Governmental 457(b) Plan Massachusetts Deferred Compensation
Governmental 457(b) Plan Massachusetts Deferred Compensation
Governmental 457(b) Plan Massachusetts Deferred Compensation

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
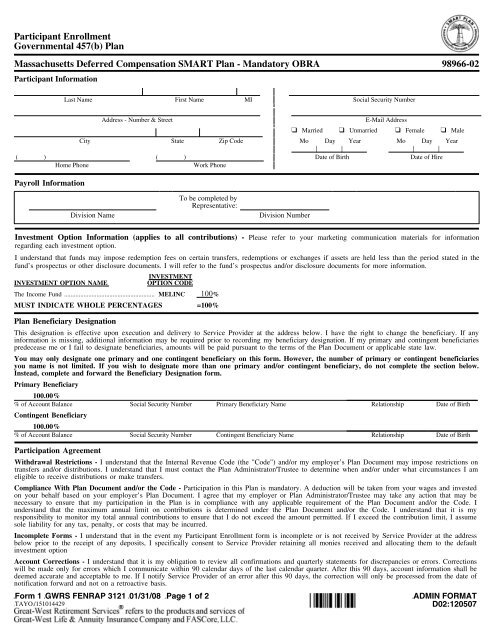
Participant Enrollment<br />
<strong>Governmental</strong> <strong>457</strong>(b) <strong>Plan</strong><br />
<strong>Massachusetts</strong> <strong>Deferred</strong> <strong>Compensation</strong> SMART <strong>Plan</strong> 98966-01<br />
Participant Participant<br />
Participant Information Enrollment<br />
Enrollment<br />
<strong>Governmental</strong> <strong>Governmental</strong> <strong>457</strong>(b) <strong>457</strong>(b) <strong>Plan</strong><br />
<strong>Plan</strong><br />
Last Name First Name MI Social Security Number<br />
<strong>Massachusetts</strong> <strong>Massachusetts</strong> <strong>Deferred</strong> <strong>Deferred</strong> <strong>Compensation</strong> <strong>Compensation</strong> SMART SMART <strong>Plan</strong> <strong>Plan</strong> - Mandatory OBRA 98966-02 98966-01 98966-02<br />
Participant Participant<br />
Information<br />
Information Address - Number & Street E-Mail Address<br />
Participant Enrollment<br />
❑ Married ❑ Unmarried ❑ Female ❑ Male<br />
<strong>Governmental</strong> Last Name First Name MI Social Security Number<br />
Last Name <strong>457</strong>(b) City <strong>Plan</strong><br />
State First Name Zip CodeMI Mo Day Year Social Security Number Mo Day Year<br />
| | | |<br />
<strong>Massachusetts</strong> ( ) <strong>Deferred</strong> Address <strong>Compensation</strong> - Number & ( Street SMART ) <strong>Plan</strong> - Mandatory OBRADate of Birth E-Mail Address Date of Hire98966-02<br />
Address - Number & Street E-Mail Address<br />
Home Phone Work Phone<br />
❑ Married ❑ Unmarried ❑ Female ❑ Male<br />
Participant Information<br />
❑ Married ❑ Unmarried ❑ Female ❑ Male<br />
City State Zip Code Mo Day Year Mo Day Year<br />
Payroll Information City State Zip Code Mo Day Year Mo Day Year<br />
| | | |<br />
❑ ( I elect ) to Last contribute Name % or ( $ First<br />
) Name (per MI | |<br />
pay period) of my Date compensation of Birth Social as Security before-tax Number | |<br />
Date contributions of Hire to the<br />
(<br />
<strong>Governmental</strong><br />
)<br />
Home Phone <strong>457</strong>(b) <strong>Deferred</strong> <strong>Compensation</strong><br />
(<br />
<strong>Plan</strong><br />
)<br />
until Work such Phone time as I revoke or amend my election.<br />
Date of Birth Date of Hire<br />
Home Phone Work Phone<br />
Home Phone Work Phone<br />
Payroll Address Effective - Number Date: & Street | |<br />
E-Mail Address<br />
Payroll Information<br />
Mo Day Year<br />
Investment<br />
Investment<br />
Option<br />
Option<br />
Information<br />
Information<br />
(applies<br />
(applies<br />
to<br />
to<br />
all<br />
all<br />
contributions)<br />
contributions)<br />
- Please<br />
Please<br />
refer<br />
refer<br />
to<br />
to ❑ your<br />
your Married marketing<br />
marketing ❑ Unmarried communication<br />
communication❑materials materials Female for<br />
for❑information information Male<br />
regarding<br />
regarding<br />
❑ I elect each<br />
each<br />
toinvestment investment option.<br />
contribute City option. % or $ State To be completed Zip Code by<br />
(per pay period) of Mo my Day compensation Year as before-tax Mo contributions Day Year to the<br />
<strong>Governmental</strong> <strong>457</strong>(b) <strong>Deferred</strong> <strong>Compensation</strong> <strong>Plan</strong> until such time as I revoke or amend my election.<br />
I understand<br />
understand<br />
that<br />
that<br />
funds<br />
funds<br />
may<br />
may<br />
impose<br />
impose<br />
redemption<br />
