Targeting Aged Care to People who are Financially or Socially ...
Targeting Aged Care to People who are Financially or Socially ...
Targeting Aged Care to People who are Financially or Socially ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>Targeting</strong> <strong>Aged</strong> <strong>C<strong>are</strong></strong> <strong>to</strong> <strong>People</strong> <strong>who</strong> <strong>are</strong><br />
<strong>Financially</strong> <strong>or</strong> <strong>Socially</strong> Disadvantaged:<br />
Policy Evaluation Study About The Social<br />
Gradient in Health of Older South<br />
Australians.<br />
Brian Fleming 1<br />
Department of Health, South Australia<br />
1 Introduction<br />
There is considerable research interest in inequalities in health, <strong>or</strong> inequities in health, <strong>or</strong>,<br />
as I prefer, the social gradient in health. Much of the published research is descriptive<br />
and there is interest in moving <strong>to</strong> policy approaches <strong>to</strong> the issue and <strong>to</strong> its attenuation.<br />
This study lies at the beginning of that path as it examines existing health services<br />
funding policy by asking how a particular policy might be different if evaluated from the<br />
perspective of a social gradient in health. Health services’ funding occupies the great<br />
bulk of the eff<strong>or</strong>t and attention of the Department of Health and <strong>Aged</strong> <strong>C<strong>are</strong></strong> in Australia.<br />
A change in health services’ policy is ‘after the event’ of health differences, and theref<strong>or</strong>e<br />
does not contribute <strong>to</strong> the attenuation of the social gradient in health. However, this<br />
policy evaluation study is a contribution <strong>to</strong> a m<strong>or</strong>e general advancement of social-gradient<br />
policy f<strong>or</strong>mulation.<br />
2 Background<br />
Responsibility f<strong>or</strong> aged c<strong>are</strong> in Australia is sh<strong>are</strong>d between national and state jurisdictions<br />
in a federal system. The Commonwealth has responsibility f<strong>or</strong> aged c<strong>are</strong> services and the<br />
supply of these places is regulated by a population-based f<strong>or</strong>mula. <strong>Aged</strong> c<strong>are</strong> services, f<strong>or</strong><br />
this paper, include high c<strong>are</strong> (f<strong>or</strong>merly nursing home c<strong>are</strong>) low c<strong>are</strong> (f<strong>or</strong>merly hostel c<strong>are</strong>)<br />
and community aged c<strong>are</strong> packages (<strong>who</strong>se <strong>or</strong>igins <strong>are</strong> as a home-based substitute f<strong>or</strong><br />
N =<br />
I would like <strong>to</strong> acknowledge the helpful comments of Dr. Neville Hicks on an earlier<br />
draft and my employees assistance with study through Mr David Kemp.<br />
Fleming, B. (2002), ‘<strong>Targeting</strong> aged c<strong>are</strong> <strong>to</strong> people <strong>who</strong> <strong>are</strong> financially <strong>or</strong> socially disadvantaged: policy<br />
evaluation study about the social gradient of health of older South Australians’, T. Eardley and B.<br />
Bradbury, eds, Competing Visions: Refereed Proceedings of the National Social Policy Conference 2001,<br />
SPRC Rep<strong>or</strong>t 1/02, Social Policy Research Centre, University of New South Wales, Sydney, 155-179.
BRIAN FLEMING<br />
hostel c<strong>are</strong>) 2 . The current f<strong>or</strong>mula f<strong>or</strong> the supply of Commonwealth aged c<strong>are</strong> services,<br />
<strong>or</strong> ‘places’, at one hundred per thousand persons age 70 years <strong>or</strong> m<strong>or</strong>e, (100/1,000 70+)<br />
was established in 1986 by the Nursing Homes and Hostels Review (Commonwealth of<br />
Australia 1986: 129).<br />
The reasoning f<strong>or</strong> selecting 100/1000 70+ was that this ratio would maintain the then<br />
existing average national supply while delivering ‘equity’ over time between the states<br />
and terri<strong>to</strong>ries (Commonwealth of Australia, 1986). 3 Since that time the ratio has also<br />
been used <strong>to</strong> deliver population-based parity of services within states, down <strong>to</strong> <strong>are</strong>as<br />
defined as Statistical Local Areas (SLAs), which c<strong>or</strong>responded closely <strong>to</strong> local<br />
government boundaries, particularly in South Australia, until about 1998. 4 So, while it<br />
was not created as an indica<strong>to</strong>r of ‘need’, the then existing national average ratio was<br />
adopted, and has been used since, as a benchmark f<strong>or</strong> planning and providing additional<br />
services <strong>to</strong> SLA level. The department routinely obtains population projections by SLA<br />
from the Australian Bureau of Statistics (ABS), computes the benchmark, and uses the<br />
results <strong>to</strong> inf<strong>or</strong>m decisions about both the overall supply and distribution of additional<br />
services. There is a growing population over 70. The department controls the distribution<br />
of aged c<strong>are</strong> places by advertising <strong>are</strong>as of under-supply, inf<strong>or</strong>med by the benchmark, and<br />
selecting providers of c<strong>are</strong> from applicants f<strong>or</strong> funding.<br />
This study is not about the <strong>to</strong>tal national supply of places, which is decided by the<br />
Minister f<strong>or</strong> <strong>Aged</strong> <strong>C<strong>are</strong></strong>, inf<strong>or</strong>med in part by the ratio. Instead, this study is about the<br />
distribution of those places, particularly the intra-state distribution effects.<br />
There <strong>are</strong> three main distributional issues with the benchmark f<strong>or</strong>mula. First, it requires<br />
an overlay <strong>to</strong> consider access; SLAs have large variation in geographic <strong>are</strong>a, with some<br />
large sized rural SLAs having relatively small 70+ populations. So the distribution of<br />
services within an SLA becomes imp<strong>or</strong>tant. Secondly, the f<strong>or</strong>mula distributes services <strong>to</strong><br />
SLAs in a way that is affected by spatial settlement patterns. Some SLAs, settled at<br />
particular times, have a coh<strong>or</strong>t effect where a relatively large prop<strong>or</strong>tion can reach the<br />
planning age <strong>to</strong>gether. This paper is about a third issue: the f<strong>or</strong>mula delivers<br />
prop<strong>or</strong>tionately m<strong>or</strong>e services <strong>to</strong> SLAs that have longer lived populations. An argument is<br />
2 The maj<strong>or</strong>ity of data presented is f<strong>or</strong> residential aged c<strong>are</strong>, which includes high c<strong>are</strong> and low c<strong>are</strong>.<br />
3 See page 42 of the Nursing Homes and Hostels Review 1985. A comparison with international<br />
supply at the time showed that Australia’s <strong>to</strong>tal was similar <strong>to</strong> 11 other ‘high provision’ countries but<br />
m<strong>or</strong>e heavily <strong>or</strong>iented <strong>to</strong> nursing c<strong>are</strong> places. Another aim of the review was theref<strong>or</strong>e <strong>to</strong> shift the<br />
balance between nursing home c<strong>are</strong> and hostel c<strong>are</strong>, so the f<strong>or</strong>mula of 100/1000 70+ was divided<br />
in<strong>to</strong> 40 nursing home and 60 hostel c<strong>are</strong> places, and later, 40 high c<strong>are</strong>, 50 low c<strong>are</strong> and 10<br />
community aged c<strong>are</strong> packages<br />
4 There was a concerted eff<strong>or</strong>t <strong>to</strong> amalgamate local governments, which resulted in boundary changes.<br />
156
TARGETING AGED CARE TO PEOPLE WHO ARE DISADVANTAGED<br />
made f<strong>or</strong> a distributive method based on life expectancy, so it is relevant <strong>to</strong> examine some<br />
features of life expectancy calculations.<br />
3 Life Expectancy<br />
Life expectancy is calculated from life tables using current age-specific death rates, that<br />
is, using the current rate of deaths per population between exact age ‘x’ and exact age<br />
