />
these patients experienced intestinal leak). A relaxing incision<br />
was done in the constricting <strong>hernia</strong> ring because it was<br />
impossible to free up the <strong>hernia</strong> sac and its contents with<br />
simple maneuvers in 18 cases: ten indirect <strong>hernia</strong>s, four indirect<br />
<strong>hernia</strong>s and four femoral <strong>hernia</strong>s. The characteristics<br />
of the mesh installed were Dacron 2, polypropylene (PPL)<br />
37, light mesh 3, and <strong>com</strong>posite (polypropylene + Teflon)<br />
1. General anesthesia was administered in all cases because<br />
of the requirement of adequate intraabdominal relaxation.<br />
Average surgical time was 142 min (75–260 min) (Table 2).<br />
Antibiotic therapy was administered with one or more<br />
drugs: two cases without antibiotics, monotherapy in 21<br />
cases, two antibiotics in 15 cases, and three antibiotics in<br />
five cases. Average hospital stay was 7.1 days (2–25 days).<br />
Follow-up of 1–118 months was reported in 21 patients;<br />
13 patients died during the course of the study due to non-<br />
table 1. Resection due to necrosis or vascular repair<br />
Resection for necrosis* 34 Small intestine 18<br />
Hernia sac 19<br />
Hernia lipoma 13<br />
Omentum 8<br />
Epiploic appendix 4<br />
Testicle 3<br />
Colon 2<br />
Without resection for 9 Small intestine 6<br />
vascular recuperation ** Colon 5<br />
Omentum 5<br />
Cecal appendix 1<br />
* Various cases with more than one necrosed organ.<br />
** Various cases with more than one incarcerated organ.<br />
Góngora-Gómez EM<br />
table 2. Surgical findings for SIH<br />
Peritonitis* 4<br />
Drainage Inguinal** 24<br />
Abdominal 10<br />
Relaxing incision Indirect opening 10<br />
(18)<br />
Direct opening 4<br />
Femoral opening 4<br />
Type of mesh Polypropylene 37<br />
Light 3<br />
Dacron 2<br />
Bilayer 1<br />
Type of anesthesia General 43<br />
Surgical Time (min) 142’<br />
*Intestinal leak due to perforation.<br />
**Closed drainage. SIH, strangulated <strong>inguinal</strong> <strong>hernia</strong>.<br />
surgical-related causes. Nine patients were lost to followup.<br />
No deaths occurred during surgical management or during<br />
the postoperative period. Deaths occurred during a 10year<br />
period due to various diseases unrelated to the surgery.<br />
There were zero recurrences during the follow-up period.<br />
There were no re-operations. No case had to be reoperated<br />
during the immediate postoperative period. There was<br />
an infected granuloma in one patient; 2 months after surgery<br />
an area of swelling was demonstrated in the interior<br />
<strong>com</strong>missure of the scar that finally revealed three knots of<br />
suture material and remained oozing until we opened to 3<br />
cm and washed the area intensively for 12 days until control<br />
was obtained. Closure was done by secondary intent<br />
without requiring re-exploration or removal of the mesh.<br />
Incisional <strong>hernia</strong> was done in one patient detected 1 month<br />
after surgery in the mid-third portion of the scar. The patient<br />
underwent conventional open herniorraphy during the<br />
second month without incident. Infection occurred in three<br />
patients. The wound was left open due to development of<br />
peritonitis and the infection was controlled with exhaustive<br />
lavage, without mesh infection. In two patients we reapproximated<br />
the wound margins with sutures, and in the<br />
third patient closure was done by secondary intent. There<br />
were six cases of seroma, four were noted among the first<br />
10 cases reported. We did not leave a preperitoneal drain as<br />
routinely done and the other two occurred with cases of giant<br />
inguinoscrotal <strong>hernia</strong>s. All resolved with one and three<br />
evacuation punctures performed aseptically during office<br />
consultation (Figure 6).<br />
336 Cirugía y Cirujanos
<strong>Strangulated</strong> <strong>inguinal</strong> <strong>hernia</strong><br />
7<br />
6<br />
5<br />
4<br />
