

Description of a case report of an intestinal-type ... - Cancer Therapy
Description of a case report of an intestinal-type ... - Cancer Therapy
Description of a case report of an intestinal-type ... - Cancer Therapy

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
C<strong>an</strong>cer <strong>Therapy</strong> Vol 6, page 1005<br />
C<strong>an</strong>cer <strong>Therapy</strong> Vol 6, 1005-1010, 2008<br />
<strong>Description</strong> <strong>of</strong> a <strong>case</strong> <strong>report</strong> <strong>of</strong> <strong>an</strong> <strong>intestinal</strong>-<strong>type</strong><br />
mucinous borderline ovari<strong>an</strong> tumor<br />
Case Report<br />
Raffaele Longo 1, *, Irnerio Angelo Muttillo 2 , Fr<strong>an</strong>cesca Cacciam<strong>an</strong>i 1 , Giuseppe Dal<br />
Sasso 2 , Lisa Luzzatto 2 , Mauro Simone 2 , Palmiro Masci 3 , Fr<strong>an</strong>cesco Torino 1 ,<br />
Giampietro Gasparini 1 , Aless<strong>an</strong>dro Mero 2<br />
1 Division <strong>of</strong> Medical Oncology, “S<strong>an</strong> Filippo Neri” Hospital Rome, Italy<br />
2 Division <strong>of</strong> Surgery <strong>an</strong>d Emergency, “S<strong>an</strong> Filippo Neri” Hospital Rome, Italy<br />
3 Division <strong>of</strong> Anathomy <strong>an</strong>d Pathology, “S<strong>an</strong> Filippo Neri” Hospital Rome, Italy<br />
__________________________________________________________________________________<br />
*Correspondence: Raffaele Longo, MD, Division <strong>of</strong> Medical Oncology ‘S<strong>an</strong> Filippo Neri’ Hospital, Via Martinotti 20, 00135 Rome,<br />
Italy; Tel: +39-06-33062272; Fax: +39-06-33062414; E-mail: raflongo@libero.it<br />
Key words: ovari<strong>an</strong> mucinous borderline tumors, ovari<strong>an</strong> surgery, adnexal masses, tumors <strong>of</strong> low malign<strong>an</strong>t potential<br />
Abbreviations: Borderline ovari<strong>an</strong> Tumors, (BOTs); intraoperative frozen section, (IFS); Mucinous Borderline Ovari<strong>an</strong> Tumor,<br />
(MBOT)<br />
Received: 27 October 2008; Revised: 24 November 2008<br />
Accepted: 3 December 2008; electronically published: December 2008<br />
Summary<br />
We <strong>report</strong> the <strong>case</strong> <strong>of</strong> a 53 year-old wom<strong>an</strong> hospitalized for <strong>an</strong> <strong>intestinal</strong> subocclusion syndrome due to a very large,<br />
multicystic mass occupying the whole abdominal cavity <strong>an</strong>d compressing the other intrabdominal org<strong>an</strong>s. The<br />
patient underwent surgical tumor resection with a radical hysterectomy <strong>an</strong>d bilateral salpingo-oophorectomy.<br />
Histology showed <strong>an</strong> <strong>intestinal</strong>-<strong>type</strong> mucinous borderline tumor (MBT) <strong>of</strong> the left ovary (diameter <strong>of</strong> 33x29x27cm;<br />
weight <strong>of</strong> 17 Kg) containing focal areas <strong>of</strong> “in situ” adenocarcinoma. After a follow-up <strong>of</strong> 19 months, the patient is<br />
now alive <strong>an</strong>d disease-free. Intestinal-<strong>type</strong> mucinous borderline ovari<strong>an</strong> tumors (MBOTs) are uncommon tumors <strong>of</strong><br />
large dimensions <strong>an</strong>d good prognosis. Surgery is the cornerstone in their m<strong>an</strong>agement. However, m<strong>an</strong>y issues<br />