‘x+1’. 5 Life expectancy, at age ‘x’ can be regarded as the probable mean length of<br />
additional life beyond age ‘x’ of all the people alive at age ‘x’ if they had the overall<br />
population experience. Life tables <strong>are</strong> produced based on a hypothetical starting<br />
population of 100 000 persons at exact age zero, with Australian tables ceasing at age<br />
99years. 6 Males and females experience markedly different death rates, so life tables <strong>are</strong><br />
produced separately by sex. Deaths in each year reduce the population at the next age, and<br />
if plotted, produce a curve of ‘survival’. Life tables <strong>are</strong> useful f<strong>or</strong> comparing one<br />
population’s experience with another’s as they standardise f<strong>or</strong> different age structures.<br />
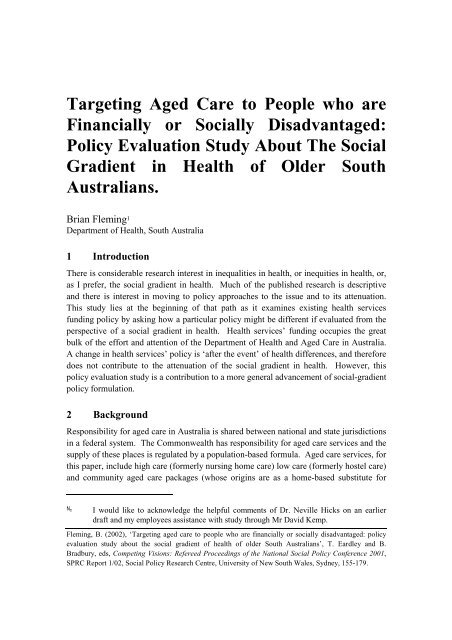
A visual example of the 1998 South Australian lifetable appears at Figure 1. It has a curve<br />
typical of developed countries, with high survival until older ages. Males have death rates<br />
higher than females from birth and this affects their surviving population, so that the male<br />
survival curve is below that of the female.<br />
In Figure 2, the same 1998 life-table inf<strong>or</strong>mation is presented as deaths by single age,<br />
rather than surviv<strong>or</strong>s, f<strong>or</strong> these representative 100 000 populations. Here it can be seen<br />
that, comp<strong>are</strong>d with female deaths, male infant deaths <strong>are</strong> higher, there is a rise in male<br />
deaths in late teens, and deaths in older age begin <strong>to</strong> rise earlier f<strong>or</strong> males. These<br />
circumstances combine <strong>to</strong> give males a five-year reduction in the mean expectation of life<br />
at birth comp<strong>are</strong>d <strong>to</strong> females. A f<strong>or</strong>mula that delivers m<strong>or</strong>e services <strong>to</strong> an increasingly<br />
aged population size, as the current benchmark approach does, is a valuable and<br />
accountable feature of the aged c<strong>are</strong> program. Use of health services, however, is much<br />
m<strong>or</strong>e closely related <strong>to</strong> time until death than time from birth (Fuchs 1984; van Weel and<br />
Michels, 1997; Himsw<strong>or</strong>th and Goldacre, 1999). One estimate is that health service<br />
expenditure in the last year of life is 6.6 times (in the next <strong>to</strong> last year, 2.3 times) as large<br />
as f<strong>or</strong> those <strong>who</strong> survived at least two years (Fuchs, 1984). So aged c<strong>are</strong> services may be<br />
better targeted if based on years from death than years from birth, as is now the case.<br />
5 Note this is the ‘current’ life table method. An alternative is the coh<strong>or</strong>t life table method,<br />
where the death rate experience of birth coh<strong>or</strong>ts is used, see f<strong>or</strong> example Armitage and<br />
Berry, 1994: 470. Current life tables can also be produced f<strong>or</strong> age groups and these <strong>are</strong><br />
referred <strong>to</strong> as abridged life tables. Life tables in this paper were produced by the Australian<br />
Bureau of Statistics.<br />
6 There <strong>are</strong> smoothing f<strong>or</strong>mulae applied in official tables <strong>to</strong> adjust f<strong>or</strong> annual fluctuations. In<br />
Australia that has meant using three years of data <strong>to</strong> produce life tables f<strong>or</strong> the middle year.<br />
157
BRIAN FLEMING<br />
Figure 1: Lifetable Survival Curves, South Australia, Male and Female<br />
100000<br />
90000<br />
80000<br />
70000<br />
60000<br />
50000<br />
40000<br />
30000<br />
20000<br />
10000<br />
Surviv<strong>or</strong>s<br />
females<br />
males<br />
0<br />
0 5 10 15 20 25 30 35 40 45 50 55 60 65 70 75 80 85 90 95 10<br />
0<br />
Age<br />
10<br />
5<br />
11<br />
0<br />
Source: ABS, 1999, Ca<strong>to</strong>logue No. 3311.4<br />
Figure 2: Lifetable Deaths Curves, South Australia, Male and Female<br />
6000<br />
5000<br />
4000<br />
3000<br />
Deaths<br />
females<br />
males<br />
2000<br />
1000<br />
0<br />
1 6 11 16 21 26 31 36 41 46 51 56 61 66 71 76 81 86 91 96 10<br />
1<br />
Age<br />
10<br />
6<br />
11<br />
1<br />
Source: ABS, 1999, Catalogue No. 3311.4<br />
An approach based on years from death, <strong>or</strong> life expectancy, is supp<strong>or</strong>ted by evidence that<br />
the expected length of stay in residential aged c<strong>are</strong>, in Australia, varies very little<br />
comp<strong>are</strong>d with age at entry, see Table 1, (Australian Institute of Health and Welf<strong>are</strong>,<br />
1999). Years <strong>to</strong> death is relatively constant at about one year f<strong>or</strong> males and two years f<strong>or</strong><br />
158
TARGETING AGED CARE TO PEOPLE WHO ARE DISADVANTAGED<br />
females. If anything, the trend is that the younger the age at entry the sh<strong>or</strong>ter the length of<br />
stay, contrary <strong>to</strong> what might be expected. 7<br />
Table 1: Expected Length of Stay in Residential <strong>C<strong>are</strong></strong> by Age, Comp<strong>are</strong>d with Life<br />
Expectancy at that Age<br />
Age ‘x’<br />
Life expectancy at<br />
age ‘x’<br />
Expected length of stay<br />
(years) at age ‘x’<br />
Males 65 16.1 0.7<br />
80 7.2 0.9<br />
90 4.0 1.1<br />
Females 65 19.8 1.9<br />
80 9.0 2.2<br />
90 4.6 2.1<br />
Source: AIHW Australia’s Welf<strong>are</strong> 1999, Chapter 6; Gibson 1996.<br />
Life Expectancy and Residential <strong>Aged</strong> <strong>C<strong>are</strong></strong><br />
In this section I establish that inf<strong>or</strong>mation about the lifetable model of deaths offers a<br />
reliable surrogate indica<strong>to</strong>r f<strong>or</strong> the pattern, by age, of entry <strong>to</strong> residential aged c<strong>are</strong>.<br />
The aim was <strong>to</strong> gain an understanding of relationships, between life expectancy and<br />
residential c<strong>are</strong> use. I obtained data from the Department of Health and <strong>Aged</strong> <strong>C<strong>are</strong></strong> on the<br />
current age, of all persons in residential aged c<strong>are</strong> in South Australia, at 30 June 2000.<br />
The age distribution of actual use of residential aged c<strong>are</strong> in South Australia in June 2000<br />
is shown in Figure 3 and Figure 4. Note that few people aged 70 years, the ‘planning age’,<br />
use residential aged c<strong>are</strong>. The median age at entry <strong>to</strong> residential c<strong>are</strong> in South Australia is<br />
about 82 years, so using the population 70+ includes the maj<strong>or</strong>ity of people <strong>who</strong> use aged<br />
c<strong>are</strong> but the planning age itself is not a representative descrip<strong>to</strong>r of the population using<br />
aged c<strong>are</strong>, in a statistical sense. This has led <strong>to</strong> suggestions that raising the planning age <strong>to</strong><br />
80+ years would make m<strong>or</strong>e sense, as this would be closer <strong>to</strong> the median age at entry and<br />
an age m<strong>or</strong>e representative of the pattern of use – this idea is criticised later in the paper.<br />
The lifetable deaths f<strong>or</strong> South Australia, <strong>are</strong> the product of rising age-specific death rates<br />
by age and a diminishing population by age. Similarly the population in aged c<strong>are</strong> is a<br />
product of rising age-specific risk of admission and a diminishing population by age. It is<br />
likely that these <strong>are</strong> related as life expectancy in aged c<strong>are</strong> is limited, see Table 1, and<br />
most separations <strong>are</strong> due <strong>to</strong> death. Data on residents in aged c<strong>are</strong> services were overlayed<br />
with deaths data, and <strong>are</strong> discussed separately by sex.<br />
F<strong>or</strong> females the data were f<strong>or</strong> current residents. Acc<strong>or</strong>ding <strong>to</strong> Gibson, (see Table 1 1996,<br />
5), female length of stay is about two years, independent of age. So, assuming an average<br />
of one year in c<strong>are</strong> f<strong>or</strong> current female residents the deaths data were translated f<strong>or</strong>ward<br />
