To: Applicants/ Referring Agencies From: Family Services, Inc. RE ...
To: Applicants/ Referring Agencies From: Family Services, Inc. RE ...
To: Applicants/ Referring Agencies From: Family Services, Inc. RE ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
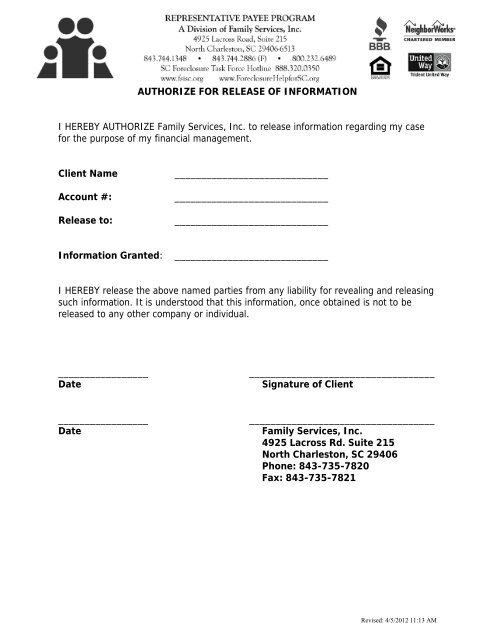
AUTHORIZE FOR <strong>RE</strong>LEASE OF INFORMATION<br />
I HE<strong>RE</strong>BY AUTHORIZE <strong>Family</strong> <strong>Services</strong>, <strong>Inc</strong>. to release information regarding my case<br />
for the purpose of my financial management.<br />
Client Name _____________________________<br />
Account #: _____________________________<br />
Release to: _____________________________<br />
Information Granted: _____________________________<br />
I HE<strong>RE</strong>BY release the above named parties from any liability for revealing and releasing<br />
such information. It is understood that this information, once obtained is not to be<br />
released to any other company or individual.<br />
_________________ ___________________________________<br />
Date Signature of Client<br />
_________________ ___________________________________<br />
Date <strong>Family</strong> <strong>Services</strong>, <strong>Inc</strong>.<br />
4925 Lacross Rd. Suite 215<br />
North Charleston, SC 29406<br />
Phone: 843-735-7820<br />
Fax: 843-735-7821<br />
Revised: 4/5/2012 11:13 AM