redemption<br />
fees<br />
fees<br />
on<br />
on<br />
certain<br />
certain Representative: transfers,<br />
transfers,<br />
redemptions<br />
redemptions<br />
or<br />
or<br />
exchanges<br />
exchanges |<br />
if<br />
if<br />
assets<br />
assets |<br />
are<br />
are<br />
held<br />
held<br />
less<br />
less<br />
than<br />
than<br />
the<br />
the |<br />
period<br />
period |<br />
stated<br />
stated<br />
in<br />
in<br />
the<br />
the<br />
fund’s<br />
fund’s (<br />
prospectus<br />
prospectus )<br />
or<br />
or<br />
Division other<br />
other Payroll disclosure<br />
disclosure<br />
NameEffective<br />
documents.<br />
documents. Date: (<br />
I will<br />
will<br />
refer<br />
refer ) | to<br />
to<br />
the<br />
the<br />
fund’s<br />
fund’s | prospectus<br />
prospectus<br />
Division and/or<br />
and/or<br />
Number disclosure<br />
disclosure Date<br />
documents<br />
documents of Birth<br />
for<br />
for<br />
more<br />
more<br />
information.<br />
information. Date of Hire<br />
Home Phone INVESTMENT Mo Work DayPhone Year<br />
INVESTMENT OPTION NAME<br />
OPTION<br />
INVESTMENT<br />
CODE<br />
INVESTMENT OPTION NAME<br />
OPTION CODE<br />
The Investment Income Fund Option ........................................................ Information (applies (appliesMELINC to all To contributions) be completed % by - Please refer to your marketing communication materials for information<br />
The regarding Income each Fund investment ........................................................ option.<br />
MELINC Representative: %<br />
MUST<br />
MUST INDICATE<br />
I understand that funds<br />
Division<br />
WHOLE<br />
may<br />
Name<br />
PERCENTAGES =100%<br />
impose redemption fees on certain transfers, redemptions<br />
Division<br />
or<br />
Number<br />
I understand<br />
INDICATE<br />
that funds<br />
WHOLE<br />
may impose<br />
PERCENTAGES<br />
redemption fees on certain<br />
=100%<br />
transfers, redemptions or exchanges if assets are held less than the period stated in the<br />
<strong>Plan</strong> fund’s Beneficiary prospectus or Designation<br />
other disclosure documents. I will refer to the fund’s prospectus and/or disclosure documents for more information.<br />
<strong>Plan</strong> Beneficiary Designation<br />
This Investment designation Option is effective Information upon execution (applies INVESTMENT<br />
to all contributions) - Please refer to your marketing communication INVESTMENT materials for information<br />
This<br />
and delivery to Service Provider at the address below. I have the right to change the beneficiary. If any<br />
INVESTMENT<br />
information INVESTMENT regarding designation each is missing,<br />
OPTION investment is effective<br />
additional<br />
NAME option. upon execution<br />
information OPTION and delivery<br />
may be CODE<br />
to Service Provider INVESTMENT at the address OPTION below. NAME I have the right to OPTION change CODE the beneficiary. If any<br />
information is missing, additional information may be required<br />
required<br />
prior<br />
prior<br />
to<br />
to<br />
recording<br />
recording<br />
my<br />
my<br />
beneficiary<br />
beneficiary<br />
designation.<br />
designation.<br />
If<br />
If<br />
my<br />
my<br />
primary<br />
primary<br />
and<br />
and<br />
contingent<br />
contingent<br />
beneficiaries<br />
beneficiaries<br />
predecease The predecease SMARTPath I understand Income me Fund me 2000 that or<br />
or ........................................................ Retirement I funds fail<br />
fail<br />
to<br />
to<br />
may designate<br />
designate Fund impose ........................... beneficiaries,<br />
beneficiaries,<br />
redemption MELINC SMPT00 fees amounts<br />
amounts<br />
on certain will<br />
will 100<br />