7 While most departures will be due <strong>to</strong> death, this may be affected by transfers.<br />
159
BRIAN FLEMING<br />
one year so that the number of deaths relates <strong>to</strong> the age less one year. This puts the<br />
‘deaths in two years’ data roughly in line with the resident data at entry <strong>to</strong> aged c<strong>are</strong>, f<strong>or</strong><br />
females. This results in Figure 4. The data <strong>are</strong> a very good visual match. Linear regresion<br />
also confirms a very strong relationship: r-squ<strong>are</strong>d = 0.9623p
TARGETING AGED CARE TO PEOPLE WHO ARE DISADVANTAGED<br />
In <strong>or</strong>der <strong>to</strong> comp<strong>are</strong> a years-from-death approach, with the current planning approach, the<br />
South Australian lifetable was used <strong>to</strong> describe the pattern of surviv<strong>or</strong>s at aged 70 <strong>or</strong><br />
m<strong>or</strong>e. Given that the lifetable is based on current age-specific death rates, the shape of<br />
this curve reflects the South Australian experience of survival at these ages; the actual<br />
numbers <strong>are</strong> not relevant at this stage. It can be seen from Figure 5 that the current<br />
method of counting the population aged 70 years <strong>or</strong> m<strong>or</strong>e is a po<strong>or</strong>er fit than deaths data,<br />
r-squ<strong>are</strong>d = 0.3158, p70 1997-9 (schema life table)<br />
and 2.residents (high and low c<strong>are</strong>) 30 Jun 1999 (n=9612)<br />
600<br />
500<br />
400<br />
300<br />
200<br />
100<br />
0<br />
0 5 10 15 20 25 30 35 40 45 50 55 60 65 70 75 80 85 90 95 10<br />
0<br />
10<br />
5<br />
11<br />
0<br />
100000<br />
90000<br />
80000<br />
70000<br />
60000<br />
50000<br />
40000<br />
30000<br />
20000<br />
10000<br />
0<br />
residents<br />
surviv<strong>or</strong>s<br />
Source: ABS (1999) Catalogue No. 3311.4<br />
The exercise was repeated f<strong>or</strong> data on males in residential c<strong>are</strong> in South Australia,<br />
without shifting the deaths data by one year. This is because the average length of stay is<br />
only one year f<strong>or</strong> males and the current age will already be roughly six months older than<br />
age at entry (see Figure 6). The 70+ figure f<strong>or</strong> males is similar <strong>to</strong> that of females but is not<br />
shown; r-squ<strong>are</strong>d f<strong>or</strong> deaths is 0.9285 p
BRIAN FLEMING<br />
In Australia, and South Australia, a series of social atlases illustrate a variation of health<br />
outcome by <strong>are</strong>a, along with the spatial distribution of material and other resources, in<br />
line with the expected pattern –the higher the material indica<strong>to</strong>rs the better the health<br />
indica<strong>to</strong>rs, including m<strong>or</strong>tality (Glover, Shand et al,. 1996; Glover and Tennant, 1999a<br />
and 1999b).<br />
Figure 6 The Distribution of Males in Residential <strong>Aged</strong> <strong>C<strong>are</strong></strong> in South Australia by<br />
Age, June 2000, and Deaths from South Australian Lifetable.<br />
SA males by single age on two axes: 1. residents (high and low c<strong>are</strong>) 30 Jun<br />
2000 (n=3380) and 2. Deaths 1997-9 (life table n=100,000)<br />
200<br />
180<br />
160<br />
140<br />
120<br />
100<br />
80<br />
60<br />
40<br />
20<br />
0<br />
0 5 10 15 20 25 30 35 40 45 50 55 60 65 70 75 80 85 90 95 10<br />
0<br />
10<br />
5<br />
5900<br />
4900<br />
3900<br />
2900<br />
1900<br />
900<br />
-100<br />
male residents<br />
male deaths<br />
If one <strong>are</strong>a has lower life expectancy than another then its population will experience the<br />
last two years of life at a lower age; the surviv<strong>or</strong>s at a given age will be fewer. So a<br />
funding f<strong>or</strong>mula based on a particular age, say 70 years, will deliver greater resources <strong>to</strong><br />
<strong>are</strong>as that have a higher survival, other things, such as age structure, being equal.<br />
F<strong>or</strong> example, take two <strong>are</strong>as A and B with about a five-and-a-half year difference in life<br />
expectancy; 81.5 and 75.9 years respectively. 8 Typical survival curves f<strong>or</strong> the two <strong>are</strong>as<br />
<strong>are</strong> shown at Figure 7. If the populations required c<strong>are</strong> in the last two years of life, then on<br />
average, population A would need c<strong>are</strong> from 79.5 <strong>to</strong> 81.5 years and population B 74 <strong>to</strong> 76<br />
years, with similar numbers of people requiring c<strong>are</strong>. The population aged between 81<br />
and 82 in Area A would be 62285 and between 79 and 80 in <strong>are</strong>a B 62545. However,<br />
under the present benchmark f<strong>or</strong>mula of 100/1000 70+, the difference in the suviving<br />
population at age seventy is 85238 – 74697 = 10541. Under the benchmark f<strong>or</strong>mula f<strong>or</strong><br />
aged c<strong>are</strong> the Commonwealth would supply 8524 places in <strong>are</strong>a A comp<strong>are</strong>d <strong>to</strong> 7470 in<br />
<strong>are</strong>a B, a difference of 1054 places.<br />
8 This is about the size of the expected difference between the longest and sh<strong>or</strong>test lived regions.<br />
162
TARGETING AGED CARE TO PEOPLE WHO ARE DISADVANTAGED<br />
Figure 7: Survival Curves f<strong>or</strong> Two Populations Whose Life Expectancy is about 5<br />
Years Different<br />
Number surviving at<br />
age x 100000<br />
90000<br />
80000<br />
70000<br />
60000<br />
50000<br />
40000<br />
30000<br />
20000<br />
10000<br />
0<br />
Life Table survival curves<br />
Life expectancy<br />
at birth = 75.9<br />
Surviv<strong>or</strong>s at<br />
age = 70.0<br />
Life expectancy<br />
at birth = 81.5<br />
x<br />
Source ABS 3302.0<br />
There <strong>are</strong> 11 South Australian planning regions, four metropolitan and seven nonmetropolitan,<br />
used by the Commonwealth Department of Health and <strong>Aged</strong> <strong>C<strong>are</strong></strong>. The four<br />
metropolitan regions <strong>are</strong>, conveniently, N<strong>or</strong>th, South, East, and West. The consistent<br />
overall pattern is that the East region experiences the best health and socioeconomic<br />
circumstances, with the N<strong>or</strong>th the po<strong>or</strong>est, and West and South in between (Glover and<br />
Woollacott, 1992). Life expectancy is theref<strong>or</strong>e expected <strong>to</strong> reflect these general patterns.<br />
However, regional and SLA life tables <strong>are</strong> not currently produced nationally. An<br />
indication of what regional and SLA tables might reveal is given by some research in<br />
Vic<strong>to</strong>ria; a page extracted from the publication is at Figure 8. (Vic<strong>to</strong>ria, 1999, Burden of<br />
Disease Study, http://www.dhs.vic.gov.au/phb/9903009/index) This shows the expected<br />
regional variation in life expectancy, in this case f<strong>or</strong> males by local government <strong>are</strong>a. It<br />
also shows a clustering of LGAs that <strong>are</strong> below, equal <strong>to</strong> <strong>or</strong> above the State averages,<br />
particularly in the metropolitan <strong>are</strong>a.<br />
In the following pages I propose a method <strong>to</strong> distribute aged c<strong>are</strong> resources using<br />
inf<strong>or</strong>mation about the spatial distribution of life expectancy and show how it would<br />
comp<strong>are</strong> <strong>to</strong> the distribution based on the benchmark 100/1000 70+. In <strong>or</strong>der <strong>to</strong><br />
demonstrate how a method based on deaths inf<strong>or</strong>mation might w<strong>or</strong>k, I have used median<br />
age at death by SLA as a proxy measure f<strong>or</strong> life expectancy. 9 The median age at death is<br />
similar <strong>to</strong> life expectancy at birth, in most jurisdictions of Australia, but does not adjust<br />
9 The ‘median age’ statistic does not standardise f<strong>or</strong> the population structure, as life expectancy does,<br />
and so will deliver a younger age where there is a younger age structure.<br />
163
BRIAN FLEMING<br />
Figure 8: Extract of Australian Example of Life Expectancy by Local Area<br />