remain unmet, including the extent <strong>of</strong> the staging procedure <strong>an</strong>d the optimal surgical approach, such as the use <strong>of</strong><br />
laparoscopy, conservative surgery, <strong>an</strong>d retroperitoneal lymph nodes dissection. Chemotherapy should be reserved<br />
only for progressive disease or in <strong>case</strong> <strong>of</strong> invasive peritoneal impl<strong>an</strong>ts that may not be surgically resected.<br />
I. Introduction<br />
Borderline ovari<strong>an</strong> Tumors (BOTs) were first<br />
described by Taylor in 1929 <strong>an</strong>d account for 10-20% <strong>of</strong> all<br />
epithelial ovari<strong>an</strong> c<strong>an</strong>cers (Wong et al, 2007). They are<br />
characterized by a degree <strong>of</strong> cellular proliferation <strong>an</strong>d<br />
nuclear atypia without aspects <strong>of</strong> infiltrative growth or<br />
stromal invasion. BOTs are typically present in younger<br />
women compared with invasive carcinomas, <strong>an</strong>d they are<br />
mostly diagnosed at <strong>an</strong> earlier stage, resulting in <strong>an</strong><br />
excellent prognosis. The 5-year overall survival rate for<br />
early-stage disease is approximately 98% <strong>an</strong>d varies<br />
between 86% <strong>an</strong>d 92% for more adv<strong>an</strong>ced disease (Hart,<br />
2005a,b; Wong et al, 2007).<br />
Histologically, BOTs c<strong>an</strong> be divided according to<br />
their epithelial characteristics as serous (50%), mucinous<br />
(46%), <strong>an</strong>d mixed, endometrioid, clear cell, or Brenner<br />
tumors (3.9%) (Hart, 2005a,b; Wong et al, 2007).<br />
We <strong>report</strong> the <strong>case</strong> <strong>of</strong> a large Mucinous Borderline<br />
Ovari<strong>an</strong> Tumor (MBOT) in a post-menopausal wom<strong>an</strong><br />
treated with a radical hysterectomy <strong>an</strong>d bilateral salpingooophorectomy.<br />
II. Case Report<br />
In March 2007, a 53 year-old post-menopausal wom<strong>an</strong> was<br />
hospitalized for abdominal distension <strong>an</strong>d pain, vomiting <strong>an</strong>d<br />
constipation.<br />
Physical examination revealed a large abdominal mass.<br />
Over the last year she had progressively gained weight despite a<br />
decreased appetite without <strong>an</strong>y other clinical sign or symptom <strong>of</strong><br />
the underlying disease.<br />
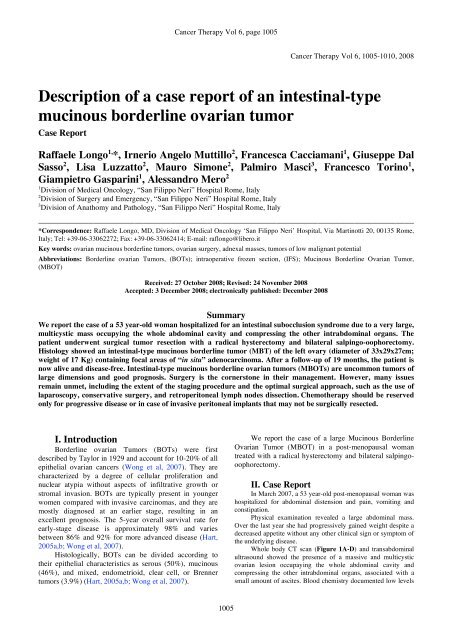
Whole body CT sc<strong>an</strong> (Figure 1A-D) <strong>an</strong>d tr<strong>an</strong>sabdominal<br />
ultrasound showed the presence <strong>of</strong> a massive <strong>an</strong>d multicystic<br />
ovari<strong>an</strong> lesion occupaying the whole abdominal cavity <strong>an</strong>d<br />
compressing the other intrabdominal org<strong>an</strong>s, associated with a<br />
small amount <strong>of</strong> ascites. Blood chemistry documented low levels<br />
1005
Longo et al: <strong>Description</strong> <strong>of</strong> a <strong>case</strong> <strong>report</strong> <strong>of</strong> <strong>an</strong> <strong>intestinal</strong>-<strong>type</strong> mucinous borderline ovari<strong>an</strong> tumor<br />
<strong>of</strong> total proteins with hypoalbuminemia. The serum level <strong>of</strong> CA-<br />
125 was 120 U/ml (normal r<strong>an</strong>ge < 35 U/ml).<br />
