

Special CME Issue - West Virginia State Medical Association
Special CME Issue - West Virginia State Medical Association
Special CME Issue - West Virginia State Medical Association

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
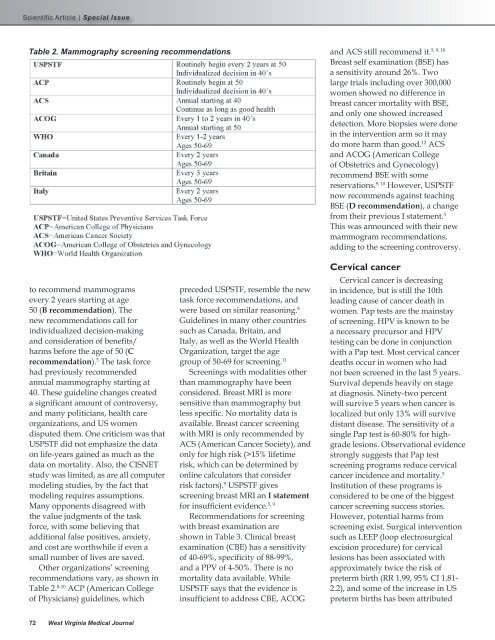
Table 2. Mammography screening recommendations<br />
5, 9, 10<br />
and ACS still recommend it.<br />
Breast self examination (BSE) has<br />
a sensitivity around 26%. Two<br />
large trials including over 300,000<br />
women showed no difference in<br />
breast cancer mortality with BSE,<br />
and only one showed increased<br />
detection. More biopsies were done<br />
in the intervention arm so it may<br />
do more harm than good. 12 ACS<br />
and ACOG (American College<br />
of Obstetrics and Gynecology)<br />
recommend BSE with some<br />
reservations. 9, 10 However, USPSTF<br />
now recommends against teaching<br />
BSE (D recommendation), a change<br />
from their previous I statement. 5<br />
This was announced with their new<br />
mammogram recommendations,<br />
adding to the screening controversy.<br />
to recommend mammograms<br />
every 2 years starting at age<br />
50 (B recommendation). The<br />
new recommendations call for<br />
individualized decision-making<br />
and consideration of benefits/<br />
harms before the age of 50 (C<br />
recommendation). 5 The task force<br />
had previously recommended<br />
annual mammography starting at<br />
40. These guideline changes created<br />
a significant amount of controversy,<br />
and many politicians, health care<br />
organizations, and US women<br />
disputed them. One criticism was that<br />
USPSTF did not emphasize the data<br />
on life-years gained as much as the<br />
data on mortality. Also, the CISNET<br />
study was limited, as are all computer<br />
modeling studies, by the fact that<br />
modeling requires assumptions.<br />
Many opponents disagreed with<br />
the value judgments of the task<br />
force, with some believing that<br />
additional false positives, anxiety,<br />
and cost are worthwhile if even a<br />
small number of lives are saved.<br />
Other organizations’ screening<br />
recommendations vary, as shown in<br />
Table 2. 8-10 ACP (American College<br />
of Physicians) guidelines, which<br />
preceded USPSTF, resemble the new<br />
task force recommendations, and<br />
were based on similar reasoning. 8<br />
Guidelines in many other countries<br />
such as Canada, Britain, and<br />
Italy, as well as the World Health<br />
Organization, target the age<br />
group of 50-69 for screening. 11<br />
Screenings with modalities other<br />
than mammography have been<br />
considered. Breast MRI is more<br />
sensitive than mammography but<br />
less specific. No mortality data is<br />
available. Breast cancer screening<br />
with MRI is only recommended by<br />
ACS (American Cancer Society), and<br />
only for high risk (>15% lifetime<br />
risk, which can be determined by<br />
online calculators that consider<br />
risk factors). 9 USPSTF gives<br />
screening breast MRI an I statement<br />
for insufficient evidence. 5, 9<br />
Recommendations for screening<br />
with breast examination are<br />
shown in Table 3. Clinical breast<br />
examination (CBE) has a sensitivity<br />
of 40-69%, specificity of 88-99%,<br />
and a PPV of 4-50%. There is no<br />
mortality data available. While<br />
USPSTF says that the evidence is<br />
insufficient to address CBE, ACOG<br />
Cervical cancer<br />
Cervical cancer is decreasing<br />
in incidence, but is still the 10th<br />
leading cause of cancer death in<br />
women. Pap tests are the mainstay<br />
of screening. HPV is known to be<br />
a necessary precursor and HPV<br />
testing can be done in conjunction<br />
with a Pap test. Most cervical cancer<br />
deaths occur in women who had<br />
not been screened in the last 5 years.<br />
Survival depends heavily on stage<br />
at diagnosis. Ninety-two percent<br />
will survive 5 years when cancer is<br />
localized but only 13% will survive<br />
distant disease. The sensitivity of a<br />
single Pap test is 60-80% for highgrade<br />
lesions. Observational evidence<br />
strongly suggests that Pap test<br />
screening programs reduce cervical<br />
cancer incidence and mortality. 5<br />
Institution of these programs is<br />
considered to be one of the biggest<br />
cancer screening success stories.<br />
However, potential harms from<br />
screening exist. Surgical intervention<br />
such as LEEP (loop electrosurgical<br />
excision procedure) for cervical<br />
lesions has been associated with<br />
approximately twice the risk of<br />
preterm birth (RR 1.99, 95% CI 1.81-<br />
2.2), and some of the increase in US<br />
preterm births has been attributed<br />
72 <strong>West</strong> <strong>Virginia</strong> <strong>Medical</strong> Journal