3<br />
2<br />
1<br />
0<br />
Results<br />
Seroma Surgical Incisional<br />
wound<br />
infection<br />
<strong>hernia</strong><br />
figure 6. Results of morbidity with the surgical technique for<br />
strangulated <strong>inguinal</strong> <strong>hernia</strong>.<br />
discussion<br />
Granuloma<br />
Management of the <strong>com</strong>plicated <strong>inguinal</strong> <strong>hernia</strong> requires<br />
a precise diagnosis. It is important to define the degree of<br />
involvement of its contents. In the case of SIH, all intervening<br />
aggravating factors should be analyzed. Selection<br />
of the operative technique is still controversial; however,<br />
each day there is further proof of the benefits derived from<br />
wide abdominal cavity exploration and <strong>hernia</strong> repair with<br />
preperitoneal prosthesis during the same surgical event. Another<br />
reason for the controversy is the use of mesh in areas<br />
potentially contaminated; however, various reports confirm<br />
that its use in such situations is not contraindicated. 31-34<br />
Approaching a strangulated <strong>inguinal</strong> <strong>hernia</strong> via an <strong>inguinal</strong><br />
incision without exploration of the abdominal cavity<br />
carries distinct risks:<br />
• Missing inadvertent unsuspected con<strong>com</strong>itant <strong>hernia</strong>s<br />
• Totally missing intraabdominal lesions that cannot<br />
be identified through a limited <strong>hernia</strong> orifice such as<br />
perforation and intestinal leak, severe ischemia and/or<br />
necrosis of the small or large intestine, of the omentum,<br />
epiploic appendix or cecal appendix, bladder or<br />
the testicle<br />
• Not identifying chronic constrictions in the intestine<br />
when strangulated, provoked by the tight neck of the<br />
<strong>hernia</strong> that in the future will stenose and cause difficult<br />
to diagnose intestinal occlusions 35<br />
• Ignoring the presence of unsuspected purulent or intestinal<br />
blood collections that warrant drainage<br />
• High degree of difficulty for intestinal resection and<br />
anastomosis as well as placing the surgical procedure<br />
at risk when performing a contaminated procedure in<br />
the <strong>inguinal</strong> region<br />
Postponing the surgery for a second surgical time gives<br />
priority to the resection, maintaining the latent risk of a second<br />
strangulation in the short term.<br />
In the past decade, various types of light mesh prostheses<br />
associated with polyglactine or polyglecaprone to reduce<br />
regional inflammatory reaction of index of seroma began to<br />
be used. We used three types of these mesh prostheses and<br />
no cases of seroma were presented. However, it should be<br />
mentioned that this <strong>com</strong>plication may be due to a number of<br />
associated factors such as the size of the <strong>hernia</strong> and, therefore,<br />
the extension of the regional surgical dissection, size<br />
and characteristics of the prosthesis (heavy or light), resection<br />
or not of the <strong>hernia</strong> sac, use of a delayed surgery and<br />
installation of a good closed drainage. In other reports on<br />
seromas, minor <strong>com</strong>plications have been reported after use<br />
of heavy Dacron or polypropylene mesh, but these reports<br />
did not mention if drains were used. In our series the largest<br />
number of seromas occurred when a closed drain was not<br />
installed. We also point out that the closed drain decreases<br />
the possibility of exterior contamination as may occur with<br />
open drains.<br />
Since 1994, various studies reporting the use of mesh for<br />
management of SIH have been published with good short-<br />
and long-term results; however, some of these studies do not<br />
distinguish, with certainty, incarcerated from SIH and both<br />
concepts were managed in an indistinct manner. Some are<br />
reports of individual cases and other report on larger series.<br />
Up to now there have been no <strong>com</strong>parative and randomized<br />