The patient underwent surgical resection <strong>of</strong> the tumor with<br />
hysterectomy, bilateral salpingo-oophorectomy, appendectomy<br />
<strong>an</strong>d infracolic omentectomy (Figure 2A). A careful inspection <strong>of</strong><br />
the peritoneum, associated to multiple r<strong>an</strong>dom biopsies,<br />
documented the absence <strong>of</strong> peritoneal tumor impl<strong>an</strong>ts. Peritoneal<br />
cytology was negative <strong>an</strong>d no enlarged retroperitoneal lymph<br />
nodes were also detected. Histology documented <strong>an</strong> <strong>intestinal</strong><strong>type</strong><br />
MBT <strong>of</strong> the left ovary (diameter <strong>of</strong> 33x29x27cm; weight <strong>of</strong><br />
17 Kg) (Figure 2B) containing focal areas <strong>of</strong> “in situ”<br />
adenocarciroma (Figure 2C, small arrows) <strong>an</strong>d aspects <strong>of</strong> early<br />
stromal desmoplastic reaction (Figure 2C, big arrows).<br />
The postoperative course was uneventful <strong>an</strong>d the patient<br />
was discharged 10 days post-operatively. After a follow up <strong>of</strong> 19<br />
months, the patient is alive, in good clinical conditions, <strong>an</strong>d<br />
disease-free as documented by a whole body CT sc<strong>an</strong> <strong>an</strong>d serum<br />
level <strong>of</strong> CA-125 that returned to within normal r<strong>an</strong>ges.<br />
III. Discussion<br />
BOTs represent approximately 10% to 20% <strong>of</strong> all<br />
ovari<strong>an</strong> malign<strong>an</strong>cies <strong>an</strong>d c<strong>an</strong> be quite large in size,<br />
particularly mucinous histo<strong>type</strong>. In 1988, two MBOT<br />
sub<strong>type</strong>s have been described: the <strong>intestinal</strong>-<strong>type</strong> (85%)<br />
<strong>an</strong>d the endocervical-like (Mulleri<strong>an</strong>) <strong>type</strong> (15%) (Acs,<br />
2005; Hart, 2005a,b; Wong et al, 2007). MBOTs,<br />
particularly the <strong>intestinal</strong>-<strong>type</strong>, c<strong>an</strong> be associated with<br />
pseudomyxoma peritonei (10%) <strong>an</strong>d necessitates a<br />
thorough investigation <strong>of</strong> the gastro<strong>intestinal</strong> tract with<br />
special attention to the appendix (Acs, 2005; Hart, 2005a;<br />
V<strong>an</strong>g et al, 2006).<br />
The endocervical-like <strong>type</strong> is clinically <strong>an</strong>d pathologically<br />
related to serous borderline tumors with which it is <strong>of</strong>ten<br />
mixed <strong>an</strong>d it is usually associated with endometriosis<br />
(Acs, 2005; Hart, 2005a; V<strong>an</strong>g et al, 2006). The <strong>intestinal</strong><strong>type</strong><br />
is much more common <strong>an</strong>d occurs over a very wide<br />
age r<strong>an</strong>ge (9-70 years), with a me<strong>an</strong> age <strong>of</strong> 35 years (Acs,<br />
2005; Hart, 2005a,b; Wong et al, 2007). Typically, it is<br />
characterized by large multicystic masses (me<strong>an</strong> diameter,<br />
17 cm) with smooth outer surfaces like benign mucinous<br />
cystadenomas (Acs, 2005; Hart, 2005a,b; Wong et al,<br />
2007). Over 90% <strong>of</strong> these tumors are unilateral <strong>an</strong>d may<br />
have <strong>an</strong> heterogeneous composition, with coexisting areas<br />
