*PHYORD* pre-operative physiCian orders - OhioHealth
*PHYORD* pre-operative physiCian orders - OhioHealth
*PHYORD* pre-operative physiCian orders - OhioHealth

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
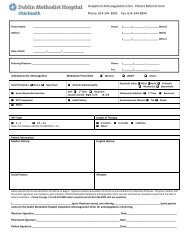
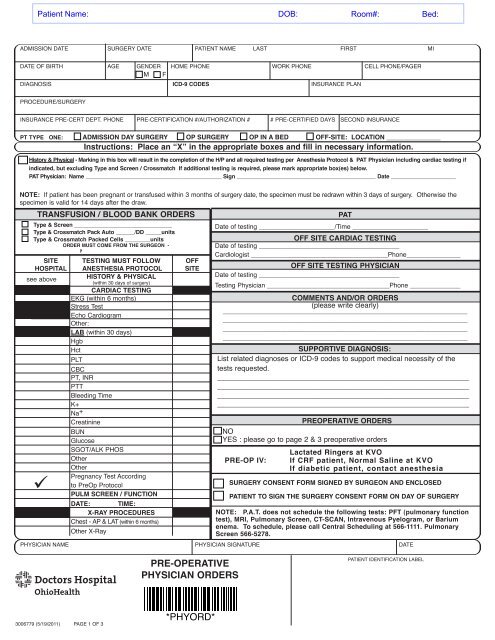
ADMISSION DATE SURGERY DATE PATIENT NAME LAST FIRST MI<br />
DATE OF BIRTH AGE GENDER HOME PHONE WORK PHONE CELL PHONE/PAGER<br />
M F<br />
DIAGNOSIS iCd-9 Codes INSURANCE PLAN<br />
PROCEDURE/SURGERY<br />
INSURANCE PRE-CERT DEPT. PHONE PRE-CERTIFICATION #/AUTHORIZATION # # PRE-CERTIFIED DAYS SECOND INSURANCE<br />
pt type one: admission day surgery op surgery op in a bed oFF-site: LoCation _______________<br />
instructions: place an “x” in the appropriate boxes and fill in necessary information.<br />
history & physical - marking in this box will result in the completion of the h/p and all required testing per anesthesia protocol & pat physician including cardiac testing if<br />
indicated, but excluding type and screen / Crossmatch if additional testing is required, please mark appropriate box(es) below.<br />
pat physician: name ____________________________________________ sign _____________________________________________ date _____________________<br />
note: If patient has been <strong>pre</strong>gnant or transfused within 3 months of surgery date, the specimen must be redrawn within 3 days of surgery. Otherwise the<br />
specimen is valid for 14 days after the draw.<br />
transFusion / bLood banK <strong>orders</strong><br />
type & screen _______________________________<br />
type & Crossmatch pack auto ______/dd _____units<br />
type & Crossmatch packed Cells ________units<br />
order must Come From the surgeon -<br />
not to be ordered by pat.<br />
site<br />
hospitaL<br />
see above<br />
¸<br />
testing must FoLLow<br />
anesthesia protoCoL<br />
history & physiCaL<br />
(within 30 days of surgery)<br />
CardiaC testing<br />
EKG (within 6 months)<br />
Stress Test<br />
Echo Cardiogram<br />
Other:<br />
Lab (within 30 days)<br />
Hgb<br />
Hct<br />
PLT<br />
CBC<br />
PT, INR<br />
PTT<br />
Bleeding Time<br />
K+<br />
Na +<br />
Creatinine<br />
BUN<br />
Glucose<br />
SGOT/ALK PHOS<br />
Other<br />
Other<br />
Pregnancy Test According<br />
to PreOp Protocol<br />
puLm sCreen / FunCtion<br />
date: time:<br />
x-ray proCedures<br />
Chest - AP & LAT (within 6 months)<br />
Other X-Ray<br />
oFF<br />
site<br />
pat<br />
Date of testing _____________________/Time _____________________<br />
oFF site CardiaC testing<br />
Date of testing _______________________________________<br />
Cardiologist ______________________________________Phone_______________<br />
oFF site testing <strong>physiCian</strong><br />
Date of testing _______________________________________<br />
Testing Physician __________________________________Phone ______________<br />
Comments and/or <strong>orders</strong><br />
(please write clearly)<br />
____________________________________________________________________<br />
____________________________________________________________________<br />
____________________________________________________________________<br />
____________________________________________________________________<br />
supportive diagnosis:<br />
List related diagnoses or ICD-9 codes to support medical necessity of the<br />
tests requested.<br />