studies that individually confront the different techniques.<br />
The studies that report the use of open techniques with<br />
mesh and those that use laparoscopic techniques report a<br />
substantial decrease in morbidity and mortality.<br />
In 1994, Henry and Randriamanantsoa 22 proposed the<br />
use of prostheses in surgical emergencies. They applied<br />
15 mesh plugs, 32 Mersiline meshes and 7 Vicryl meshes,<br />
mainly through an <strong>inguinal</strong> approach. Resection was carried<br />
out in five cases, reporting only one wall abscess as a<br />
<strong>com</strong>plication.<br />
In 1996, Gavioli et al. 32 presented their work with 31<br />
cases subjected to the application of a polypropylene mesh<br />
(29 cases) and Dacron (2 cases) preperitoneally or retromuscularly.<br />
They performed intestinal resection in three<br />
patients and omentum in 13 due to necrosis. There were no<br />
infections or recurrences. These authors proposed the use of<br />
mesh in SIH, excluding the case with severe infection due<br />
to gangrenous intestine, perforation and peritonitis as well<br />
as in those in whom colonic resection is performed.<br />
In 1997 Pans et al. 21 published a retrospective study suggesting<br />
the use of a preperitoneal prosthesis using a midline<br />
abdominal approach. They presented a series of 35 cases in<br />
which 13 resections were performed, although the degree of<br />
vascular involvement in the unresected cases was not speci-<br />
Volume 80, No. 4, July-August 2012 337
fied. Complications included two infections of the surgical<br />
wound that did not require mesh removal, six hematomas,<br />
one seroma, one recurrence 46 months later and a death unrelated<br />
to the surgery. No drains were left. Follow-up was<br />
4.2 years.<br />
In 2000, Mauch et al. 23 studied 44 patients: 32 with incarcerated<br />
<strong>inguinal</strong> <strong>hernia</strong> and 12 with SIH. These authors<br />
proposed a midline posterior approach and repair with mesh<br />
in all cases. Resection was done in 12 cases and the results<br />
included eight cases of wound infection, two recurrences<br />
and no deaths.<br />
The first reports of transabdominal preperitoneal laparoscopic<br />
management management (TAPP) <strong>com</strong>bined with<br />
assisted intestinal resection were published by Tschudi et<br />
al. 16 and Watson et al. 24 in 1993 (report of isolated cases).<br />
Since then, other reports have been published such as the<br />
one from Leibl et al. 28 in 2001 that consisted of a retrospective<br />
study of 194 cases of incarcerated <strong>inguinal</strong> <strong>hernia</strong>s.<br />
These authors introduced the terms “chronic incarcerated”<br />
and “acute incarcerated,” and performed resection in only<br />
six cases, reporting a morbidity of 6.6% without deaths or<br />
recurrences during a 26-month follow-up.<br />
In 2004, Ferzli et al. 27 proposed the total extraperitoneal<br />
(TEP) laparoscopic approach in a retrospective study of 16<br />
patients, of whom five were managed via a conventional<br />
anterior approach (type of technique was unspecified) because<br />
of intestinal gangrene and inflammation of the <strong>inguinal</strong><br />
wall. Eleven patients began with TEP and three patients<br />
were converted to an open procedure, but the technique<br />
was not specified. A morbidity of 25% was reported and<br />
included a mesh infection resolved with local hygiene and a<br />
wound infection. These authors introduced the term “acutely<br />
incarcerated.”<br />
In 2005, Gongora 4 reported on a <strong>com</strong>parative study presenting<br />
38 cases of SIH divided into two groups: group A<br />
with 20 cases operated with different open techniques and<br />
group B with 18 cases operated with preperitoneal repair<br />
with mesh and exploratory laparotomy. Eighteen cases in<br />
group A required resection of some intraabdominal organ<br />
and 16 cases in group B. Results on morbidity and mortality<br />
show important differences between groups. In group A<br />