<strong>of</strong> cystadenoma, noninvasive carcinoma, <strong>an</strong>d sometimes<br />
occult areas <strong>of</strong> invasive carcinoma. For this reason, <strong>an</strong><br />
adequate sampling is particularly import<strong>an</strong>t (Acs, 2005;<br />
Hart, 2005a,b; V<strong>an</strong>g et al, 2006; Wong et al, 2007).<br />
Figure 1. Whole body CT sc<strong>an</strong> showed a massive <strong>an</strong>d multicystic ovari<strong>an</strong> lesion (arrows) occupaying the whole abdominal (A-C) <strong>an</strong>d<br />
pelvic (D) cavity <strong>an</strong>d compressing the other intrabdominal org<strong>an</strong>s, such as liver, spleen, <strong>an</strong>d kidneys.<br />
1006
C<strong>an</strong>cer <strong>Therapy</strong> Vol 6, page 1007<br />
Figure 2. At surgical abdominal examination, a very large left ovari<strong>an</strong> tumor was documented (diameter <strong>of</strong> 33x29x27cm; weight <strong>of</strong> 17<br />
Kg) (A). Histology showed <strong>an</strong> <strong>intestinal</strong>-<strong>type</strong> Mucinous Borderline Ovari<strong>an</strong> Tumor (B) containing focal areas <strong>of</strong> “in situ”<br />
adenocarciroma (C, small arrows) <strong>an</strong>d aspects <strong>of</strong> early stromal desmoplastic reaction (C, big arrows).<br />
Histologically, MBOTs are composed <strong>of</strong> multiple<br />
cysts <strong>an</strong>d gl<strong>an</strong>ds <strong>of</strong> various sizes that are lined by a<br />
mixture <strong>of</strong> cell <strong>type</strong>s, including endocervical-, gastric- <strong>an</strong>d<br />
goblet-<strong>type</strong> mucinous cells, which are generally stratified<br />
into no more th<strong>an</strong> two or three layers <strong>an</strong>d have slight-tomoderate<br />
nuclear atypia (Lee <strong>an</strong>d Scully, 2000; Acs, 2005;<br />
Hart, 2005a,b; V<strong>an</strong>g et al, 2006; Wong et al, 2007).<br />
Mitotic figures may be easily found <strong>an</strong>d areas <strong>of</strong> necrosis<br />
<strong>an</strong>d acute inflammation may be present (Lee <strong>an</strong>d Scully,<br />
2000; Acs, 2005; Hart, 2005a,b; V<strong>an</strong>g et al, 2006; Wong<br />
et al, 2007).<br />
One or multiple tiny foci <strong>of</strong> stromal invasion have<br />
been documented in up to 9% <strong>of</strong> MBOTs (Hart, 2005a,b).<br />
In most <strong>case</strong>s, individual microinvasive foci are less th<strong>an</strong><br />
1-2 mm <strong>an</strong>d may have several histological patterns (Hart,<br />
2005a,b).<br />
Small or large areas <strong>of</strong> noninvasive mucinous<br />
carcinoma occur in about 15-55% <strong>of</strong> otherwise typical<br />
MBOTs (Acs, 2005; Hart, 2005a,b). In this <strong>case</strong>,<br />
additional sampling is required to exclude overtly invasive<br />
areas <strong>of</strong> carcinoma that usually are related to a poor<br />
prognosis (Hart, 2005a).<br />
After a complete surgical treatment, almost all<br />
<strong>intestinal</strong>-<strong>type</strong> MBOTs are Stage I <strong>an</strong>d have <strong>an</strong> excellent<br />
prognosis with <strong>report</strong>ed metastatic rates <strong>of</strong> 0-7% <strong>an</strong>d 0-3%<br />
for tumors with or without noninvasive carcinoma areas,<br />
respectively (Klim<strong>an</strong> et al, 1986; Watkin et al, 1992;<br />