________________________________________________________<br />
________________________________________________________<br />
________________________________________________________<br />
________________________________________________________<br />
<strong>pre</strong><strong>operative</strong> <strong>orders</strong><br />
NO<br />
YES : please go to page 2 & 3 <strong>pre</strong><strong>operative</strong> <strong>orders</strong><br />
<strong>pre</strong>-op iv:<br />
Lactated ringers at Kvo<br />
if CrF patient, normal saline at Kvo<br />
if diabetic patient, contact anesthesia<br />
surgery Consent Form signed by surgeon and enCLosed<br />
patient to sign the surgery Consent Form on day oF surgery<br />
note: p.a.t. does not schedule the following tests: pFt (pulmonary function<br />
test), mri, pulmonary screen, Ct-sCan, intravenous pyelogram, or barium<br />
enema. to schedule, please call Central scheduling at 566-1111. pulmonary<br />
screen 566-5278.<br />
PHYSICIAN NAME PHYSICIAN SIGNATURE DATE<br />
<strong>pre</strong>-<strong>operative</strong><br />
<strong>physiCian</strong> <strong>orders</strong><br />
PATIENT IDENTIFICATION LABEL<br />
3006779 (5/19/2011) PAGE 1 OF 3<br />
<strong>*PHYORD*</strong>
<strong>pre</strong>-<strong>operative</strong> <strong>physiCian</strong> <strong>orders</strong><br />
Name: _________________________________________ Time: _______________________ Date: _________________<br />
Instructions: Circle / Check box all <strong>orders</strong> that apply.<br />
required FieLd For aCCurate antibiotiC administration CaLCuLation<br />
CURRENT WEIGHT: _________________ lbs. _______________ kg. HEIGHT: ____________ ft. _______________ in.<br />
NKDA ALLERGY(S) & REACTIONS: ____________________________________________________________________________<br />
Latex Allergy No Yes – Reaction : ________________________ IVP Dye No Yes – Reaction : _____________________<br />
antibiotiC aLLergy: a positive response to one or more of the following 4 signs / symptoms:<br />
Respiratory difficulty (trouble breathing or chest tightness) Hypotension (low blood <strong>pre</strong>ssure or fainting)<br />
Immediate reaction of swelling or hives<br />
Emergency Room visit / Emergency visit to physician<br />
surgiCaL proCedure drug oF ChoiCe (iv) aLLergies to drug oF ChoiCe (iv)<br />
(antibiotiCs to be administered by anesthesia)<br />
(vanComyCin to be administered in <strong>pre</strong>op)<br />
GI (Gastrointestinal)<br />
General Surgery<br />
Cefoxitin 2 grams<br />
Cefazolin (dosing below) & metronidazole (Flagyl) 500mg<br />
1 gram if patient weight < 80 kg.<br />
2 grams if patient weight ≥ 80 kg.<br />
Clindamycin (dosing scale below) & gentamicin 80 mg<br />
600 mg if weight < 80 kg.<br />
900 mg if weight ≥ 80 kg.<br />
Vascular/ Thoracic<br />
Open Heart Procedures<br />
Neurological<br />
Ortho/Podiatry<br />
Implantable devices<br />
GU (Genitourinary)<br />
GYN and Urology<br />
Synthetic pubovaginal sling<br />
Head and Neck<br />
Major Soft Tissues<br />
Cefazolin<br />
1 gram if patient weight < 80 kg.<br />
2 grams if patient weight ≥ 80 kg.<br />
iF mrsa screening is negative or results unavailable and not<br />
allergic to Cefazolin<br />
Cefazolin<br />
1 gram if patient weight < 60 kg.<br />
2 grams if patient weight ≥ 60 kg.<br />
Bactroban : ½ tube each nostril<br />
Cefuroxime (Zinacef) 1.5gm<br />
Cefazolin<br />
1 gram if patient weight < 80 kg.<br />
2 grams if patient weight ≥ 80 kg<br />
Cefazolin<br />
1 gram if patient weight < 80 kg.<br />