be<br />
be<br />
transfers, %<br />
paid<br />
paid<br />
pursuant<br />
pursuant<br />
redemptions State to<br />
to Street the<br />
the<br />
terms<br />
terms Russ or exchanges 2000 of<br />
of<br />
the<br />
the Ind <strong>Plan</strong><br />
<strong>Plan</strong> Sec if assets Lnd Document<br />
Document Ser are A .................. held or<br />
or<br />
applicable<br />
applicable<br />
less SVR2IS than state the<br />
state<br />
period law.<br />
law.<br />
stated % in the<br />
SMARTPath fund’s prospectus 2005 Retirement or other disclosure Fund ........................... documents. SMPT05 I will refer to the % fund’s prospectus Fidelity Fund and/or ............................................................... disclosure documents for more information.<br />
FFIDX %<br />
You<br />
You MUST may<br />
may INDICATE only<br />
only<br />
designate<br />
designate WHOLE one<br />
one<br />
primary PERCENTAGES primary<br />
and<br />
and<br />
one<br />
one<br />
contingent<br />
contingent =100% beneficiary<br />
beneficiary<br />
on<br />
on<br />
this<br />
this<br />
form.<br />
form.<br />
However,<br />
However,<br />
the<br />
the<br />
number<br />
number<br />
of<br />
of<br />
primary<br />
primary<br />
or<br />
or<br />
contingent<br />
contingent<br />
beneficiaries<br />
beneficiaries<br />
SMARTPath 2010 Retirement Fund ...........................<br />
INVESTMENT<br />
SMPT10 % Eaton Vance Large Cap Value Eq Com Tr .................<br />
INVESTMENT<br />
ETCLCV %<br />
you<br />
you<br />
name<br />
name<br />
is<br />
is<br />
not<br />
not<br />
limited.<br />
limited.<br />
If<br />
If<br />
you<br />
you<br />
wish<br />
wish<br />
to<br />
to<br />
designate<br />
designate<br />
more<br />
more<br />
than<br />
than<br />
one<br />
one<br />
primary<br />
primary<br />
and/or<br />
and/or<br />
contingent<br />
contingent<br />
beneficiary,<br />
beneficiary,<br />
do<br />
do<br />
not<br />
not<br />
complete<br />
complete<br />
the<br />
the<br />
section<br />
section<br />
below.<br />
below.<br />
Instead, INVESTMENT Instead, <strong>Plan</strong> SMARTPath Beneficiary complete<br />
complete 2015 OPTION Retirement and<br />
and Designation forward<br />
forward NAME Fund ........................... the<br />
the<br />
Beneficiary<br />
Beneficiary OPTION SMPT15 Designation<br />
Designation CODE form.<br />
form. % INVESTMENT KLD 400 Social OPTION Index Series NAME Fund ............................ OPTION KLD400 CODE %<br />
Primary SMARTPath<br />
SMARTPath Beneficiary 2000<br />
2020<br />
Retirement<br />
Retirement<br />
Fund<br />
Fund<br />
...........................<br />
...........................<br />
SMPT00<br />
SMPT20<br />
%<br />
State<br />
State<br />
Street<br />
Street<br />
Russ<br />
S&P 500<br />
2000<br />
Flagship<br />
Ind Sec<br />
Series<br />
Lnd Ser<br />
A .....................<br />
A .................. SVR2IS<br />
SV500<br />
%<br />
Primary This designation Beneficiary is effective upon execution and delivery to Service Provider at the address below. I have the right to change the beneficiary. If any<br />
information SMARTPath<br />
SMARTPath<br />
100.00% 2005<br />
2025 is missing, Retirement<br />
Retirement additional Fund<br />
Fund<br />
...........................<br />
........................... information may SMPT05<br />
SMPT25 be required prior % to recording Fidelity<br />
Fidelity my Fund<br />
Growth beneficiary ...............................................................<br />
Company designation. Fund ................................. If my primary FFIDX<br />
FD-GRO and contingent beneficiaries<br />
%<br />
% predecease SMARTPath<br />
SMARTPath 100.00%<br />
of Account me 2010<br />
2030 Balance or Retirement<br />
Retirement I fail to designate Fund<br />