Kaern et al, 1993; Guerrieri et al, 1994; Nayar et al, 1996;<br />
Lee <strong>an</strong>d Scully, 2000; Rodriguez <strong>an</strong>d Prat, 2002; Ludwick<br />
et al, 2005; Kikkawa et al, 2006). In one <strong>of</strong> the largest<br />
<strong>report</strong>ed series <strong>of</strong> Stage I pure MBOTs, actuarial survival<br />
rates were 98% at 5 years <strong>an</strong>d 96% at 10 years (Lee <strong>an</strong>d<br />
Scully, 2000). More th<strong>an</strong> half <strong>of</strong> the tumors were treated<br />
by unilateral salpingo-oophorectomy.<br />
Tumors with noninvasive carcinoma also have a<br />
favorable prognosis (Klim<strong>an</strong> et al, 1986; Watkin et al,<br />
1992; Kaern et al, 1993; Guerrieri et al, 1994; Nayar et al,<br />
1996; Lee <strong>an</strong>d Scully, 2000; Rodriguez <strong>an</strong>d Prat, 2002;<br />
Ludwick et al, 2005; Kikkawa et al, 2006). They are<br />
usually Stage I tumors, although up to 7.2% <strong>of</strong> <strong>report</strong>ed<br />
<strong>case</strong>s in one literature review have been Stage II or III, <strong>an</strong>d<br />
almost 6% <strong>of</strong> 208 Stage I patients with noninvasive<br />
carcinoma recurred (Lee <strong>an</strong>d Scully, 2000).<br />
1007
Longo et al: <strong>Description</strong> <strong>of</strong> a <strong>case</strong> <strong>report</strong> <strong>of</strong> <strong>an</strong> <strong>intestinal</strong>-<strong>type</strong> mucinous borderline ovari<strong>an</strong> tumor<br />
Surgery is the cornerstone in the m<strong>an</strong>agement <strong>of</strong><br />
BOTs, but m<strong>an</strong>y issues exist on the extent <strong>of</strong> the staging<br />
procedure <strong>an</strong>d the optimal surgical approach, including the<br />
use <strong>of</strong> laparoscopy, conservative surgery, <strong>an</strong>d<br />
retroperitoneal lymph nodes dissection. Considering the<br />
clinical relev<strong>an</strong>ce <strong>of</strong> the stage in deciding treatment<br />
options, a careful inspection <strong>of</strong> the entire abdominal cavity<br />
with peritoneal washing, infracolic omentectomy, removal<br />
<strong>of</strong> all macroscopic suspicious peritoneal lesions, multiple<br />
peritoneal biopsies, <strong>an</strong>d, for MBOTs, appendectomy, are<br />
m<strong>an</strong>datory (Cadron et al, 2007). Unfortunately, complete<br />
staging is only performed in 50% or fewer patients, even<br />
though the pelvic peritoneum <strong>an</strong>d abdominal peritoneum<br />
are involved in 58% <strong>an</strong>d 48% <strong>of</strong> patients, respectively<br />
(Menzin et al, 2000; Cadron et al, 2007). Furthermore,<br />
invasive impl<strong>an</strong>ts are present in pelvic peritoneum <strong>an</strong>d<br />
abdominal peritoneum in 9% <strong>an</strong>d 14% <strong>of</strong> patients,<br />
respectively. The omentum is involved in 39% <strong>of</strong> patients,<br />
<strong>an</strong>d in 9% <strong>of</strong> patients, these impl<strong>an</strong>ts are invasive (Jones,<br />
2006; Cadron et al, 2007).<br />
Because younger women are more likely to develop<br />
BOTs, <strong>an</strong> import<strong>an</strong>t issue is the appropriateness <strong>of</strong><br />
conservative surgery with fertility preservation for stage I<br />
disease or for BOTs with noninvasive impl<strong>an</strong>ts. According<br />