2 grams if patient weight ≥ 80 kg<br />
if patient has a hx of staphlococcus aureus infection within<br />
the past 2 years<br />
Vancomycin (dosing scale below)<br />
1 gram if patient weighs < 80 kg<br />
1.5 gram if patients weighs ≥ 80 kg<br />
Cefazolin<br />
1 gram if patient weight < 80 kg.<br />
2 grams if patient weight ≥ 80 kg.<br />
Cefoxitin 2 grams<br />
Cefazolin<br />
1 gram if patient weight < 80 kg.<br />
2 grams if patient weight ≥ 80 kg.<br />
Vancomycin 1 gram<br />
Clindamycin<br />
600 mg if weight < 80 kg.<br />
900 mg if weight ≥ 80 kg.<br />
if mrsa screening is positive or allergic to Cefazolin<br />
Vancomycin (dosing scale below) & gentamicin 80 mg<br />
1 gram if patient weighs ≤ 65 kg<br />
1.5 gram if patients weighs 66 – 90 kg<br />
2 gram if patient weighs > 90 kg<br />
Bactroban : ½ tube each nostril<br />
Vancomycin 1 gram<br />
Clindamycin<br />
600 mg if weight < 80 kg.<br />
900 mg if weight ≥ 80 kg.<br />
Clindamycin 900 mg<br />
if patient has a hx of staphlococcus aureus infection within<br />
the past 2 years<br />
Vancomycin (dosing scale below)<br />
1 gram if patient weighs < 80 kg<br />
1.5 gram if patients weighs ≥ 80 kg<br />
Clindamycin (dosing scale below) & gentamicin 80 mg<br />
600 mg if weight < 80 kg.<br />
900 mg if weight ≥ 80 kg.<br />
Ciprofloxacin 400 mg (urology only)<br />
Doxycycline 200 mg (urology only)<br />
Clindamycin (dosing scale below)<br />
600 mg if weight < 80 kg.<br />
900 mg if weight ≥ 80 kg.<br />
SBE Prophylaxis per AHA<br />
guidelines<br />
Ampicillin 1 gram<br />
Cefazolin 1 gram<br />
Vancomycin 1 gram<br />
Clindamycin (dosing scale below)<br />
600 mg if weight < 80 kg.<br />
900 mg if weight ≥ 80 kg.<br />
entereg <strong>pre</strong> op <strong>orders</strong><br />
Patient Criteria for Entereg (alvimopan) Use:<br />
By Checking the items 1 – 4 I confirm I have verified the following:<br />
❑ 1. Entereg (alvimopan) is indicated for partial or small bowel resection with primary anastomosis.<br />
❑ 2. Patient has not taken theraputic doses of opiods for more than seven (7) consecutive days immedatly prior to Entereg.<br />
❑ 3. Patient does not have hepatic dis<strong>orders</strong>.<br />
❑ 4. Patient does not have severe renal failure.<br />
Pre-Op: ❑ Entereg 12mg capsule orally NOW (must be given 30 minutes to 5 hours prior to surgery – give in <strong>pre</strong>-op)<br />
Post–Op: Follow “Entereg Fast Track” protocol on Post-Op Inpatient General Surgery Physician Orders.<br />
PHYSICIAN NAME PHYSICIAN SIGNATURE DATE TIME<br />
<strong>pre</strong>-<strong>operative</strong><br />
<strong>physiCian</strong> <strong>orders</strong><br />
PATIENT IDENTIFICATION LABEL<br />
3006779 (5/19/2011) PAGE 2 OF 3<br />
<strong>*PHYORD*</strong>
<strong>pre</strong>-<strong>operative</strong> <strong>physiCian</strong> <strong>orders</strong><br />
Name: _________________________________________ Time: _______________________ Date: _________________<br />
dvt prophyLaxis<br />
Heparin 5000 units (SQ) x 1 dose prior to surgery<br />
T.E.D. Hose _____ Bilateral _____ Right ______ Left<br />
SCDs ________________________________________<br />
Enoxaparin (Lovenox) 40 mg sq x1 ________________<br />
Other DVT Orders : _____________________________<br />
breast speCiaL needs<br />
sub-areola injection of nuclear isotope Tc 99m<br />
Sulfur Colloid per<br />
Nuclear Medicine Protocol<br />
______ Right ______Left _____Bilateral<br />
Needle placement with ultrasound/mammography<br />