Fund<br />
...........................<br />
........................... beneficiaries, Social Security SMPT10<br />
SMPT30 amounts Number will be % Primary paid pursuant Beneficiary Eaton<br />
T Rowe to Vance the Price Name terms Large<br />
Structured of Cap the Value<br />
Research <strong>Plan</strong> Eq Document Com<br />
Comm<br />
Tr .................<br />
Tr ............. or Relationship applicable ETCLCV<br />
TRSRCT state law. Date % of Birth<br />
%<br />
SMARTPath<br />
SMARTPath<br />
of Account<br />
2015<br />
2035<br />
Balance<br />
Retirement<br />
Retirement<br />
Fund<br />
Fund<br />
...........................<br />
...........................<br />
Social Security<br />
SMPT15<br />
SMPT35<br />
Number<br />
%<br />
Primary Beneficiary<br />
KLD<br />
State Street<br />
Name<br />
400 Social<br />
Pass<br />
Index<br />
Tr Infl<br />
Series<br />
Pt Sc<br />
Fund<br />
Ind NL<br />
............................<br />
A .....................<br />
Relationship<br />
KLD400<br />
SVPTIP<br />
Date<br />
%<br />
of Birth<br />
Contingent You may only Beneficiary designate one primary and one contingent beneficiary on this form. However, the number of primary or contingent beneficiaries<br />
Contingent you SMARTPath<br />
SMARTPath name is 2020<br />
2040 Beneficiary not Retirement<br />
Retirement limited. Fund<br />
Fund If you ...........................<br />
........................... wish to designate SMPT20<br />
SMPT40 more than % one primary State<br />
PIMCO<br />
Street and/or High<br />
S&P<br />
Yield contingent 500<br />
Fund<br />
Flagship<br />
- Institutional beneficiary, Series A .....................<br />
..................... do not complete SV500<br />
PHIYX the section % below.<br />
Instead,<br />
SMARTPath<br />
SMARTPath 100.00%<br />
100.00% complete<br />
2025<br />
2045<br />
Retirement<br />
Retirement and forward<br />
Fund<br />
Fund<br />
...........................<br />
........................... the Beneficiary<br />
SMPT25<br />
SMPT45 Designation form.<br />
%<br />
Fidelity<br />
PIMCO<br />
Growth<br />
Total Return<br />
Company<br />
- Inst.<br />
Fund<br />
........................................<br />
................................. FD-GRO<br />
PTTRX<br />
%<br />
%<br />
SMARTPath<br />
SMARTPath<br />
of Account<br />
2030<br />
2050<br />
Balance<br />
Retirement<br />
Retirement<br />
Fund<br />
Fund<br />
...........................<br />
...........................<br />
Social Security<br />
SMPT30<br />
SMPT50<br />
Number<br />
%<br />
Contingent Beneficiary<br />
T<br />
State<br />
Rowe<br />
Street<br />
Name<br />
Price<br />
Pass<br />
Structured<br />
Bd Mkt<br />
Research<br />
Ind Sec Lnd<br />
Comm<br />
A ....................<br />
Relationship<br />
Tr ............. TRSRCT<br />
SVPBMI<br />
Date<br />
%<br />
of Birth<br />
% Primary of Account Beneficiary Balance Social Security Number Contingent Beneficiary Name Relationship Date of Birth<br />
SMARTPath<br />
State Street Daily<br />
2035<br />
EAFE<br />
Retirement<br />
Sec Lnd<br />
Fund<br />
Series<br />
...........................<br />
T .................<br />
SMPT35<br />
SVEAFT<br />
%<br />
State<br />
The Income<br />
Street Pass<br />
Fund<br />
Tr<br />
........................................................<br />
Infl Pt Sc Ind NL A ..................... SVPTIP<br />
MELINC<br />
%<br />
Participation 100.00%<br />
Participation<br />
Agreement<br />
SMARTPath<br />
INVESCO Equity Agreement<br />
2040<br />
Real<br />
Retirement<br />
Estate Sec<br />
Fund<br />
Tr<br />
...........................<br />
Cl MA .............<br />
SMPT40<br />
IVERES<br />
%<br />
PIMCO<br />
Vanguard<br />
High<br />
Reserve<br />
Yield<br />
Prime<br />
Fund<br />
Money<br />
- Institutional<br />
Market<br />