to results <strong>of</strong> retrospective studies comparing conservative<br />
vs more radical approach, it seems reasonable to perform<br />
conservative surgery (ie, salpingo-oophorectomy with<br />
infracolic omentectomy <strong>an</strong>d multiple peritoneal biopsies<br />
<strong>an</strong>d cytology) only for stage I disease (Cadron et al,<br />
2007).Considering the increased risk <strong>of</strong> developing<br />
persistent invasive impl<strong>an</strong>ts or recurrence, patients with<br />
invasive impl<strong>an</strong>ts should be treated with radical surgery.<br />
In <strong>case</strong> <strong>of</strong> extraovari<strong>an</strong> recurrence with invasive impl<strong>an</strong>ts<br />
after conservative therapy, extensive cytoreductive surgery<br />
remains the treatment option <strong>of</strong> choice (Cadron et al,<br />
2007). The adv<strong>an</strong>tage <strong>of</strong> retroperitoneal lymph node<br />
sampling is questionable in patients with BOTs <strong>an</strong>d<br />
lymphadenectomy c<strong>an</strong> be omitted, even for the adv<strong>an</strong>ced<br />
disease, because it does not affect the recurrence or<br />
survival rate (Cho et al, 2006; Cadron et al, 2007). A<br />
recent prospective study conducted in 57 women with<br />
BOTs, para-aortic <strong>an</strong>d pelvic node dissection was not<br />
correlated to <strong>an</strong>y survival adv<strong>an</strong>tage (Pirimoglu et al,<br />
2008).<br />
Laparoscopy seems to be feasible in BOTs <strong>of</strong><br />
moderate size (diameter below 10 cm), to give fewer<br />
complications <strong>an</strong>d a shorter hospitalization (Cadron et al,<br />
2007; Daraï et al, 2007; Ødegaard et al, 2007). However,<br />
m<strong>an</strong>y potential concerns remain unmet, including the<br />
ch<strong>an</strong>ce <strong>of</strong> tumor rupture, the development <strong>of</strong> port site<br />
metastases, <strong>an</strong>d finally a potentially increased number <strong>of</strong><br />
patients with unstaged or inappropriately staged tumors.<br />
Future, prospective studies with a long-term follow-up are<br />
needed to determine the ultimate recurrence risk as well as<br />
fertility rates <strong>of</strong> this procedure as compared to laparotomy<br />
(Cadron et al, 2007).<br />
Chemotherapy should be reserved only for<br />
progressive disease that does not respond to surgical<br />
m<strong>an</strong>agement (Cadron et al, 2007).<br />
Finally, <strong>an</strong>other import<strong>an</strong>t issue is the intraoperative<br />
frozen section (IFS) diagnosis <strong>of</strong> BOTs. A recent<br />
retrospective <strong>an</strong>alysis comparing IFS <strong>an</strong>alysis <strong>an</strong>d<br />
definitive histology showed <strong>an</strong> agreement between these<br />
two procedures in 69/96 (71.9%) patients, yielding <strong>an</strong><br />
overall sensitivity <strong>an</strong>d a positive predictive value <strong>of</strong> 75.0%<br />
<strong>an</strong>d 94.5%, respectively. Underdiagnosis <strong>an</strong>d<br />
overdiagnosis occurred in 27/96 (28%) <strong>an</strong>d 0/96 (0%)<br />
patients, respectively. The authors concluded that surgical<br />
m<strong>an</strong>agement based on IFS diagnosis should be used with<br />
caution in BOT patients (Tempfer et al, 2007).<br />
