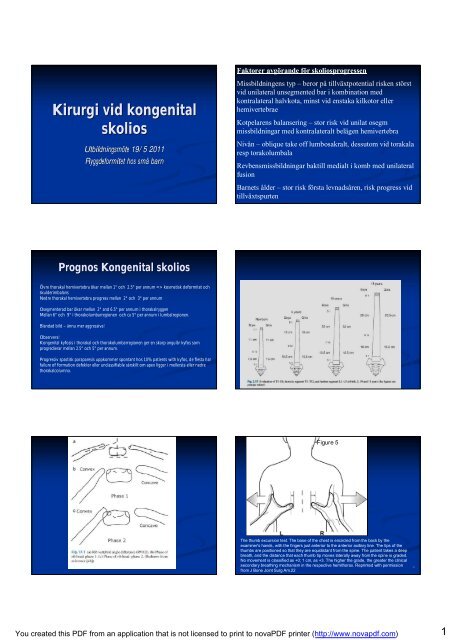
Kirurgi vid kongenital skolios
Kirurgi vid kongenital skolios
Kirurgi vid kongenital skolios

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>Kirurgi</strong> <strong>vid</strong> <strong>kongenital</strong><br />
<strong>skolios</strong><br />
Utbildningsmöte te 19/5 2011<br />
Ryggdeformitet hos små barn<br />
Faktorer avgörande för <strong>skolios</strong>progressen<br />
Missbildningens typ – beror på tillväxtpotential risken störst<br />
<strong>vid</strong> unilateral unsegmented bar i kombination med<br />
kontralateral halvkota, minst <strong>vid</strong> enstaka kilkotor eller<br />
hemivertebrae<br />
Kotpelarens balansering – stor risk <strong>vid</strong> unilat osegm<br />
missbildningar med kontralateralt belägen hemivertebra<br />
Nivån – oblique take off lumbosakralt, dessutom <strong>vid</strong> torakala<br />
resp torakolumbala<br />
Revbensmissbildningar baktill medialt i komb med unilateral<br />
fusion<br />
Barnets ålder – stor risk första levnadsåren, risk progress <strong>vid</strong><br />
tillväxtspurten<br />
Prognos Kongenital <strong>skolios</strong><br />
Övre thorakal hemivertebra ökar mellan 1° och 2.5° per annum => kosmetisk deformitet och<br />
skulderimbalans<br />
Nedre thorakal hemivertebra progress mellan 2° och 3° per annum<br />
Osegmenterad bar ökar mellan 2° and 6.5° per annum i thorakalryggen<br />
Mellan 6° och 9° i thorakolumbarregionen och ca 5° per annum i lumbalregionen.<br />
Blandad bild – ännu mer aggressiva!<br />
Observera!<br />
Kongenital kyfosis i thorakal och thorakolumbarregionen ger en skarp angulär kyfos som<br />
progredierar mellan 2.5° och 5° per annum.<br />
Progressiv spastisk paraparesis uppkommer spontant hos 10% patients with kyfos, de flesta har<br />
failure of formation defekter eller unclassifiable särskilt om apex ligger i mellersta eller nedre<br />
thorakalcolumna.<br />
Figure 5<br />
The thumb excursion test. The base of the chest is encircled from the back by the<br />
examiner's hands, with the fingers just anterior to the anterior axillary line. The tips of the<br />
thumbs are positioned so that they are equidistant from the spine. The patient takes a deep<br />
breath, and the distance that each thumb tip moves laterally away from the spine is graded.<br />
No movement is classified as +0; 1 cm, as +3. The higher the grade, the greater the clinical<br />
secondary breathing mechanism in the respective hemithorax. Reprinted with permission<br />
from J Bone Joint Surg Am.22<br />
8<br />
You created this PDF from an application that is not licensed to print to novaPDF printer (http://www.novapdf.com)<br />
1
Figure 6<br />
Figure 7<br />
Measuring the space available for the lung. The height of the hemithorax is defined as the<br />
distance from the middle of the most cephalad rib down to the center of the hemidiaphragm (A<br />
lines). A ratio, expressed as a percentage, is derived by di<strong>vid</strong>ing the height of the concave<br />
hemithorax by the height of the convex hemithorax, defining the space available for the lung. A<br />
variation of this measurement technique uses points on ribs at similar distances caudad to the<br />
hemidiaphragms (B lines) to define the inferior border of the hemithorax, with the width of a<br />
vertebra (X) measured laterally along the chosen ribs. Worsening values for the space available<br />
for the lung on sequential radiographs suggest longitudinal growth inhibition of the concave<br />
hemithorax, with progression of thoracic deformity.<br />
9<br />
Prevaluation with bolster bending films. Posteroanterior and<br />
lateral radiograph of a 16-year-old girl with progressive<br />
congenital scoliosis. A, B, Bolster bending films done showed<br />
correction of the primary thoracic curvature from 90[degrees] to<br />
72[degrees] and correction of the thoracolumbar curve from<br />
60[degrees] to 35[degrees] (C, D).<br />
10<br />
You created this PDF from an application that is not licensed to print to novaPDF printer (http://www.novapdf.com)<br />
2
Handläggning<br />
- behandling<br />
Tidig diagnos – innan utveckling av stor deformitet.<br />
Om risk för progress – tidig adekvat beh.<br />
Liten deformitet - Fusion in situ, convex<br />
hemiepiphysiodes<br />
Moderat deformitet – partiell korrektion genom<br />
instrumenterad fusion.<br />
Allvarlig deformitet – osteotomi/hemivertebrektomi<br />
- ökad risk neurologisk komplikation<br />
När r operera<br />
Operationsmetoder<br />
Krökar över 40 grader<br />
Ryggen ur balans<br />
Vänta på tillväxt<br />
Påverkan på andningsfunktion<br />
Sittfunktion<br />
1. Konventionell fusion<br />
Fusion in situ, ”growth arrest”<br />
Korrektion och fusion + instrumentering<br />
Osteotomy / hemivertebrectomy, korrektion, fusion och<br />
instrumentering.<br />
Risk Crank shaft om inte kombineras främre kirurgi –<br />
gäller inte moderna implantat med pedikelskruvar<br />
You created this PDF from an application that is not licensed to print to novaPDF printer (http://www.novapdf.com)<br />
3
2. VEPTR<br />
Operationsmetoder<br />
Expansion thoracoplasty<br />
Barn < 5år<br />
Thorax insufficiens syndrom<br />
MMC<br />
Missbildningar<br />
Operations-<br />
metoder<br />
3. Growing<br />
rods<br />
You created this PDF from an application that is not licensed to print to novaPDF printer (http://www.novapdf.com)<br />
4
You created this PDF from an application that is not licensed to print to novaPDF printer (http://www.novapdf.com)<br />
5
MMC<br />
Kyphotic deformity<br />
Sitting<br />
Flexible<br />
You created this PDF from an application that is not licensed to print to novaPDF printer (http://www.novapdf.com)<br />
6
You created this PDF from an application that is not licensed to print to novaPDF printer (http://www.novapdf.com)<br />
7