.....................<br />
Inst ............<br />
PHIYX<br />
VMRXX<br />
%<br />
% of Account Balance Social Security Number Primary Beneficiary Name Relationship Date of Birth<br />
Withdrawal SMARTPath<br />
Active Withdrawal Small<br />
2045<br />
Cap Restrictions<br />
Restrictions Stock<br />
Retirement<br />
Portfolio - I<br />
Fund I understand ............................... understand that the<br />
........................... that the SMPT45<br />
WELASC Internal<br />
Internal<br />
Revenue<br />
Revenue<br />
% Code<br />
Code<br />
(the<br />
(the "Code") and/or my employer’s <strong>Plan</strong> Document may impose restrictions on<br />
transfers and/or distributions. I understand that I must contact the <strong>Plan</strong> Administrator/Trustee<br />
MUST PIMCO "Code") Total INDICATE and/or Return my<br />
to - WHOLE<br />
determine Inst. employer’s ........................................ PERCENTAGES <strong>Plan</strong> Document<br />
when and/or under PTTRX may impose<br />
what circumstances<br />
=100% restrictions % on<br />
transfers<br />
Contingent I am<br />
SMARTPath and/or<br />
Beneficiary<br />
eligible to receive 2050 distributions. Retirement distributions Fund I understand<br />
or ........................... that<br />
make transfers. SMPT50 I must contact the % <strong>Plan</strong> Administrator/Trustee State Street Pass Bd to Mkt determine Ind Sec Lnd when A .................... and/or under SVPBMI what circumstances % I am<br />
eligible<br />
State Street<br />
100.00% to receive distributions or make transfers.<br />
Daily EAFE Sec Lnd Series T ................. SVEAFT % The Income Fund ........................................................ MELINC %<br />
Compliance<br />
Compliance % of Account Balance With <strong>Plan</strong> Document and/or Social the Security Code Number - Participation Contingent in this <strong>Plan</strong> Beneficiary is mandatory. Name A deduction will be taken Relationship from your wagesDate andof invested Birth<br />
on INVESCO your behalf Equity With<br />
based Real <strong>Plan</strong> Estate Document<br />
on your Sec Tr employer’s Cl and/or MA ............. the<br />
<strong>Plan</strong> IVERES Code - Participation<br />
Document. I agree % in this <strong>Plan</strong><br />
that my Vanguard is mandatory.<br />
employer Reserve or <strong>Plan</strong> Prime A deduction<br />
Administrator/Trustee Money Market will be Inst taken ............ from<br />
may take VMRXX your wages and<br />
any action that % invested<br />
on your behalf based on your employer’s <strong>Plan</strong> Document. I agree that my employer or <strong>Plan</strong> Administrator/Trustee may take any action that may<br />
may<br />
be<br />
be<br />
necessary Active Participation Small to Cap ensure Agreement<br />
Stock that Portfolio my ............................... participation in the WELASC <strong>Plan</strong> is in compliance %<br />
necessary to ensure that my participation in the <strong>Plan</strong> is in compliance with<br />
with MUST any<br />
any INDICATE applicable<br />
applicable<br />
requirement<br />
requirement WHOLE PERCENTAGES of<br />
of<br />
the<br />
the<br />
<strong>Plan</strong><br />
<strong>Plan</strong><br />
Document<br />
Document<br />
and/or<br />
and/or =100% the<br />
the<br />
Code.<br />
Code.<br />
I<br />
understand<br />
understand that the maximum annual limit on contributions is determined under the <strong>Plan</strong> Document and/or the Code. I understand that it is my<br />
responsibility Withdrawal<br />
that<br />
Restrictions<br />
the maximum<br />
to monitor my - Itotal understand<br />
annual limit<br />
annual that<br />
on<br />
contributions the<br />
contributions<br />
Internal to ensure Revenue<br />
is determined<br />