there were three deaths, five recurrences, five wound infections,<br />
two granulomas, and four re-operations. In group B<br />
there were no cases of recurrences, death or re-operation.<br />
There were two wound infections, one granuloma, one seroma<br />
and one case of incisional <strong>hernia</strong>. It is notable that<br />
the index of recurrence has statistical significance (p
<strong>Strangulated</strong> <strong>inguinal</strong> <strong>hernia</strong><br />
anesthetic contraindications or due to the large size of the<br />
<strong>hernia</strong>s.) Two cases required resection and one case had<br />
postincisional herniorrhaphy performed without recurrence<br />
after an 18-month follow-up. They concluded that TAPP<br />
can be proposed for management of SIH allowing the correction<br />
of the <strong>hernia</strong> and the resolution of the damage as<br />
well as visual control of the type of vascular injury of the<br />
trapped organ and its possible recovery.<br />
In 2009, Deeba et al. 38 presented a review paper on seven<br />
references captured from Medline, Ovid, Cochrane, Embase<br />
and Google on the laparoscopic management of SIH. They<br />
analyzed 328 cases reporting six conversions, 17 bowel resections<br />
resolved laparoscopically or by minilaparotomy<br />
and 34 <strong>com</strong>plications (25 classified as minor). No mention<br />
was made of recurrence or mortality. Table 3 provides a review<br />
of all the authors mentioned above, emphasizing that<br />
there is statistical significance with p 12 h of evolution<br />
• intestinal occlusive syndrome with gastrointestinal<br />
vomiting, bloating and diffuse colic<br />
• systemic inflammatory response syndrome (tachycardia,<br />
dehydration, leukocytosis, etc.)<br />
• signs of peritoneal irritation<br />
• radiological changes with bowel loop distention, air<br />
fluid levels, free fluid and/or intra-abdominal collections,<br />
etc.<br />
Given these signs and symptoms, we may ascertain that<br />
it is possible to establish the definitive diagnosis of SIH<br />
Years of<br />
follow-up<br />
1994 Henry22 Inguinal approach 54 5 9 -<br />
1996 Gavioli32 Preperitoneal mesh 31 16 51 -<br />
1997 Pans21 Preperitoneal mesh 35 13 37 4.2<br />
2000 Mauch23 Preperitoneal mesh 44 12 27 2<br />
2001 Leibl28 Tapp** 194 6 3 2<br />
2005<br />
Papaziogas34 Lichtenstein 33 4 12 9<br />
Bassini 42 10 23 9<br />
2006 Rebuffat6 Tapp 28 9 32 1<br />
2006 Wisocky14 Lichtenstein 56 8 14 3<br />
Bassini 21 5 23 3<br />
2007 Bessa15 Lichtenstein 25 4 16 1<br />
2008 Dieng36 Bassini-McVay 228 16 7 3.5<br />
2008 Legnani37 Tapp 9 2 22 1.5<br />
2009 Deeba38 * Tapp-Tep*** 328 17 5 -<br />
2010 Góngora20 RPPM and LAPE**** 43 34 79 10<br />
*Review articles from 1989–2008: COCHRANE, OVID, MEDLINE, EMBASE, GOOGLE (seven articles chosen<br />
among 43).<br />
**Intraabdominal preperitoneal technique.<br />
***Total extraperitoneal technique.<br />
****Preperitoneal repair with mesh and exploratory laparotomy.<br />
Volume 80, No. 4, July-August 2012 339
from the preoperative period. Therefore, that this set of syndromes<br />
should be considered as inclusion criteria to qualify<br />
specific cases of SIH and to clearly differentiate incarcerated<br />
<strong>inguinal</strong> <strong>hernia</strong>s or reduced <strong>hernia</strong>s. The latter do not<br />
suffer vascular damage and, therefore, constitute a bias by<br />
their imprecise inclusion in the case series. After emphasis<br />
on vascular damage and its impact from SIH, treatment<br />
should be considered mandatory, whereas an elective procedure<br />
may be used for reduced or incarcerated <strong>hernia</strong>s.<br />
In conclusion:<br />
• The operative technique of preperitoneal mesh repair<br />
and exploratory laparotomy has reduced morbidity and<br />
mortality in the management of SIH.<br />
• Proceeding with preperitoneal mesh repair and exploratory<br />
laparotomy would allow for resolution of all cases<br />
of SIH, regardless of the <strong>com</strong>plications that arise and<br />
