

dhjBa
dhjBa
dhjBa

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
REVIEW<br />
Cover<br />
Focus<br />
Refractive Surgery<br />
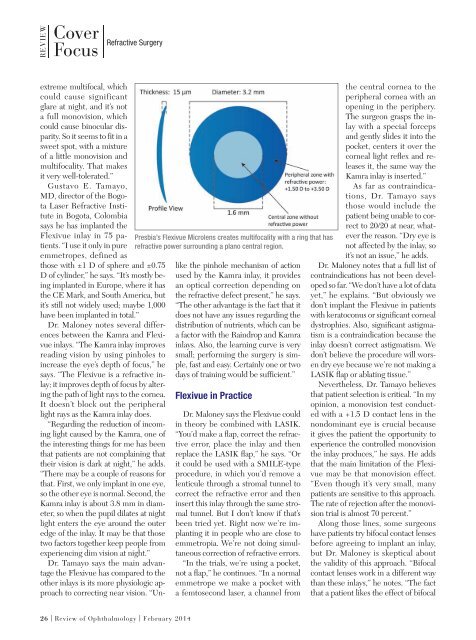
Presbia’s Flexivue Microlens creates multifocality with a ring that has<br />
refractive power surrounding a plano central region.<br />
extreme multifocal, which<br />
could cause significant<br />
glare at night, and it’s not<br />
a full monovision, which<br />
could cause binocular disparity.<br />
So it seems to fit in a<br />
sweet spot, with a mixture<br />
of a little monovision and<br />
multifocality. That makes<br />
it very well-tolerated.”<br />
Gustavo E. Tamayo,<br />
MD, director of the Bogota<br />
Laser Refractive Institute<br />
in Bogota, Colombia<br />
says he has implanted the<br />
Flexivue inlay in 75 patients.<br />
“I use it only in pure<br />
emmetropes, defined as<br />
those with ±1 D of sphere and ±0.75<br />
D of cylinder,” he says. “It’s mostly being<br />
implanted in Europe, where it has<br />
the CE Mark, and South America, but<br />
it’s still not widely used; maybe 1,000<br />
have been implanted in total.”<br />
Dr. Maloney notes several differences<br />
between the Kamra and Flexivue<br />
inlays. “The Kamra inlay improves<br />
reading vision by using pinholes to<br />
increase the eye’s depth of focus,” he<br />
says. “The Flexivue is a refractive inlay;<br />
it improves depth of focus by altering<br />
the path of light rays to the cornea.<br />
It doesn’t block out the peripheral<br />
light rays as the Kamra inlay does.<br />
“Regarding the reduction of incoming<br />
light caused by the Kamra, one of<br />
the interesting things for me has been<br />
that patients are not complaining that<br />
their vision is dark at night,” he adds.<br />
“There may be a couple of reasons for<br />
that. First, we only implant in one eye,<br />
so the other eye is normal. Second, the<br />
Kamra inlay is about 3.8 mm in diameter,<br />
so when the pupil dilates at night<br />
light enters the eye around the outer<br />
edge of the inlay. It may be that those<br />
two factors together keep people from<br />
experiencing dim vision at night.”<br />
Dr. Tamayo says the main advantage<br />
the Flexivue has compared to the<br />
other inlays is its more physiologic approach<br />
to correcting near vision. “Unlike<br />
the pinhole mechanism of action<br />
used by the Kamra inlay, it provides<br />
an optical correction depending on<br />
the refractive defect present,” he says.<br />
“The other advantage is the fact that it<br />
does not have any issues regarding the<br />
distribution of nutrients, which can be<br />
a factor with the Raindrop and Kamra<br />
inlays. Also, the learning curve is very<br />
small; performing the surgery is simple,<br />
fast and easy. Certainly one or two<br />
days of training would be sufficient.”<br />
Flexivue in Practice<br />
Dr. Maloney says the Flexivue could<br />
in theory be combined with LASIK.<br />
“You’d make a flap, correct the refractive<br />
error, place the inlay and then<br />
replace the LASIK flap,” he says. “Or<br />
it could be used with a SMILE-type<br />
procedure, in which you’d remove a<br />
lenticule through a stromal tunnel to<br />
correct the refractive error and then<br />
insert this inlay through the same stromal<br />
tunnel. But I don’t know if that’s<br />
been tried yet. Right now we’re implanting<br />
it in people who are close to<br />
emmetropia. We’re not doing simultaneous<br />
correction of refractive errors.<br />
“In the trials, we’re using a pocket,<br />
not a flap,” he continues. “In a normal<br />
emmetrope we make a pocket with<br />
a femtosecond laser, a channel from<br />
the central cornea to the<br />
peripheral cornea with an<br />
opening in the periphery.<br />
The surgeon grasps the inlay<br />
with a special forceps<br />
and gently slides it into the<br />
pocket, centers it over the<br />
corneal light reflex and releases<br />
it, the same way the<br />
Kamra inlay is inserted.”<br />
As far as contraindications,<br />
Dr. Tamayo says<br />
those would include the<br />
patient being unable to correct<br />
to 20/20 at near, whatever<br />
the reason. “Dry eye is<br />
not affected by the inlay, so<br />
it’s not an issue,” he adds.<br />
Dr. Maloney notes that a full list of<br />
contraindications has not been developed<br />
so far. “We don’t have a lot of data<br />
yet,” he explains. “But obviously we<br />
don’t implant the Flexivue in patients<br />
with keratoconus or significant corneal<br />
dystrophies. Also, significant astigmatism<br />
is a contraindication because the<br />
inlay doesn’t correct astigmatism. We<br />
don’t believe the procedure will worsen<br />
dry eye because we’re not making a<br />
LASIK flap or ablating tissue.”<br />
Nevertheless, Dr. Tamayo believes<br />
that patient selection is critical. “In my<br />
opinion, a monovision test conducted<br />
with a +1.5 D contact lens in the<br />
nondominant eye is crucial because<br />
it gives the patient the opportunity to<br />
experience the controlled monovision<br />
the inlay produces,” he says. He adds<br />
that the main limitation of the Flexivue<br />
may be that monovision effect.<br />
“Even though it’s very small, many<br />
patients are sensitive to this approach.<br />
The rate of rejection after the monovision<br />
trial is almost 70 percent.”<br />
Along those lines, some surgeons<br />
have patients try bifocal contact lenses<br />
before agreeing to implant an inlay,<br />
but Dr. Maloney is skeptical about<br />
the validity of this approach. “Bifocal<br />
contact lenses work in a different way<br />
than these inlays,” he notes. “The fact<br />
that a patient likes the effect of bifocal<br />
26 | Review of Ophthalmology | February 2014