

vol45.3 LR.pdf - International Hospital Federation
vol45.3 LR.pdf - International Hospital Federation
vol45.3 LR.pdf - International Hospital Federation

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Management: Quality and funding<br />
Table 1. Incompatibilities of clinical paths and medical guidelines<br />
Table 1: Incompatibilities of clinical paths and medical guidelines<br />
Disease<br />
Medical methods missing from clinical paths<br />
Cardiogenic shock Neither the life-saving mechanical treatment through counterpulsation,<br />
nor the direct haemodynamic treatment through SwanGanz catheter<br />
are included in the medical algorithm<br />
AMI<br />
Discrepancies in the medication – GP IIB/IIA inhibitors are not<br />
reimbursed<br />
Hypertensive crisis<br />
No clinical path<br />
Pulmonary hypertension<br />
No clinical path<br />
CRT implantation<br />
No clinical path<br />
ICD implantation<br />
No clinical path<br />
Heart trauma<br />
No clinical path<br />
NSTEMI<br />
No clinical path<br />
Table guidelines 2: Incompatibilities of outpatient examinations and examinations by international medical guidelines<br />
Condition<br />
Missing compulsory examinations in compliance with medical guidelines<br />
50 – Congestive HF Lack of creatinine testing<br />
20 – Angina Pectoris Lack of cholesterol fractions testing, EchoCG and exercise test<br />
25.2 – previous<br />
Lack of cholesterol fractions testing, EchoCG and exercise test<br />
myocardial infarction<br />
25.3 – cardiac aneurysm Lack of cholesterol fractions testing, EchoCG and INR<br />
15 – secondary<br />
hypertension<br />
Lack of consultation with an endocrinologist and a nephrologist, no<br />
hormonal and creatinine testing<br />
27 – primary pulmonary<br />
Lack of pulmonary scintigraphy or pulmonary angiography<br />
hypertension<br />
31 – chronic pericarditis Lack of tuberculosis examination<br />
38 – endocarditis Lack of hemoculture examination<br />
171,4 – aneurysm of<br />
abdominal aorta<br />
Lack of lipid profile and EchoCG<br />
consider clinical paths an instrument for funding inpatient care.<br />
These mistakes urge doctors to use outdated and inadequate<br />
treatment methods, even where modern alternatives are available.<br />
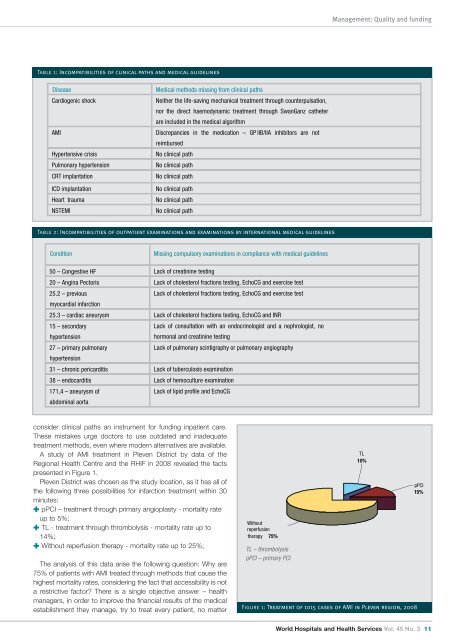
A study of AMI treatment in Pleven District by data of the<br />
Regional Health Centre and the RHIF in 2008 revealed the facts<br />
presented in Figure 1.<br />
Pleven District was chosen as the study location, as it has all of<br />
the following three possibilities for infarction treatment within 30<br />
minutes:<br />
✚ pPCI – treatment through primary angioplasty - mortality rate<br />
up to 5%;<br />
✚ TL - treatment through thrombolysis - mortality rate up to<br />
14%;<br />
✚ Without reperfusion therapy - mortality rate up to 25%;<br />
The analysis of this data arise the following question: Why are<br />
75% of patients with AMI treated through methods that cause the<br />
highest mortality rates, considering the fact that accessibility is not<br />
a restrictive factor? There is a single objective answer – health<br />
managers, in order to improve the financial results of the medical<br />
establishment they manage, try to treat every patient, no matter<br />
Without<br />
reperfusion<br />
therapy 75%<br />
TL – thrombolysis<br />
pPCI – primary PCI<br />
TL<br />
10%<br />
Figure 1: Treatment of 1015 cases of AMI in Pleven region, 2008<br />
pPCI<br />
15%<br />
World <strong>Hospital</strong>s and Health Services Vol. 45 No. 3 11