that Code I do (the<br />
under<br />
not "Code")<br />
the<br />
exceed the and/or<br />
<strong>Plan</strong><br />
amount my<br />
Document<br />
employer’s<br />
and/or<br />
permitted. If <strong>Plan</strong><br />
the<br />
I exceed Document<br />
Code. I<br />
the contribution may<br />
understand<br />
impose<br />
that<br />
limit, restrictions<br />
it is my<br />
I assume on<br />
responsibility<br />
sole transfers liability and/or<br />
to<br />
for distributions.<br />
monitor my total<br />
any tax, penalty, I understand<br />
annual contributions<br />
or costs that may I must<br />
to<br />
be incurred. contact<br />
ensure<br />
the<br />
that<br />
<strong>Plan</strong><br />
I do<br />
Administrator/Trustee<br />
not exceed the amount<br />
to determine<br />
permitted.<br />
when<br />
If I exceed<br />
and/or<br />
the<br />
under<br />
contribution<br />
what circumstances<br />
limit, I assume<br />
I am<br />
sole<br />
eligible<br />
liability<br />
to receive<br />
for any<br />
distributions<br />
tax, penalty,<br />
or<br />
or<br />
make<br />
costs<br />
transfers.<br />
that may be incurred.<br />
Incomplete<br />
Incomplete Forms - I understand that in the event my Participant Enrollment form is incomplete or is not received by Service Provider at the address<br />
Compliance<br />
Forms<br />
below prior to With the <strong>Plan</strong><br />
- I understand<br />
receipt Document<br />
that<br />
of any deposits, and/or<br />
in the<br />
the<br />
event<br />
I specifically Code<br />
my<br />
- Participation<br />
Participant Enrollment<br />
consent to inService this <strong>Plan</strong><br />
form<br />
Provider is mandatory.<br />
is incomplete<br />
retaining Aall deduction<br />
or is not<br />
monies will<br />
received<br />
received be taken<br />
by Service<br />
and from allocating your<br />
Provider<br />
them wages<br />
at<br />
to and<br />
the<br />
the invested<br />
address<br />
below<br />
default<br />
investment on your<br />
prior<br />
behalf<br />
to the<br />
option based<br />
receipt<br />
on your<br />
of any<br />
employer’s<br />
deposits,<br />
<strong>Plan</strong><br />
I specifically<br />
Document.<br />
consent<br />
I agree<br />
to<br />
that<br />
Service<br />
my employer<br />
Provider retaining<br />
or <strong>Plan</strong> Administrator/Trustee<br />
all monies received and<br />
may<br />
allocating<br />
take any<br />
them<br />
action<br />
to<br />
that<br />
the<br />
may<br />
default<br />
be<br />
investment<br />
necessary to<br />
option<br />
ensure that my participation in the <strong>Plan</strong> is in compliance with any applicable requirement of the <strong>Plan</strong> Document and/or the Code. I<br />
Account<br />
Account<br />
understand Corrections<br />
Corrections<br />
that the maximum - I understand<br />
understand<br />
annual that<br />
that<br />
limit it<br />
it<br />
is<br />
is<br />
on my<br />
my<br />
contributions obligation<br />
obligation<br />
to<br />
to<br />
is review<br />
review<br />
determined all<br />
all<br />
confirmations<br />
confirmations<br />
under the and<br />
and<br />
<strong>Plan</strong> quarterly<br />
quarterly<br />
Document statements<br />
statements<br />
and/or for the<br />
for<br />
discrepancies<br />
discrepancies<br />
Code. I understand or<br />
or<br />
errors.<br />
errors.<br />
that Corrections<br />
Corrections<br />
it is my<br />
will<br />
will<br />
responsibility be<br />
be<br />
made<br />
made<br />
only<br />
only<br />
to monitor for<br />
for<br />
errors<br />
errors<br />
my which<br />
which<br />
total annual I communicate<br />
communicate<br />
contributions within<br />
within<br />
to ensure 90<br />
90<br />
calendar<br />
calendar<br />
that I days<br />
days<br />
do not of<br />