_____ Right ______ Left _____ Bilateral<br />
Appointment time ________________<br />
ortho teCh – CerviCaL CoLLar / post-op shoe<br />
Miami J Collar (<strong>pre</strong>op to size)<br />
Post-Op Surgical Shoe: Size : ____________________<br />
protoCoL For parathyroideCtomy<br />
First PTH level drawn in Pre-Op<br />
Nuclear Medicine IV injection of Isotope,<br />
25 mCi Tc99m Sestamibi<br />
mri and Ct<br />
Placement of Fiducials in <strong>pre</strong>op per protocol ____________<br />
Right Frontal Temporal Parietal<br />
Left Frontal Temporal Parietal<br />
Posterior Fossa<br />
MRI with Stealth Protocol<br />
nuCLear mediCine “other” protoCoL<br />
Melanoma injection of nuclear isotope Tc99m<br />
Sulfur Colloid per Nuclear Medicine Protocol<br />
Melanoma site : _______________________________<br />
sLeep apnea protoCoL<br />
MRI of _______________________________________<br />
CT with Stealth Protocol<br />
CT Scan of ___________________________________<br />
additional <strong>orders</strong><br />
PHYSICIAN NAME PHYSICIAN SIGNATURE DATE<br />
<strong>pre</strong>-<strong>operative</strong><br />
<strong>physiCian</strong> <strong>orders</strong><br />
PATIENT IDENTIFICATION LABEL<br />
3006779 (5/19/2011) PAGE 3 OF 3<br />
<strong>*PHYORD*</strong>
anesthesia protoCoL<br />
*h&p on aLL patients within 30 days oF surgery*<br />
LoCaL & ConsCious sedation<br />
HEALTHY ASYMPTOMATIC PATIENTS<br />
No additional testing nescessary<br />
maC (monitored anesthesia care)<br />
< 50 years old No additional testing nescessary<br />
HEALTHY ASYMPTOMATIC PATIENTS<br />
> 50 years old Hgb EKG<br />
generaL & spinaL anesthetiC<br />
1) Low risK surgery with minimum bLood Loss (75 years old<br />
2) high risK surgery: iF patient matChes Criteria,<br />
assign FoLLowing Lab<br />
CBC<br />
No additional testing<br />
Hgb<br />
Hgb EKG<br />
Hgb EKG Creat<br />
Type & Screen / Cross Match x2 units<br />
■ Intra-abdominal, Intrathoracic, Vascular ■ Amputation, Major Bladder, Femur<br />
■ Lumbar, Thoracic or Cervical SPine ■ Knee or Hip other than replacement<br />
■ Knee, Ankle, or Hip Replacement<br />
■ Elbow, Shoulder<br />
■ Urologic other than major Bladder, Hernia<br />
■ C-section, Mastectomy, Breast Mass<br />
mediCaL history seCtion<br />
note: if patient<br />
has a medical<br />
history, consider<br />
lab from medical<br />
history section.<br />
Stable Coronary Artery Disease Hgb EKG<br />
Unstable Coronary Artery Disease Hgb EKG CXR<br />
Cardiac clearance within 3 months of surgery date<br />
Antiarrhythmic medication K+ EKG<br />
Digoxin K+ Creat EKG<br />
Diuretics K+<br />
Hypertension (HTN) Creat EKG<br />
Pulmonary Disease<br />
Smoker 1pk/day X 20 years<br />
EKG CXR<br />
PFT<br />
Only obtain if signs & symptoms suggest<br />
newer or pulmonary disease<br />
Diabetes glucose Creat EKG<br />
Renal Disease Hct/Hgb K+ Creat BUN<br />
Hepatic Disease pt/inr, ptt SGOT/ALK Phos<br />
Hepatitis Exposure pt/inr, ptt SGOT/ALK Phos<br />
Cerebral Vascular Accident (CVA) CBC EKG<br />
CNS Disease Creat EKG<br />
Anticoagulants CBC pt/inr, ptt<br />
Bleeding Disorder CBC pt/inr, ptt T&S or T&C<br />
Malignancy (chemotherapy) CBC pt/inr, ptt EKG CXR<br />
Radiation Therapy WBC EKG CXR<br />
Leukemia CBC pt/inr, ptt<br />
Steroids glucose Na+ K+<br />
Female of childbearing age<br />
<strong>pre</strong>gnancy test: urine or serum<br />
3006779 (5/19/2011)<br />
this page is not a permanent part oF the patient's Chart