type of existing <strong>hernia</strong>, including more advanced cases.<br />
• Preperitoneal mesh repair and exploratory laparotomy<br />
is accessible to any surgeon because it requires no additional<br />
technology than what is available in any operating<br />
room.<br />
• The use of mesh in <strong>hernia</strong>s and/or in potentially contaminated<br />
areas should not be considered a contraindication.<br />
• All <strong>inguinal</strong> <strong>hernia</strong>s must undergo a tension-free plasty<br />
in the shortest time possible, especially in the case of<br />
patients >60 years of age.<br />
references<br />
1. Álvarez JA, Baldonedo RF, Bear IG, Solís JAS, Álvarez P, Jorge JI.<br />
Incarcerated groin <strong>hernia</strong>s in adults: presentation and out<strong>com</strong>e. Hernia<br />
2004;8:121-126.<br />
2. Kurt N, Oncel M, Ozkan Z, Bingul S. Risk and out<strong>com</strong>e of bowel<br />
resection in patients with incarcerated groin <strong>hernia</strong>s: retrospective<br />
study. World J Surg 2003;27:741-743.<br />
3. Primatesta P. Goldacre MJ. Inguinal <strong>hernia</strong> repair: incidence of elective<br />
and emergency surgery, readmission and mortality. Int J Epidemiol<br />
1996;25:835-889.<br />
4. Góngora-Gómez EM. Reparación preperitoneal con malla y laparotomía<br />
en la <strong>hernia</strong> <strong>inguinal</strong> estrangulada. Cir Gen 2005;27:31-36.<br />
5. Gallegos NC, Dawson J, Jarvis M, Hobsley M. Risk of strangulation<br />
in groin <strong>hernia</strong>s. Br J Surg 1991;78:1171-1173.<br />
6. Rebuffat C, Galli A, Scalambra MS, Balsamo F. Laparoscopic repair<br />
of strangulated <strong>hernia</strong>s. Surg Endosc 2006;20:131-134.<br />
7. Rogers FA. <strong>Strangulated</strong> femoral <strong>hernia</strong>. A review of 170 cases. Ann<br />
Surg 1959;149:9-20.<br />
8. Nyhus LM, Condon RE, Harkins HN. Clinical experience with preperitoneal<br />
<strong>hernia</strong> repair for all types of <strong>hernia</strong> of the groin: with particular<br />
reference to the importance of transversalis fascia analogues.<br />
Am Surg 1960;100:234-244.<br />
9. Read RC. Recurrence after preperitoneal herniorrhaphy in the adult.<br />
Arch Surg 1975;110:666-671.<br />
Góngora-Gómez EM<br />
10. Pans A, Jacquet N. Prostheses in emergency surgery. II. In: Bendavid<br />
R, ed. Prostheses and Abdominal Wall Hernias. Austin, TX: RG Landes;<br />
1994. pp. 342-353.<br />
11. Steinke W, Zellweger R. Richter’s <strong>hernia</strong> and Sir Frederick Treves:<br />
an original clinical experience, review and historical overview. Ann<br />
Surg 2000;232:710-718.<br />
12. Harouna Y, Yaya H, Abdou I, Bazira L. Prognosis of strangulated<br />
<strong>inguinal</strong> <strong>hernia</strong> in the adult: influence of intestinal necrosis. A propos<br />
of 34 cases. Bull Soc Pathol Exot 2000;93:317-320.<br />
13. Kelly ME, Behrman SW. The safety and efficacy of prosthetic <strong>hernia</strong><br />
repair in clean-contaminated and contaminated wounds. Am Surg<br />
2002;68:524-529.<br />
14. Wysocki A, Kulawik J, Pozniczek M, Strzalka M. Is the Lichtenstein<br />
operation of strangulated groin <strong>hernia</strong> a safe procedure? World J Surg<br />
2006;30:2065-2070.<br />
15. Bessa SS, Katri KM, Abdel-Salam WN, Abdel Baki NA. Early results<br />
from the use of the Lichtenstein repair in the management of<br />
strangulated groin <strong>hernia</strong>. Hernia 2007;11:239-242<br />
16. Tschudi J, Wagner M, Klaiber C. Laparoscopic operation of incarcerated<br />
obturator <strong>hernia</strong> with assisted intestinal resection. Chirurg<br />
1993;64:827-828.<br />
17. Shapiro K, Patel S, Choy C, Chaudry G, Khalil S, Ferzli G. Totally extraperitoneal<br />
repair of obturator <strong>hernia</strong>. Surg Endosc 2004;18:954-956.<br />
18. Uludag M, Yetkin G, Kebudi A, Isgor A, Akgun I, Donmez AG. A<br />
rare cause of intestinal obstruction: incarcerated femoral <strong>hernia</strong>,<br />
strangulated obturator <strong>hernia</strong>. Hernia 2006;10:288-291.<br />
19. Cueto-García J, Rodríguez-Díaz M, Elizalde-Di MA, Weber-Sanchez<br />