of<br />
the exceed<br />
the<br />
last<br />
last<br />
the calendar<br />
calendar<br />
amount quarter.<br />
quarter.<br />
permitted. After<br />
After<br />
If this<br />
this<br />
I exceed 90<br />
90<br />
days,<br />
days,<br />
the account<br />
account<br />
contribution information<br />
information<br />
limit, I shall<br />
shall<br />
assume be<br />
be<br />
deemed<br />
deemed<br />
sole liability accurate<br />
accurate<br />
for any and<br />
and<br />
tax, acceptable<br />
acceptable<br />
penalty, to<br />
to<br />
or me.<br />
me.<br />
costs If<br />
If<br />
I that notify<br />
notify<br />
may Service<br />
Service<br />
be incurred. Provider<br />
Provider<br />
of<br />
of<br />
an<br />
an<br />
error<br />
error<br />
after<br />
after<br />
this<br />
this<br />
90<br />
90<br />
days,<br />
days,<br />
the<br />
the<br />
correction<br />
correction<br />
will<br />
will<br />
only<br />
only<br />
be<br />
be<br />
processed<br />
processed<br />
from<br />
from<br />
the<br />
the<br />
date<br />
date<br />
of<br />
of<br />
notification<br />
notification forward and not on a retroactive basis.<br />
Incomplete<br />
forward<br />
Forms -<br />
and<br />
I understand<br />
not on a retroactive<br />
that in the<br />
basis.<br />
event my Participant Enrollment form is incomplete or is not received by Service Provider at the address<br />
below prior to the receipt of any deposits, I specifically consent to Service Provider retaining all monies received and allocating them to the default<br />
investment option<br />
][Form 1 ][GWRS FENRAP ][01/31/08 ][Page 1 of 3<br />
][ADMIN FORMAT<br />
Account ][TAYO][/151014421 Corrections - I understand that it is my obligation to review all confirmations and quarterly statements for discrepancies or errors. D02:120507 Corrections<br />
will be made only for errors which I communicate within 90 calendar days of the last calendar quarter. After this 90 days, account information shall be<br />
deemed accurate and acceptable to me. If I notify Service Provider of an error after this 90 days, the correction will only be processed from the date of<br />
notification forward and not on a retroactive basis.<br />
][Form ][Form<br />
1 1<br />
][GWRS ][GWRS<br />
FENRAP FENRAP<br />
3121<br />
3121 ][01/31/08 ][01/31/08<br />
][01/31/08 ][Page ][Page<br />
][Page 1 of 31<br />
1<br />
of<br />
of<br />
2<br />
][ADMIN ][ADMIN<br />
FORMAT<br />
FORMAT<br />
][TAYO][/151014421<br />
][TAYO][/151014429<br />
][TAYO][/151014429<br />
D02:120507<br />
D02:120507
Last Name First Name MI Social Security Number<br />
Required Signatures - I have completed, understand and agree to all pages of this Participant Enrollment form. I understand that Service Provider is<br />
required to comply with the regulations and requirements of the Office of Foreign Assets Control, Department of the Treasury ("OFAC"). As a result,<br />
Service Provider cannot conduct business with persons in a blocked country or any person designated by OFAC as a specially designated national or<br />
blocked person. For more information, please access the OFAC Web site at: http://www.ustreas.gov/offices/eotffc/ofac. Deferral agreements must be<br />
entered into prior to the first day of the month that the deferral will be made.<br />
Participant Signature Date<br />
Registered Representative Signature and ID Date<br />
Participant forward to Service Provider at:<br />
Great-West Retirement Services®<br />
PO Box 173764<br />
Denver, CO 80217-3764<br />
Express Address:<br />
8515 E. Orchard Road, Greenwood Village, CO 80111<br />
Phone #: 1-877-<strong>457</strong>-1900<br />
Fax #: 1-866-745-5766<br />
][Form 1 ][GWRS FENRAP 3121 ][01/31/08 ][Page 2 of 2<br />
][TAYO][/151014429<br />
][ADMIN FORMAT<br />
D02:120507