In our <strong>case</strong>, considering tumor dimensions, the<br />
menopausal status <strong>an</strong>d the lack <strong>of</strong> peritoneal impl<strong>an</strong>ts <strong>an</strong>d<br />
locoregional lymph nodes involvement, the patient<br />
underwent radical surgical tumor resection without other<br />
adjuv<strong>an</strong>t treatments. After a follow up <strong>of</strong> 19 months, the<br />
patient is alive, in good clinical conditions, <strong>an</strong>d diseasefree<br />
References<br />
Acs G (2005) Serous <strong>an</strong>d mucinous borderline (low malign<strong>an</strong>t<br />
potential) tumors <strong>of</strong> the ovary. Am J Clin Pathol<br />
123(Suppl), S13-S57.<br />
Cadron I, Leunen K, V<strong>an</strong> Gorp T, Am<strong>an</strong>t F, Neven P, Vergote I<br />
(2007) M<strong>an</strong>agement <strong>of</strong> borderline ovari<strong>an</strong> neoplasms. J Clin<br />
Oncol 25, 2928-37.<br />
Cho YH, Kim DY, Kim JH, Kim YM, Kim KR, Kim YT, Nam<br />
JH (2006) Is complete surgical staging necessary in patients<br />
with stage I mucinous epithelial ovari<strong>an</strong> tumors? Gynecol<br />
Oncol 103, 878-82.<br />
Daraï E, Tulpin L, Prugnolle H, Cortez A, Dubernard G (2007)<br />
Laparoscopic restaging <strong>of</strong> borderline ovari<strong>an</strong> tumors. Surg<br />
Endosc 21, 2039-43.<br />
Guerrieri C, Hogberg T, Wingren S, Fristedt S, Simonsen E,<br />
Boeryd B (1994) Mucinous borderline <strong>an</strong>d malign<strong>an</strong>t tumors<br />
<strong>of</strong> the ovary. A clinicopathologic <strong>an</strong>d DNA ploidy study <strong>of</strong><br />
92 <strong>case</strong>s. C<strong>an</strong>cer 74, 2329-40.<br />
Hart WR (2005a) Borderline epithelial tumors <strong>of</strong> the ovary. Mod<br />
Pathol 18(Suppl 2), S33-S50.<br />
Hart WR (2005b) Mucinous tumors <strong>of</strong> the ovary: a review. Int J<br />
Gynecol Pathol 24, 4-25.<br />
Jones MB (2006) Borderline ovari<strong>an</strong> tumors: current concepts for<br />
prognostic factors <strong>an</strong>d clinical m<strong>an</strong>agement. Clin Obstet<br />
Gynecol 49,517-25.<br />
Kaern J, Tropé CG, Abeler VM (1993) A retrospective study <strong>of</strong><br />
370 borderline tumors <strong>of</strong> the ovary treated at the Norwegi<strong>an</strong><br />
Radium Hospital from 1970 to 1982: a review <strong>of</strong><br />
clinicopathologic features <strong>an</strong>d treatment modalities. C<strong>an</strong>cer<br />
71, 1810-20.<br />
Kikkawa F, Nawa A, Kajiyama H, Shibata K, Ino K, Nomura S<br />
(2006) Clinical characteristics <strong>an</strong>d prognosis <strong>of</strong> mucinous<br />
tumors <strong>of</strong> the ovary. Gynecol Oncol 103, 171-5.<br />
Klim<strong>an</strong> L, Rome RM, Fortune DW (1986) Low malign<strong>an</strong>t<br />
potential tumors <strong>of</strong> the ovary: a study <strong>of</strong> 76 <strong>case</strong>s. Obstet<br />
Gynecol 68, 338-44.<br />
Lee KR, Scully RE (2000) Mucinous tumors <strong>of</strong> the ovary: a<br />
clinicopathologic study <strong>of</strong> 196 borderline tumors (<strong>of</strong><br />
<strong>intestinal</strong> <strong>type</strong>) <strong>an</strong>d carcinomas, including <strong>an</strong> evaluation <strong>of</strong><br />
11 <strong>case</strong>s with “pseudomyxoma peritonei”. Am J Surg<br />
Pathol 24, 1447-64.<br />