A. Incarcerated obturator <strong>hernia</strong> successfully treated by laparoscopy.<br />
Surg Laparosc Endosc 1998;8:71-73.<br />
20. Góngora GE. Hernia <strong>inguinal</strong> estrangulada. In: Mayagoitia GJ. Hernias<br />
de la Pared Abdominal, Tratamiento Actual. 2nd ed. México,<br />
DF: Editorial Alfil; 2009. pp. 223-233.<br />
21. Pans A, Desaive C, Jacquet N. Use of a preperitoneal prostheses for<br />
strangulated groin <strong>hernia</strong>s. Br J Surg 1997;84:310-312.<br />
22. Henry X, Randriamanantsoa V. Prostheses in emergency surgery. I.<br />
In: Bendavid R, ed. Prostheses and Abdominal Wall Hernias. Austin,<br />
TX: RG Landes; 1994. pp. 337-341.<br />
23. Mauch J, Helbling C, Schlumpf R. Incarcerated and strangulated <strong>hernia</strong>s--surgical<br />
approach and management. Swiss Surg 2000;6:28-31.<br />
24. Watson SD, Saye W, Hollier PA. Combined laparoscopic incarcerated<br />
herniorrhaphy and small bowel resection. Surg Laparosc Endosc<br />
1993;3:106-108.<br />
25. Franklyn ME, Rosenthal D, Díaz EJ, Balli JE. Laparoscopic intraperitoneal<br />
<strong>hernia</strong> repair. Cir Gen 1998;20(suppl 1):29-35.<br />
26. Weber SA, Vázquez FJA, Cueto GJ. La <strong>hernia</strong> <strong>inguinal</strong> en la era laparoscópica.<br />
Reparación tipo TAPP (abordaje transabdminal preperitoneal).<br />
Cir Gen 1998;20(suppl 1):21-28.<br />
27. Ferzli G, Shapiro K, Chaudry G, Patel S. Laparoscopic extraperitoneal<br />
approach to acutely incarcerated <strong>inguinal</strong> <strong>hernia</strong>. Surg Endosc<br />
2004;18:228-231.<br />
28. Leibl BJ, Schmedt GC, Kraft K, Kraft B, Bittner R. Laparoscopic<br />
transperitoneal <strong>hernia</strong> repair of incarcerated <strong>hernia</strong>s. Is it feasible?<br />
Results of prospective study. Surg Endosc 2001;15:1179-1183.<br />
29. Koehler RH. Diagnosing the occult contralateral <strong>inguinal</strong> <strong>hernia</strong>.<br />
Surg Endosc 2002;16:512-520.<br />
30. Sharma H, Gupta A, Shekhawat NS, Memon B, Memon MA. Amyand’s<br />
<strong>hernia</strong>: a report of 18 consecutive patients over a 15-year period.<br />
Hernia 2007;11:31-35.<br />
31. Wysocki A, Pozniczek M, Krzywon J, Bolt L. Use of polypropylene<br />
prostheses for strangulated <strong>inguinal</strong> and incisional <strong>hernia</strong>s. Hernia<br />
2001;5:105-106.<br />
340 Cirugía y Cirujanos
<strong>Strangulated</strong> <strong>inguinal</strong> <strong>hernia</strong><br />
32. Gavioli M, Rosi A, Piccagli I, Zenezini Chiozzi A, Bernardelli D,<br />
Lazzaretti MG, et al. Prosthesis and emergency surgery of <strong>hernia</strong>. J<br />
Chir 1996;133:317-319.<br />
33. Campanelli G, Nicolosi FM, Pettinari D, Avesani EC. Prosthetic<br />
repair, intestinal resection, and potentially contaminated areas: safe<br />
and feasible? Hernia 2004;8:190-192.<br />
34. Papaziogas B, Lazaridis CH, Makris J, Koutelidakis J, Patsas A,<br />
Grigoriou M, et al. Tension-free repair versus modified Bassini technique<br />
(Andrews technique) for strangulated <strong>inguinal</strong> <strong>hernia</strong>: a <strong>com</strong>parative<br />
study. Hernia 2005;9:156-159.<br />
35. Dakubo JCB, Akoto H, Etwire VK, Naaeder SB. Ileal stricture following<br />
strangulated <strong>inguinal</strong> <strong>hernia</strong>. Trop Doct 2007;37:260-262.<br />
36. Dieng M, El Kouzi B, Ka O, Konaté I, Cissé M, Sanou A, et al.<br />
<strong>Strangulated</strong> groin <strong>hernia</strong>s in adults: a survey of 228 cases. Mali Med<br />
2008;23:12-16.<br />
37. Legnani GL, Rasini M, Pastori S, Sarli D. Laparoscopic trans-peritoneal<br />
hernioplasty (TAPP) for the acute management of strangulated<br />
inguino-crural <strong>hernia</strong>s: a report of nine cases. Hernia 2008;12:185-<br />
188.<br />
38. Deeba S, Purkayasta S, Paraskevas P, Athanasiou T, Darzi A, Zacharakis<br />
E. Laparoscopic approach to incarcerated and strangulated <strong>inguinal</strong><br />
<strong>hernia</strong>s. J Soc Laparoendosc Surg 2009;13:327-331.<br />
Volume 80, No. 4, July-August 2012 341