T - Huntington's Disease Society of America
T - Huntington's Disease Society of America
T - Huntington's Disease Society of America

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Intoke: Regording your fomily membe/s core while home wiilr fomih-<br />
1. Who assisted u'ith self-care?<br />
\Vith u,hich tasks?<br />
Bothing: Dressing: Grooming: Toileting:<br />
Upper body- Upper bod-v- Brushing hair fusist with pants up/down -<br />
Lower bodv- Lorver body- Brushing teeth - Help complete task<br />
Hands/face -<br />
Socks/shoes - Shaving - Commode was used<br />
Underclothes only - Makeup - Bathroom was used<br />
Nail care -<br />
Which tasks were the most difficulti \\hvi<br />
2. \Ahen did assistance wirh homemaking skills become necessary?<br />
Which chores could your family member still perforn-r independentlyi<br />
Which chores could he or she Derform oart <strong>of</strong>?<br />
3. Sho assisted your family member with eating?<br />
\Vere there anv "tricks" that made<br />
this task easier? (such as using special cups or utensils, avoiding certain t-vpes <strong>of</strong> food, using special chairs or clothes)<br />
4. Please describe the position used by your family member while he or she was eating or being fed:<br />
Heod:<br />
Trunk (chest) Hips: Legs ([eet):<br />
Up - Forward - Back in chair - Flat on floor -<br />
Down _ Backward _ To one side ieft/right - Resring on stool -<br />
Foru,ard - Sidervays right/left - Fonvard in chair - In constant motion -<br />
Straight ahead - Upright -<br />
Under buttocks -<br />
Othei (please describe): Orher (please describe): Other (please describe):<br />
5. Did your family member have an,v difficulty sitting in a chair? Yes - No -<br />
Which type <strong>of</strong> chairs did he or she use? Sling back chair - Straight backed chair -<br />
Wheelchair - Lounge chair - Rocking chair - Recliner (e.g.,Lazy Boi€) - Didn t use a chair -<br />
Did you use anything to help your family member stay in the chair?<br />
A sheer tied around the chair - A tray placed over chair - Never used anything -<br />
\\hen did you use something to help your family member stay in the chairi<br />
During meals - In the morning - In the afternoon - In the evening - In the middle <strong>of</strong> the night -<br />
6. Did you need to help -vour family member u'alk? Yes - No -<br />
Did you provide a wheelchairl Yes - No -<br />
How did you help,vour family member walk?<br />
One person held onto belt - One person held onto hips - One person held onto arm -<br />
'livo<br />
Didn r let him/her rvalk - Tivo people on each arm - people held hands - Two people held onto belt -<br />
7. Is there anyrhing yor.d used during your family member's stay at home that made his or her stay easier for you?-<br />
ffiro<br />
Designed by Linda Anderson, OTNL, 1990<br />
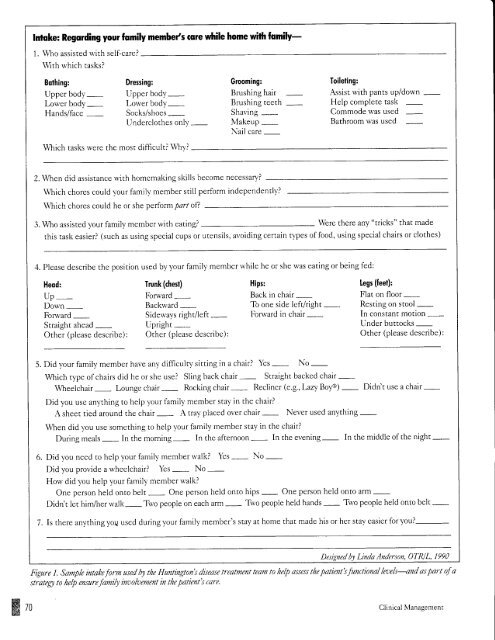
Figure 1. Sample intahe form used hy rhe <strong>Huntington's</strong> disease treatment€am to he lp assess tlte patient's functional lroels--and os part <strong>of</strong> a<br />
strateg to help ensurefamifinoolaement in the patient's care.<br />
Clinical Management