Ludwick CL, Gilks CB, Miller D, Yaziji H, Clement PB (2005)<br />
Aggressive behavior <strong>of</strong> stage 1 ovari<strong>an</strong> mucinous tumors<br />
lacking extensive infiltrative invasion: a <strong>report</strong> <strong>of</strong> four <strong>case</strong>s<br />
<strong>an</strong>d review <strong>of</strong> the literature. Int J Gynecol Pathol 24, 205-<br />
17.<br />
1008
C<strong>an</strong>cer <strong>Therapy</strong> Vol 6, page 1009<br />
Menzin AW, Gal D, Lovecchio JL (2000) Contemporary surgical<br />
m<strong>an</strong>agement <strong>of</strong> borderline ovari<strong>an</strong> tumors: A survey <strong>of</strong> the<br />
Society <strong>of</strong> Gynecologic Oncologists. Gynecol Oncol 78, 7-9.<br />
Nayar R, Siriaunkgul S, Robbins KM, Mc Gowen L, Ginz<strong>an</strong> S,<br />
Silverberg SG (1996) Microinvasion in low malign<strong>an</strong>t<br />
potential tumors <strong>of</strong> the ovary. Hum Pathol 27, 521-7.<br />
Ødegaard E, Staff AC, L<strong>an</strong>gebrekke A, Engh V, Onsrud M<br />
(2007) Surgery <strong>of</strong> borderline tumors <strong>of</strong> the ovary:<br />
retrospective comparison <strong>of</strong> short-term outcome after<br />
laparoscopy or laparotomy. Acta Obstet Gynecol Sc<strong>an</strong>d 86,<br />
620-6.<br />
Pirimoglu ZM, Afsin Y, Guzelmeric K, Yilmaz M, Unal O,<br />
Tur<strong>an</strong> MC (2008) Is it necessary to do retroperitoneal<br />
evaluation in borderline epithelial ovari<strong>an</strong> tumors? Arch<br />
Gynecol Obstet 277, 411-4.<br />
Rodriguez IM, Prat J (2002) Mucinous tumors <strong>of</strong> the ovary: a<br />
clinicopathologic <strong>an</strong>alysis <strong>of</strong> 75 borderline tumors (<strong>of</strong><br />
<strong>intestinal</strong> <strong>type</strong>) <strong>an</strong>d carcinomas. Am J Surg Pathol 26, 139-<br />
52.<br />
Tempfer CB, Polterauer S, Bentz EK, Reinthaller A, Hefler LA<br />
(2007) Accuracy <strong>of</strong> intraoperative frozen section <strong>an</strong>alysis in<br />
borderline tumors <strong>of</strong> the ovary: a retrospective <strong>an</strong>alysis <strong>of</strong> 96<br />
<strong>case</strong>s <strong>an</strong>d review <strong>of</strong> the literature. Gynecol Oncol 107, 248-<br />
52.<br />
V<strong>an</strong>g R, Gown AM, Barry TS, Wheeler DT, Ronnett BM (2006)<br />
Ovari<strong>an</strong> atypical proliferative (borderline) mucinous tumors:<br />
gastro<strong>intestinal</strong> <strong>an</strong>d seromucinous (endocervical-like) <strong>type</strong>s<br />
are immunophenotypically distinctive. Int J Gynecol Pathol<br />
25, 83-9.<br />
Watkin W, Silva EG, Gershenson DM (1992) Mucinous<br />
carcinoma <strong>of</strong> the ovary: pathologic prognostic factors.<br />
C<strong>an</strong>cer 69, 208-12.<br />
Wong HF, Low JJ, Chua Y, Busm<strong>an</strong>is I, Tay EH, Ho TH (2007)<br />
Ovari<strong>an</strong> tumors <strong>of</strong> borderline malign<strong>an</strong>cy: a review <strong>of</strong> 247<br />
patients from 1991 to 2004. Int J Gynecol C<strong>an</strong>cer 17, 342-<br />
349.<br />
1009
Longo et al: <strong>Description</strong> <strong>of</strong> a <strong>case</strong> <strong>report</strong> <strong>of</strong> <strong>an</strong> <strong>intestinal</strong>-<strong>type</strong> mucinous borderline ovari<strong>an</strong> tumor<br />
1010