Source:Vic<strong>to</strong>ria, (1999) Burden of Disease<br />
f<strong>or</strong> age structure see Table 2 F<strong>or</strong> example, younger age structures in the N<strong>or</strong>thern<br />
Terri<strong>to</strong>ry and the ACT affect the size of the difference between life expectancy and<br />
median age at death. 10 ABS supplied data on the average annual number of female<br />
deaths, male deaths, male, female and person median age at death by SLA f<strong>or</strong> the years<br />
1997-99. 11 A wider range of years was not readily obtainable due <strong>to</strong> boundary changes.<br />
Aggregates of those SLAs, however, were in current use in aged c<strong>are</strong> planning aged c<strong>are</strong><br />
through 1999.<br />
10 The N<strong>or</strong>thern Terri<strong>to</strong>ry has a younger population and a relatively large indigenous population, which<br />
has high standardised- m<strong>or</strong>tality (2.2 f<strong>or</strong> males and 1.5 females in 1997-98). The Australian Capital<br />
Terri<strong>to</strong>ry, the home of the national government, has a healthy, educated and young w<strong>or</strong>ker inmigration<br />
effect.<br />
11 SLAs were based on 1996 profiles.<br />
164
TARGETING AGED CARE TO PEOPLE WHO ARE DISADVANTAGED<br />
Table 2 Comp<strong>are</strong> median age at death with expectation of life at birth, Australian<br />
jurisdictions.<br />
Median age death e 0 0 96/8 delta (LE-median)<br />
Males Females Male Female Male Female<br />
NSW 74.4 81 75.8 81.6 1.4 0.6<br />
Vic 74.8 81.6 76.3 81.7 1.5 0.1<br />
Qld 73.7 80.3 75.6 81.5 1.9 1.2<br />
SA 75.3 81.7 76 81.6 0.7 -0.1<br />
WA 73.6 80.8 76.1 81.9 2.5 1.1<br />
Tas 75.1 80.5 75.1 80.4 0.0 -0.1<br />
NT 53.7 57.7 70.6 75 16.9 17.3<br />
ACT 72.6 78.8 77.5 81.6 4.9 2.8<br />
Aust 74.3 81 75.9 81.5 1.6 0.5<br />
Source: ABS, (1998:12) Table 1.1, 12 Catalogue No. 3302.0<br />
Only SLAs with m<strong>or</strong>e than an average of 5 female deaths per year were used in the<br />
subsequent analysis. 12 A scatter plot of median age at death by SLA appears at Figure 9.<br />
Figure 9: Median Age at Death, Males, Females and Persons (ranked), by SLA<br />
Median age at death, males, females, persons(ranked), by SLA deaths(f)>4<br />
90.0<br />
85.0<br />
80.0<br />
75.0<br />
70.0<br />
65.0<br />
60.0<br />
55.0<br />
50.0<br />
45.0<br />
40.0<br />
Persons<br />
Males<br />
Females<br />
In Table 3, I have set out some basic features of the data. When separated in<strong>to</strong> the<br />
planning regions used by the Commonwealth, the metropolitan regions show the expected<br />
relationship; the East has the highest group of median ages and the n<strong>or</strong>th the lowest, see<br />
Figure 10.<br />
12 The decision <strong>to</strong> use five deaths was based on discussion with ABS. Five female deaths was chosen as<br />
the population in aged c<strong>are</strong> is mainly female and it is a m<strong>or</strong>e conservative approach as male deaths<br />
usually exceed female deaths.<br />
165
BRIAN FLEMING<br />
Table 3: Median Age at Death Data by SLA - Selected Features<br />
SLA<br />
Avg.<br />
annual<br />
male<br />
deaths<br />
Avg.<br />
annual<br />
female<br />
deaths<br />
Median<br />
age death<br />
male<br />
Median<br />
age death<br />
female<br />
Median<br />
age death<br />
persons<br />
Lowest median age<br />
at death persons 18 5.5 40.2 52.5 56.6<br />
Highest median<br />
age at death<br />
persons 6 8 80.0 86.0 85.3<br />
With most (male<br />
and) female deaths 478.5 404.5 76.5 80.8 78.5<br />
With largest<br />
population<br />
(111 910) 287 226.5 70.0 76.8 72.9<br />
Figure 10: Median Age at Death, Persons, and Metropolitan Areas South Australia<br />
(SLAs) Grouped in<strong>to</strong> Commonwealth Planning Regions<br />
Median age at death, deaths 1997-98, SLAs grouped in<strong>to</strong> four urban planning regions, m<strong>or</strong>e than 5 female<br />
deaths.<br />
86.0<br />
84.0<br />
82.0<br />
80.0<br />
78.0<br />
76.0<br />
74.0<br />
72.0<br />
70.0<br />
Gawler<br />
T T Gully<br />
Salisbury<br />
Elizabeth<br />
Munno<br />
P<br />
N<strong>or</strong>th<br />
Glenelg Mitcham<br />
Brigh<strong>to</strong>n<br />
Onkaparing<br />
Marion<br />
Noarlunga<br />
Happy<br />
V ll<br />
Willunga<br />
South<br />
West<br />
THenley&Grang<br />
Hindmarsh&Woodvill<br />
P<strong>or</strong>t<br />
Ad l id<br />
Thebar<strong>to</strong><br />
EnfieldB<br />
West<br />
Kensing<strong>to</strong>n<br />
St Peters<br />
Walkervill<br />
Unley<br />
Payneha<br />
Adelaide<br />
Burnside<br />
East<br />
Prospect<br />
Cambell<strong>to</strong>w<br />
Enfield<br />
Stirling<br />
East T<strong>or</strong>rens<br />
Source: ABS (1999), Catalogue No. 3302.0<br />
The non-metropolitan data is displayed at Figure 11.<br />
166
TARGETING AGED CARE TO PEOPLE WHO ARE DISADVANTAGED<br />
Figure 11: Median Age at Death, Persons, Non-metropolitan Areas South Australia<br />
(SLAs) Grouped in<strong>to</strong> Commonwealth Planning Regions<br />
90.0<br />
Median age at death, deaths 1997-98, SLAs grouped in<strong>to</strong> seven non- urban<br />
regions, m<strong>or</strong>e than 5 female deaths. Source ABS<br />
85.0<br />
80.0<br />
75.0<br />
70.0<br />
Qu<strong>or</strong>n<br />
72.5<br />
70.5<br />
Cleve<br />
80.9<br />
Lox<strong>to</strong>n 79.0<br />
76.8 77.1<br />
76.3<br />
76.8 76.9 77.5 78.1<br />
Berri<br />
Tatiara<br />
78.3<br />
77.5<br />
76.8<br />
74.5<br />
Mt Gambier<br />
Tanunda<br />
82.9<br />
80.8 81.1 81.3<br />
81.4 81.9<br />
78.2 78.4 78.7 79.1 79.5<br />
75.4<br />
71.8 72.1<br />
70.0<br />
Mallala<br />
Pinnaroo<br />
80.9<br />
80.1<br />
78.3 78.9<br />
77.3<br />
76.2 76.3 76.4<br />
74.4 75.0<br />
Yankalilla<br />
Orr<strong>or</strong>oo<br />
79.5<br />
80.0<br />
78.0<br />
76.6 76.1<br />
Pt Brough<strong>to</strong>n<br />
65.0<br />
Ceduna<br />
60.0<br />
55.0<br />
Uninc far n<strong>or</strong>th<br />
Whyalla &<br />
Far N<strong>or</strong>th Riverland Eyre South Y<strong>or</strong>ke &<br />
Hills<br />
East<br />
Barossa Mallee<br />
Mid N<strong>or</strong>th<br />
Source: ABS (1999), Catalogue No. 3302.0<br />
In <strong>or</strong>der <strong>to</strong> arrive at a representative median age at death by region the medians were<br />
treated as means and population-weighted <strong>to</strong> arrive at the ‘medians’ in Table 4. I am well<br />
aw<strong>are</strong> of the arithmetical leap here but, while it would be a relatively straightf<strong>or</strong>ward<br />
exercise f<strong>or</strong> the ABS <strong>to</strong> make the calculations based on the <strong>or</strong>iginal deaths data, it is<br />
expensive f<strong>or</strong> an individual <strong>to</strong> obtain this data, and not warranted as the exercise is<br />
illustrative. The result is consistent with other spatial inf<strong>or</strong>mation and indicates clearly a<br />
range of median age at death, by locality, f<strong>or</strong> both Adelaide and the rest of South<br />
Australia.<br />
The analysis of deaths data and residents by age suggests that one possibility would be <strong>to</strong><br />
count the numbers of deaths and use the subsequent prop<strong>or</strong>tions by <strong>are</strong>a <strong>to</strong> distribute aged<br />
c<strong>are</strong>. Note that the very strong c<strong>or</strong>relation, between deaths data and resident data, is f<strong>or</strong><br />
these two sets <strong>to</strong> move <strong>to</strong>gether by age. At SLA level, deaths <strong>are</strong> quite small in number,<br />
and, while adequate <strong>to</strong> determine median age at death, <strong>are</strong> <strong>to</strong>o unstable by single year <strong>to</strong><br />
discriminate well between SLAs f<strong>or</strong> planning purposes. A surviving population measure<br />
is m<strong>or</strong>e stable. What is needed is a distribution that matches the residential aged c<strong>are</strong><br />
residents’ profile by SLA. The curve of survival above the life expectancy age is the<br />
same shape as the last half of the curve of residents in aged c<strong>are</strong>. If that last part of the<br />
survival curve, by SLA, were mirr<strong>or</strong>ed about the vertical from the life expectancy age, the<br />
resulting distribution would m<strong>or</strong>e closely match the residential distribution. This would<br />
