

Robinow Syndrome: An Update - GGH Journal
Robinow Syndrome: An Update - GGH Journal
Robinow Syndrome: An Update - GGH Journal

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Meinhard <strong>Robinow</strong>, MD<br />
Clinical Professor of Pediatrics<br />
Emeritus<br />
Wright State University School of<br />
Medicine<br />
Dayton, Ohio<br />
In 1969, Silverman, Smith, and I<br />
reported a family consisting of 3<br />
siblings, mother, and grandmother<br />
with "a previously unrecognized<br />
dwarfing syndrome."1 The major<br />
features were: moderately short stature,<br />
characteristic facial dysmorphism,<br />
genital hypoplasia, and<br />
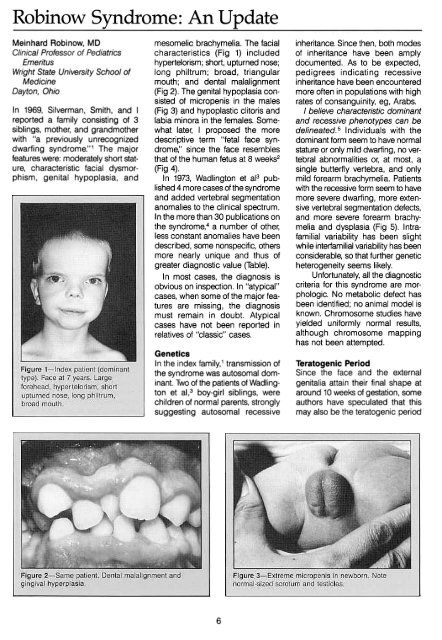
mesomelic brachymelia. The facial<br />
characteristics (Fig 1) included<br />
hypertelorism; short, upturned nose;<br />
long philtrum; broad, triangular<br />
mouth; and dental malalignment<br />
(Fig 2). The genital hypoplasia consisted<br />
of micropenis in the males<br />
(Fig 3) and hypoplastic clitoris and<br />
labia minora in the females. Somewhat<br />
later, I proposed the more<br />
descriptive term "fetal face syndrome,"<br />
since the face resembles<br />
that of the human fetus at 8 weeks2<br />
(Fig 4).<br />
In 1973, Wadlington et al3 published<br />
4 more cases of the syndrome<br />
and added vertebral segmentation<br />
anomalies to the clinical spectrum.<br />
In the more than 30 publications on<br />
the syndrome,4 a number of other,<br />
less constant anomalies have been<br />
described, some nonspecific, others<br />
more nearly unique and thus of<br />
greater diagnostic value (Table).<br />
In most cases, the diagnosis is<br />
obvious on inspection. In "atypical"<br />
cases, when some of the major features<br />
are missing, the diagnosis<br />
must remain in doubt. Atypical<br />
cases have not been reported in<br />
relatives of "classic" cases.<br />
Genetics<br />
In the index family,1 transmission of<br />
the syndrome was autosomal dominant.<br />
Two of the patients of Wadlington<br />
et al,3 boy-girl siblings, were<br />
children of normal parents, strongly<br />
suggesting autosomal recessive<br />
inheritance. Since then, both modes<br />
of inheritance have been amply<br />
documented. As to be expected,<br />
pedigrees indicating recessive<br />
inheritance have been encountered<br />
more often in populations with high<br />
rates of consanguinity, eg, Arabs.<br />
I believe characteristic dominant<br />
and recessive phenotypes can be<br />
delineated. 5 Individuals with the<br />
dominant form seem to have normal<br />
stature or only mild dwarfing, no vertebral<br />
abnormalities or, at most, a<br />
single butterfly vertebra, and only<br />
mild forearm brachymelia. Patients<br />
with the recessive form seem to have<br />
more severe dwarfing, more extensive<br />
vertebral segmentation defects,<br />
and more severe forearm brachymelia<br />
and dysplasia (Fig 5). Intrafamilial<br />
variability has been slight<br />
while interfamilial variability has been<br />
considerable, so that further genetic<br />
heterogeneity seems likely.<br />
Unfortunately, all the diagnostic<br />
criteria for this syndrome are morphologic.<br />
No metabolic defect has<br />
been identified; no animal model is<br />
known. Chromosome studies have<br />
yielded uniformly normal results,<br />
although chromosome mapping<br />
has not been attempted.<br />
Teratogenic Period<br />
Since the face and the external<br />
genitalia attain their final shape at<br />
around 10 weeks of gestation, some<br />
authors have speculated that this<br />
may also be the teratogenic period<br />
6
The Future<br />
Further studies of the phenotype are<br />
not likely to add much to present<br />
understanding. Progress will have to<br />
await metabolic and molecular genetic<br />
studies. Once the gene abnormality(ies)<br />
has (have) been identified,<br />
we can derive a better classification<br />
and may gain a better insight not<br />
only into the teratogenesis of the<br />
syndrome but also into mechanisms<br />
of normal embryogenesis.<br />
References<br />
1. <strong>Robinow</strong> M, Silverman FN, Smith HD.<br />
Am J Dis Child 1969;117:645-651.<br />
2. Patten MB. Human Embryo/og}( 3rd ed.<br />
New York, NY: Blakiston; 1968:346.<br />
3. Wadlington WB, Tucker VL, Schimke<br />
RM. Am J Dis Child 1973;126:202-205.<br />
4. Butler MG, Wadlington MB. <strong>Robinow</strong><br />
syndrome: report of two patients and<br />
review of the literature. Clin Genet 1987;<br />
31:77-85.<br />
5. <strong>Robinow</strong> M, Markert RJ. Proceed<br />
Greenwood Genet Center 1988;7:144.<br />
6. Lee PA, Migeon CJ, Brown TR,<br />
<strong>Robinow</strong> M. Am J Dis Child 1982;<br />
136:327-330.<br />
for the syndrome. However, vertebral<br />
segmentation is normally completed<br />
at 4 weeks, suggesting that teratogenesis<br />
is more extended, at least in<br />
the recessive type.<br />
Course<br />
Approximately 10% of patients have<br />
died in infancy, most of them of pulmonary<br />
disease or cardiac malformations.<br />
Probably all the deaths<br />
occurred in the recessive type. The<br />
remaining 90% seem to have<br />
enjoyed good health. The facial features<br />
become less striking at puber-ty,<br />
which may explain the fact that<br />
almost all index cases have been in<br />
infants and young children.<br />
Endocrine Aspects<br />
Sexual maturation occurs at the<br />
usual age in both sexes. In males,<br />
the penis remains abnormally short<br />
but may attain normal circumference,<br />
permitting sexual function.<br />
Endocrine studies by Lee et al6<br />
suggested partial primary hypogonadism.<br />
<strong>An</strong>drogen receptors and<br />
Sa-reductase in genital skin fibroblasts<br />
were normal. Females with<br />
both the dominant and recessive<br />
forms have reproduced, as have<br />
males with the dominant type. Reproduction<br />
by males with the recessive<br />
form has not yet been documented.<br />
7