167
BRIAN FLEMING<br />
Table 4: Median Age at Death, Persons, South Australian Areas (SLAs) Grouped<br />
in<strong>to</strong> Commonwealth Planning Regions<br />
South Australian Region<br />
Whyalla and far n<strong>or</strong>th Non-metropolitan 70.3<br />
Riverland planning regions 76.3<br />
Eyre 76.4<br />
South East 76.6<br />
Y<strong>or</strong>ke &Barossa 77.4<br />
Hills Mallee 77.4<br />
Mid n<strong>or</strong>th<br />
77.8<br />
N<strong>or</strong>th Metropolitan regions 73.7<br />
South 78.0<br />
West 78.4<br />
East<br />
80.3<br />
Median age at death<br />
(yrs)<br />
have the effect of doubling the population survival count at a given age. Since the<br />
resulting count is <strong>to</strong> be used relatively, as it is distributional, the effect of doubling the<br />
count and allocating prop<strong>or</strong>tions is the same as counting the <strong>or</strong>iginal half and allocating<br />
prop<strong>or</strong>tions.<br />
ABS data was obtained on the population single ages from the 1996 census 13 . The<br />
calculation is done f<strong>or</strong> regions and the method is illustrated in Figure 12. Take the region<br />
in the <strong>to</strong>p row and the median age at death from the c<strong>or</strong>responding column in the second<br />
row. The population greater than <strong>or</strong> equal <strong>to</strong> the median age at death is read from the first<br />
column at the bot<strong>to</strong>m of the table. The existing benchmark process reads the population<br />
of each region from the 70+ row. So, f<strong>or</strong> example f<strong>or</strong> the n<strong>or</strong>thern metropolitan region,<br />
the median age at death is 74 and the population is 9845, shown shaded in dark, rather<br />
than the 70+ population of 15 410, unshaded.<br />
A comparison of the prop<strong>or</strong>tion of places allocated <strong>to</strong> different regions using the<br />
population over comp<strong>are</strong>d with the population older than the median age is shown at<br />
Figure 13. The prop<strong>or</strong>tion of places that would ‘move’ is about 15 per cent; given 13 000<br />
<strong>to</strong>tal places in South Australia, about 2 000 would move, summarised in Table 5.<br />
13 ABS projected populations, f<strong>or</strong> 1997-99, were only available in 5-year age groupings and<br />
individual ages <strong>are</strong> necessary <strong>to</strong> plan at different ages. This is not imp<strong>or</strong>tant f<strong>or</strong> the<br />
comparison as the same population base is used, and individual age projections can be<br />
sought from ABS.<br />
168
TARGETING AGED CARE TO PEOPLE WHO ARE DISADVANTAGED<br />
Figure 12: Determining the Population by Using a Life Expectancy Approach<br />
Whyalla Y<strong>or</strong>ke Lwr<br />
Planning regionN<strong>or</strong>th South West East Eyre<br />
Hills<br />
Mallee<br />
Flinders N<strong>or</strong>th<br />
Mid N<strong>or</strong>thRiverlandSouth East Far N<strong>or</strong>thBarossa<br />
Totals<br />
Med age at<br />
death - person<br />
= 'X' 74 78 78 80 76 77 78 76 77 70 77<br />
Population 'X' + 9845 13438 11030 12141 1521 4065 1302 1603 2292 3043 3684 63964<br />
Region sh<strong>are</strong><br />
<strong>to</strong>tal based on<br />
70+ pop 11.13% 22.78% 19.17% 22.81% 2.02% 6.31% 2.24% 2.25% 3.50% 2.20% 5.59% 1<br />
Region sh<strong>are</strong><br />
based on<br />
median age<br />
"X"+ 15.39% 21.01% 17.24% 18.98% 2.38% 6.36% 2.04% 2.51% 3.58% 4.76% 5.76% 1<br />
abs (med -70+) 4.26% 1.77% 1.93% 3.83% 0.35% 0.04% 0.20% 0.26% 0.08% 2.56% 0.17% 0.154688133<br />
Population 65 + 24099 44037 36962 42721 4133 12711 4586 4610 7129 4881 11274<br />
66+ 22208 41648 34927 40544 3842 11917 4277 4321 6658 4447 10534<br />
67+ 20367 39199 32988 38290 3559 11085 3987 4032 6156 4099 9814<br />
68+ 18671 36704 30899 36058 3298 10302 3686 3703 5710 3696 9110<br />
69+ 17009 34134 28756 33886 3070 9524 3377 3410 5277 3362 8393<br />
70+ 15410 31541 26547 31591 2802 8738 3101 3113 4850 3043 7734 138470<br />
71+ 13887 29014 24294 29256 2573 7964 2824 2839 4422 2736 7020<br />
72+ 12490 26566 22197 27096 2335 7220 2589 2612 4029 2469 6390<br />
73+ 11128 24177 20038 24865 2122 6518 2315 2349 3657 2219 5841<br />
74+ 9845 21734 18011 22703 1911 5874 2080 2078 3271 1954 5233<br />
75+ 8631 19376 16033 20630 1727 5215 1870 1833 2943 1743 4704<br />
76+ 7453 17095 14051 18591 1521 4645 1639 1603 2596 1520 4166<br />
77+ 6341 15097 12319 16731 1370 4065 1452 1432 2292 1339 3684<br />
78+ 5594 13438 11030 15198 1194 3611 1302 1266 2029 1186 3256<br />
79+ 4876 11792 9754 13660 1052 3153 1140 1113 1778 1033 2866<br />
80+ 4239 10223 8543 12141 916 2755 992 972 1548 861 2469<br />
169
BRIAN FLEMING<br />
Figure 13: Comparison of the Prop<strong>or</strong>tion of <strong>Aged</strong> <strong>C<strong>are</strong></strong> Services by Region Using<br />
Median Age at Death (+) versus 70 Years from Birth(+).<br />
25.00%<br />
Comparison between prop<strong>or</strong>tions of places by region using 70+ vs median age at death, SA planning<br />
i<br />
20.00%<br />
15.00%<br />
10.00%<br />
5.00%<br />
Sources<br />
ABS data<br />
1996 and 0.00%<br />
1997/8<br />
N<strong>or</strong>th South West East Eyre<br />
Hills<br />
Mallee<br />
Mid N<strong>or</strong>th Riverland South<br />
E t<br />
Whyalla Y<strong>or</strong>ke Lwr<br />
Flinders N<strong>or</strong>th<br />
Far N<strong>or</strong>th Barossa<br />
70 + 11.13% 22.78% 19.17% 22.81% 2.02% 6.31% 2.24% 2.25% 3.50% 2.20% 5.59%<br />
median age 15.39% 21.01% 17.24% 18.98% 2.38% 6.36% 2.04% 2.51% 3.58% 4.76% 5.76%<br />
Source: ABS 1996 Census<br />
Table 5: The Change in Service Distribution Using Median Age at Death<br />
Pop 70+ Median age Change Absolute change<br />
Percentages<br />
N<strong>or</strong>th 11.13 14.10 2.97 2.97<br />
South 22.78 24.66 1.88 1.88<br />
West 19.17 15.93 -3.24 3.24<br />
East 22.81 19.83 -2.98 2.98<br />
Eyre 2.02 2.48 0.46 0.46<br />
Hills Mallee 6.31 5.90 -0.41 0.41<br />
Mid N<strong>or</strong>th 2.24 1.86 -0.38 0.38<br />
Riverland 2.25 2.99 0.74 0.74<br />
South East 3.50 3.74 0.24 0.24<br />
Whyalla Flinders Far N<strong>or</strong>th 2.20 3.19 0.99 0.99<br />
Y<strong>or</strong>ke Lower N<strong>or</strong>th Barossa 5.59 5.32 -0.27 0.27<br />
100.00% 0.00 14.56<br />
The results <strong>are</strong> consistent with what one would expect from a distribution of services<br />
based on life expectancy given the spatial segregation of South Australia shown in social<br />
atlases (Glover, Shand et al., 1996; Glover and Tennant, 1999). The N<strong>or</strong>th Metropolitan<br />
region ‘sh<strong>are</strong>’ of a given resource would rise, as the last two years of life would be<br />
experienced at a younger age. The demonstration has been with median age, as a proxy<br />
170
TARGETING AGED CARE TO PEOPLE WHO ARE DISADVANTAGED<br />
f<strong>or</strong> life expectancy, and so would distribute relatively m<strong>or</strong>e services <strong>to</strong> structurally<br />
younger populations. A m<strong>or</strong>e sophisticated approach could be envisaged by calculating<br />
male and female provision separately, based on a one- year expected residence f<strong>or</strong> males<br />
and two years f<strong>or</strong> females, from Table 1. F<strong>or</strong> policy purposes however, it may be<br />
preferable <strong>to</strong> say simply that services <strong>are</strong> planned on known patterns of use.<br />
It should be noted that, in South Australia, based on the current planning benchmark<br />
100/1000 70+, there is a large ‘oversupply’ of places in the East region, a residential aged<br />
c<strong>are</strong> variant of the inverse c<strong>are</strong> law. 14 Life expectancy, if calculated by region, <strong>or</strong> by<br />
Statistical Local Area (SLA), uses deaths data and it is known that the calculation is<br />
affected by the rec<strong>or</strong>ded ‘usual residence’ at death. So, if people from other regions, <strong>who</strong><br />
<strong>are</strong> likely <strong>to</strong> die younger, <strong>are</strong> unable <strong>to</strong> receive c<strong>are</strong>, in the last two years of life, in their<br />
home region and move <strong>to</strong> the East, <strong>to</strong> access the high supply, the life expectancy of the<br />
East will reduce as an artefact. The effect will be <strong>to</strong> attenuate the differences between<br />
regional life expectancy. So the method, if anything, will underestimate the size of the<br />
redistribution required, at least at first.<br />
Supp<strong>or</strong>ting Data on Actual Use<br />
In the next section the the<strong>or</strong>y, that there <strong>are</strong> spatial differences in the age at which<br />
populations use aged c<strong>are</strong> services, consistent with m<strong>or</strong>tality experience, is confirmed in<br />
two ways. One is that potential residents <strong>are</strong> assessed at different ages by region. Another<br />
is that the actual use of residential aged c<strong>are</strong> shows a variation of age by region.<br />
Assessment<br />
Assessment f<strong>or</strong> entry <strong>to</strong> aged c<strong>are</strong> is carried out independent of services by an <strong>Aged</strong> <strong>C<strong>are</strong></strong><br />
Assessment Team (ACAT) in each planning region. The ACAT evaluation team rep<strong>or</strong>t<br />
shows a picture of assessments at higher ages in the east comp<strong>are</strong>d with other regions<br />
(Basso, Pretreger et al., 1999: 22).<br />
While the variation in age is small, it should be noted that ACATs assess f<strong>or</strong> m<strong>or</strong>e than<br />
residential aged c<strong>are</strong> and the variation in age at assessment is consistent, f<strong>or</strong> example,<br />
with higher life expectancy in the east 15 .<br />
The median age is higher than the mean age in each case indicating some skewness in<br />
assessment age in the distribution.<br />
14 ‘The availability of good medical c<strong>are</strong> tends <strong>to</strong> vary inversely with the need f<strong>or</strong> it in the population<br />
served … This ... operates m<strong>or</strong>e completely where medical c<strong>are</strong> is most exposed <strong>to</strong> market f<strong>or</strong>ces,<br />
and less so where such exposure is reduced’ Hart, J. T. (1971), 405-12, 'Commentary: Three decades<br />
of the inverse c<strong>are</strong> law' Hart, 2000: 18-19.<br />
15 A caution must be noted that this is assessment of eligibility f<strong>or</strong>, not the same as admission <strong>to</strong> aged<br />
c<strong>are</strong>.<br />
171
BRIAN FLEMING<br />
Table 6: ACAT Client Age by Team(s) 1998<br />
ACAT team(s) Median Mean<br />
N<strong>or</strong>thern 82 80.4<br />
Western 82 80.6<br />
Southern 83 81.8<br />
Eastern 83 82.1<br />
All Metropolitan 83 81.2<br />
All Country 82 81.4<br />
Source: ACAT Evaluation Unit Rep<strong>or</strong>t Jan-Jun 1998.<br />
Residential <strong>Aged</strong> <strong>C<strong>are</strong></strong><br />
Data were obtained on the age at entry <strong>to</strong> residential aged c<strong>are</strong>. A potential confounder is,<br />
as noted above, that there is high supply in the East region and low supply in the N<strong>or</strong>th<br />
region, against the benchmark. This means that the age of existing residents will not truly<br />
reveal any pattern in the predicted direction, <strong>to</strong> the extent that younger residents move<br />
from N<strong>or</strong>th <strong>to</strong> East <strong>to</strong> gain services. Acc<strong>or</strong>dingly, data were extracted on a cross section<br />
of residents in permanent residential aged c<strong>are</strong> at 31 December 2000 and divided in<strong>to</strong><br />
regions based on the address rec<strong>or</strong>ded when the aged c<strong>are</strong> assessment had been made.<br />
The assessment f<strong>or</strong>m asks f<strong>or</strong> ‘preferred contact address’ and it is possible that a<br />
prop<strong>or</strong>tion of these will have the address of a friend <strong>or</strong> relative not in the same home<br />
region as the resident. This is a limitation of the data collection. The results <strong>are</strong> shown in<br />
Table 7 by sex, separately f<strong>or</strong> metropolitan and non-metropolitan regions and ranked by<br />
female mean age, females being the main users of residential aged c<strong>are</strong>.<br />
The age differences <strong>are</strong> notable. F<strong>or</strong> comparison, a two-year difference in life expectancy<br />
is the estimated impact of eliminating all cancer.<br />
The use of contact address is unlikely <strong>to</strong> have an impact. There would have <strong>to</strong> be younger<br />
aged c<strong>are</strong> residents from higher socioeconomic <strong>are</strong>as systematically giving lower<br />
socioeconomic <strong>are</strong>a contact addresses, <strong>or</strong> older people from lower socioeconomic <strong>are</strong>as<br />
systematically giving higher socioeconomic <strong>are</strong>a contact addresses, f<strong>or</strong> the result <strong>to</strong> be in<br />
doubt. This may happen if the individual circumstances of the person were not that of the<br />
<strong>are</strong>a, the ecological fallacy, in which case the underlying association with socioeconomic<br />
circumstances would, ironically, be confirmed. It seems m<strong>or</strong>e likely that the impact<br />
would be <strong>to</strong> attenuate the real differences by younger people from lower socioeconomic<br />
<strong>are</strong>as giving a higher socioeconomic <strong>are</strong>a as the, say, child’s address.<br />
Comparing The Ranking of Regions Using Median Age at Death and Age at Entry.<br />
The ranking of the regions in Table 4 and Table 7 is similar, with an outlier of Eyre. The<br />
median age at death of persons in Eyre is affected by the size of the indigenous population<br />
relative <strong>to</strong> the non-indigenous population, with indigenous deaths at younger ages. The<br />
172
TARGETING AGED CARE TO PEOPLE WHO ARE DISADVANTAGED<br />
Table 7: Age at Admission by Region: SA Residents in Permanent <strong>C<strong>are</strong></strong> by<br />
Preferred Contact Address and Age at Date of Admissions: 31 December 2000<br />
Ranked by female mean age.<br />
Female<br />
Male<br />
Metro Mean Age Median Age Mean Age Median Age<br />
MetroN<strong>or</strong>th 83.6 84 80.3 81<br />
MetroWest 84.7 86 81.5 82<br />
MetroSouth 85.3 86 82.3 83<br />
MetroEast 85.4 87 81.5 83<br />
Non-Metro<br />
WhyallaFlindersFarN<strong>or</strong>th 81.4 83 78.8 80<br />
Riverland 84.3 85 82.1 84<br />
SouthEast 84.4 85 82.0 83<br />
MidN<strong>or</strong>th 84.6 86 79.5 82<br />
Y<strong>or</strong>keLwrNthBarossa 84.7 86 81.1 82<br />
HillsMalleeSouthern 85.0 86 81.0 82<br />
Eyre 87.4 88 80.3 81<br />
residential aged c<strong>are</strong> data <strong>are</strong> from non-indigenous providers obtained via the payments<br />
system f<strong>or</strong> standard, aged c<strong>are</strong> services. Data were not obtained on the ages of people in<br />
indigenous aged c<strong>are</strong> programs in the Eyre region, which have a different funding<br />
mechanism, where age is not rec<strong>or</strong>ded.<br />
With Eyre excluded, the association between the rank of the planning region based on<br />
median age at death (persons) and the rank of the region based on the mean female age at<br />
entry <strong>to</strong> aged c<strong>are</strong> is significant. 16 With Eyre included the rank c<strong>or</strong>relation two tailed p=<br />
0.117, and with Eyre excluded p = 0.009.<br />
4 Discussion<br />
This paper is not concerned with the overal quantum of places of aged c<strong>are</strong>, rather their<br />
distribution. Some caution would be necessary in the use of life expectancy f<strong>or</strong> other than<br />
16 Note that the deaths data were f<strong>or</strong> persons as it is intended <strong>to</strong> use general population data as the<br />
planning <strong>to</strong>ol. The age at entry is f<strong>or</strong> females, the main users of aged c<strong>are</strong>.<br />
173
BRIAN FLEMING<br />
Table 8: The Ranking of South Australia Regions by Median Age at Death (Persons)<br />
Comp<strong>are</strong>d with Age of Female Residents at Entry <strong>to</strong> Residential <strong>C<strong>are</strong></strong> by Contract<br />
Address<br />
Including Eyre Excluding Eyre<br />
Rank a Rank b Rank a Rank b<br />
Whyalla, Flinders, Far N<strong>or</strong>th 1 1 1 1<br />
N<strong>or</strong>th 2 2 2 2<br />
Eyre 3 11<br />
Riverland 4 3 3 3<br />
Hills Mallee 5 8 4 8<br />
South East 6 4 5 4<br />
Y<strong>or</strong>ke, Lower, N<strong>or</strong>th Barossa 7 6 6 6<br />
South 8 9 7 9<br />
West 9 7 8 7<br />
Mid N<strong>or</strong>th 10 5 9 5<br />
East 11 10 10 10<br />
distributive effects. Life expectancy has increased since the 100/1000 70+ f<strong>or</strong>mula was<br />
introduced in 1986, but the absolute period of life with a disability is either not changing<br />
<strong>or</strong> may be slightly decreasing (Mathers and Robine 1998). 17 The disability-free years of<br />
life <strong>are</strong> increasing, and increasing as a prop<strong>or</strong>tion of life, f<strong>or</strong> disability requiring<br />
residential c<strong>are</strong>. <strong>People</strong> were not ‘sicker’ <strong>or</strong> m<strong>or</strong>e frail, f<strong>or</strong> longer periods of their life, in<br />
1997 than they were in 1985, when the f<strong>or</strong>mula was introduced. So if the f<strong>or</strong>mula,<br />
100/1000 70+, described the ‘c<strong>or</strong>rect’ prop<strong>or</strong>tion of the 1985 population requiring<br />
services, it now describes a greater prop<strong>or</strong>tion of the population, yet there is increasing<br />
demand.<br />
Table 9: Expectation of Life at Birth and at 65 Years: 1985 and 1997<br />
c1985 1996-8<br />
Expectation of life Male Female Male Female<br />
At birth 71.2 78.2 75.86 81.52<br />
At age 65 13.7 17.9 16.32 20.01<br />
Source: ABS (1999), Catalogue No. 3302.0<br />
Drivers of demand have had some scrutiny. High levels of personal c<strong>are</strong> can be met by<br />
committed and skilled c<strong>are</strong>rs, and c<strong>are</strong>r supp<strong>or</strong>t, <strong>or</strong> lack of it, is a critical fac<strong>to</strong>r in<br />
admission <strong>to</strong> residential aged c<strong>are</strong>, separate from clinical measures of the individual. <strong>C<strong>are</strong></strong><br />
needs can be met at home; the maj<strong>or</strong>ity of c<strong>are</strong>rs <strong>are</strong> spouses and the children of people<br />
17 The compression of m<strong>or</strong>bidity thesis was advanced by Fries in (1989: 205-28).<br />
174
TARGETING AGED CARE TO PEOPLE WHO ARE DISADVANTAGED<br />
entering aged c<strong>are</strong> services <strong>are</strong> themselves nearing retirement ages (Gibson 1996). Gibson<br />
and Liu (1995) suggest that structural ageing has an effect. This is <strong>to</strong> say that the need f<strong>or</strong><br />
aged c<strong>are</strong> increases with age, such that the p<strong>or</strong>tion of the population 80+ has a higher risk<br />
of admission <strong>to</strong> aged c<strong>are</strong>, and so an increasing prop<strong>or</strong>tion of people 80+ increases<br />
demand, <strong>or</strong> ‘need’. This point was reiterated in an Australian Institute of Health and<br />
Welf<strong>are</strong> (2000) paper on disability and ageing, which suggested a one in three chance of a<br />
person over 65 years ever needing aged c<strong>are</strong> comp<strong>are</strong>d with a population in aged c<strong>are</strong> at<br />
any one time aged 65 years being about three per cent (Australian Institute of Health and<br />
Welf<strong>are</strong> 2000). However, it was acknowledged that this conclusion was drawn from<br />
examining the existing population in residential c<strong>are</strong>, and so could not be regarded as a<br />
statement about any objective measure of need. It also did not take increases in life<br />
expectancy in<strong>to</strong> account. Gibson’s papers point <strong>to</strong> use of disability as a guide <strong>to</strong> demand,<br />
but these measures <strong>are</strong> not available at SLA level so it is not yet feasible <strong>to</strong> use them f<strong>or</strong><br />
these purposes<br />
The fact that use of aged c<strong>are</strong> services increases with age has contributed <strong>to</strong> calls f<strong>or</strong> the<br />
80+ population <strong>to</strong> be used as a better indica<strong>to</strong>r of need. However, as has been<br />
demonstrated, age-based f<strong>or</strong>mulae deliver a higher prop<strong>or</strong>tion of services <strong>to</strong> longer lived<br />
populations, that is, <strong>to</strong> higher socioeconomic <strong>are</strong>as. The higher the age the greater that<br />
distribution. To illustrate this effect, consider the following graph, Figure 14. It shows the<br />
prop<strong>or</strong>tion of the metropolitan population above a particular age by region against the<br />
prop<strong>or</strong>tion of the existing metropolitan aged c<strong>are</strong> supply by region. The large movements<br />
by age <strong>are</strong> in the N<strong>or</strong>th and East. The N<strong>or</strong>th sh<strong>are</strong> of population declines as the age<br />
increases, and the East sh<strong>are</strong> rises. This is expected with lower life expectancy in the<br />
N<strong>or</strong>th; the higher the age the fewer surviv<strong>or</strong>s. The aged c<strong>are</strong> supply stays as h<strong>or</strong>izontal<br />
lines by age. The gap between the two lines is regarded as the ‘need’ - indicated by age, <strong>or</strong><br />
population sh<strong>are</strong> minus supply sh<strong>are</strong>. At lower ages the East supply substantially exceeds<br />
population but this narrows as the age increases. In the N<strong>or</strong>th, supply is below population<br />
at age 70+ but not at age 80+. A planning benchmark age of 80+ would see the current<br />
distribution of supply as being appropriate, perversely, because there would be fewer<br />
surviv<strong>or</strong>s in the N<strong>or</strong>th. 18 The main point from the graph is that the volatility of age based<br />
planning makes it a po<strong>or</strong> indica<strong>to</strong>r of need.<br />
Certain conditions associated with residential aged c<strong>are</strong> use may not be consistent with<br />
planning based on m<strong>or</strong>tality. The prevalence of dementia increases with age, and there<br />
may not be as strong an association of that condition with socioeconomic circumstances<br />
as there is of m<strong>or</strong>tality. However, life expectancy with dementia, beyond age 65, f<strong>or</strong> both<br />
18 Note this is not adjusted f<strong>or</strong> any coh<strong>or</strong>t settlement effects.<br />
175
BRIAN FLEMING<br />
Figure 14: The Regional Prop<strong>or</strong>tion of the Metropolitan Population Above Ages<br />
Comp<strong>are</strong>d with the Regional Prop<strong>or</strong>tion of Metropolitan <strong>Aged</strong> <strong>C<strong>are</strong></strong> Supply in<br />
South Australia<br />
0.4<br />
0.35<br />
0.3<br />
0.25<br />
0.2<br />
0.15<br />
0.1<br />
0.05<br />
Eastern<br />
N<strong>or</strong>thern<br />
Southern<br />
Western<br />
Eastern supply<br />
N<strong>or</strong>thern supply<br />
Southern supply<br />
Western supply<br />
0<br />
Sum of P65+ Sum of P70+ Sum of P80+ Sum of P85+<br />
Source: ABS (middle projection of year 2001 population) and Department of Health and<br />
<strong>Aged</strong> <strong>C<strong>are</strong></strong> Supply tables 31 January 2001<br />
sexes, has been estimated at one year, so the condition is feeding in <strong>to</strong> lifetables via agespecific<br />
death rates (Ritchie 1994).<br />
The current planning method, based on years from birth, also distributes services <strong>to</strong> <strong>are</strong>as<br />
that were settled at particular times. As Australia’s population expanded, particularly over<br />
the last 50 years, with post W<strong>or</strong>ld War II migration, new housing <strong>are</strong>as were established<br />
from greenfields. If, f<strong>or</strong> example, most people settled in an <strong>are</strong>a in 1955, when they were<br />
25, they will turn 70 <strong>to</strong>gether in 2000 and be counted f<strong>or</strong> planning purposes, while not<br />
having the age distribution of longer settled <strong>are</strong>as. Planning based on m<strong>or</strong>tality would<br />
overcome this weakness.<br />
There is a spatial distribution of the sex ratio, the number of males <strong>to</strong> 100 females. In<br />
metropolitan <strong>are</strong>as the number of females 65+ outnumbers males but this reverses in<br />
remote and some rual regions in Australia (Haberk<strong>or</strong>n, Hugo et al. 1999, 116). This is<br />
illustrated in Figure 15. Since men die younger than women, a fixed planning age delivers<br />
m<strong>or</strong>e services <strong>to</strong> longer lived women and theref<strong>or</strong>e disadvantages remote Australia f<strong>or</strong><br />
aged c<strong>are</strong> services, albeit at low numbers. Planning based on life expectancy would<br />
inc<strong>or</strong>p<strong>or</strong>ate adjustments f<strong>or</strong> such populations.<br />
176
TARGETING AGED CARE TO PEOPLE WHO ARE DISADVANTAGED<br />
Figure 15 Sex Ratio, Australia Population 65+, 1996<br />
Source: National Key Centre f<strong>or</strong> Social Applications of GIS<br />
5 Conclusion<br />
The social gradient in health persists in<strong>to</strong> old age, and there is a clear social gradient in<br />
age at death. There is a spatial distribution of socioeconomic circumstances and theref<strong>or</strong>e<br />
of life expectancy. An age-based planning mechanism, that is, years from birth, theref<strong>or</strong>e<br />
distributes finite resources spatially <strong>to</strong> longer lived populations. Perversely, the older the<br />
planning age, the greater the distribution of services would be <strong>to</strong> higher socioeconomic<br />
<strong>are</strong>as. Choosing a planning age closer <strong>to</strong> the median age at entry <strong>to</strong> aged c<strong>are</strong> services, say<br />
80 years <strong>or</strong> m<strong>or</strong>e, an app<strong>are</strong>ntly m<strong>or</strong>e meaningful age statistically, would have a<br />
distributive effect <strong>to</strong>wards higher socioeconomic <strong>are</strong>as. 19<br />
19 There <strong>are</strong> also coh<strong>or</strong>t effects of <strong>are</strong>as settled at particular times.<br />
177
BRIAN FLEMING<br />
<strong>Aged</strong> c<strong>are</strong> legislation includes the capacity <strong>to</strong> consider financial <strong>or</strong> social disadvantage<br />
and there <strong>are</strong> no current mechanisms <strong>to</strong> address this special needs group. An approach<br />
based on life expectancy, such as years <strong>to</strong> death <strong>or</strong> equal probability of death would better<br />
predict the distributed use of residential aged c<strong>are</strong> services. It would theref<strong>or</strong>e better target<br />
aged c<strong>are</strong> resources.<br />
There may be other distributive advantages. A life expectancy method can be applied <strong>to</strong><br />
particular populations other than spatially. So, f<strong>or</strong> example, there need not be a different<br />
planning approach <strong>to</strong> distributing services f<strong>or</strong> indigenous populations. 20 Similarly f<strong>or</strong><br />
rural <strong>are</strong>as, as the method adjusts f<strong>or</strong> the sex ratio change that is experienced by remote<br />
Australia, given the lower life expectancy of males. The method also adjusts f<strong>or</strong> different<br />
age structures.<br />
The method requires the calculation of life tables by region and SLA and populations<br />
projected by single age. While these <strong>are</strong> not routinely available, they do not require any<br />
additional data collection by the ABS <strong>to</strong> be produced. Home address mobility, a potential<br />
problem f<strong>or</strong> such calculations, is lowest at age 65 years (Bell and Hugo 2000: 172).<br />
Data on the age structure of persons in residential aged c<strong>are</strong> confirms a spatial pattern of<br />
use of aged c<strong>are</strong> services consistent with the association between the expectation of life<br />
and socioeconomic circumstances.<br />
References<br />
Armitage, P. and G. Berry (1994). Statistical Methods in Medical Research. Blackwell<br />
Science Ltd, Oxf<strong>or</strong>d.<br />
Australian Bureau of Statistics (ABS) (1999), Demography, South Australia, Catalogue<br />
No. 3311.4, ABS, Canberra<br />
Australian Bureau of Statistics (ABS) (1999), Deaths, Australia, Catalogue No. 3302.0<br />
ABS, Australia.<br />
Australian Institute of Health and Welf<strong>are</strong> (1999), Australia's Health 1999, Australian<br />
Institute of Health and Welf<strong>are</strong>, Canberra.<br />
Australian Institute of Health and Welf<strong>are</strong> (2000), Disability and Ageing: Australian<br />
Population Patterns and Implications, Australian Institute of Health and Welf<strong>are</strong>,<br />
Canberra<br />
Basso, P., L. Pretreger et al. (1999), <strong>Aged</strong> <strong>C<strong>are</strong></strong> Assessment Program South Australia<br />
Evaluation Unit Rep<strong>or</strong>t, Department of Human Services, South Australia, Adelaide.<br />
Bell, M. and G. Hugo (2000), Internal Migration in Australia 1991-1996, Australian<br />
Population, Immigration and Multicultural Research Program, Commonwealth of<br />
Australia, Canberra.<br />
20 Tacit acceptance of planning f<strong>or</strong> aged c<strong>are</strong> bearing some relationship <strong>to</strong> life expectancy has been the<br />
different planning age used by the Commonwealth f<strong>or</strong> Ab<strong>or</strong>iginal and T<strong>or</strong>res Strait Islander<br />
populations, that is, the population aged 50+ rather than 70+.<br />
178
TARGETING AGED CARE TO PEOPLE WHO ARE DISADVANTAGED<br />
Commonwealth of Australia (1986), Nursing Homes and Hostels Review, Department of<br />
Community Services and Health, Canberra.<br />
Fries, J. F. (1989), 'The compression of m<strong>or</strong>bidity: near <strong>or</strong> far?, The Milbank Quarterly,<br />
67 (2): 208-28.<br />
Fuchs, V. R. (1984), '"Though much is taken": reflections on ageing, health, and medical<br />
c<strong>are</strong>', Milbank Mem<strong>or</strong>ial Fund Quarterly/Health and Society, 62 (2), 143-67.<br />
Gibson, D. (1996), 'Ref<strong>or</strong>ming aged c<strong>are</strong> in Australia: change and consequence', Journal<br />
of Social Policy, 2, 157–79.<br />
Gibson, D. and Z. Liu (1995), 'Planning ratios and population growth: will there be a<br />
sh<strong>or</strong>tfall in residential aged c<strong>are</strong> by 2021?' Australian Journal on Ageing, 14 (2),<br />
57-62.<br />
Glover, J., M. Shand, et al. (1996), A social health atlas of South Australia, South<br />
Australian Health Commission, Commonwealth of Australia, Adelaide,.<br />
Glover, J. and S. Tennant (1999a), A Social Health Atlas of Australia, Public Health<br />
Inf<strong>or</strong>mation Development Unit, Commonwealth of Australia, Adelaide.<br />
Glover, J. and S. Tennant (1999b), A Social Health Atlas of Australia, Public Health<br />
Inf<strong>or</strong>mation Development Unit, Commonwealth of Australia, Canberra.<br />
Glover, J. and T. Woollacott (1992), A Social Health Atlas of Australia, Commonwealth<br />
of Australia, Adelaide.<br />
Haberk<strong>or</strong>n, G., G. Hugo et al. (1999), Country Matters Social Atlas of Rural and<br />
Regional Australia, Commonwealth of Australia Bureau of Rural Sciences,<br />
Canberra.<br />
Hart, J. T. (1971), 'The inverse c<strong>are</strong> law', Lancet, i, 405-12.<br />
Hart, J. T. (2000), 'Commentary: three decades of the inverse c<strong>are</strong> law' British Medical<br />
<strong>C<strong>are</strong></strong> Journal, 320, 1 January, 18-19.<br />
Himsw<strong>or</strong>th, R. L. and M. J. Goldacre (1999), 'Does time spent in hospital in the final 15<br />
years of life increase with age at death? A population based study', British Medical<br />
Journal, 319, November, 1338-39.<br />
Mathers, C. D. and J. M. Robine (1998), 'International trends in health expectancies: a<br />
review', Australasian Journal on Ageing, 17, 1 Supplement, 51-5.<br />
Ritchie, K. (1994), International comparisons of dementia-free life expectancy: a critical<br />
review of the results obtained, Advances in Health Expectancies, Australian<br />
Institute of Health and Welf<strong>are</strong>, Canberra.<br />
van Weel, C. and J. Michels (1997), 'Dying, not old age, <strong>to</strong> blame f<strong>or</strong> costs of health c<strong>are</strong>',<br />
Lancet, 350 (9085) 1159-60.<br />
Vic<strong>to</strong>ria (1999), Burden of Disability Study,<br />
http://www.dhs.vic.gov.au/phb/9903009/index<br />
179