Voice evaluation registration packet
Voice evaluation registration packet
Voice evaluation registration packet

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
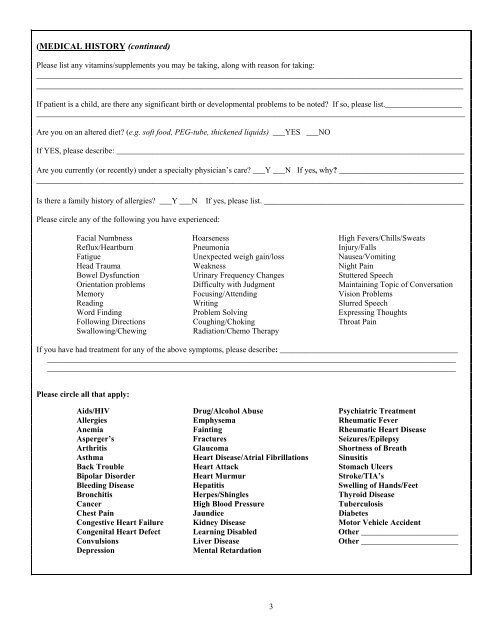
(MEDICAL HISTORY (continued)<br />
Please list any vitamins/supplements you may be taking, along with reason for taking:<br />
___________________________________________________________________________________________________<br />
________________________________________________________________________________________________<br />
If patient is a child, are there any significant birth or developmental problems to be noted? If so, please list.___________________<br />
__________________________________________________________________________________________________________<br />
Are you on an altered diet? (e.g. soft food, PEG-tube, thickened liquids) ___YES ___NO<br />
If YES, please describe: ______________________________________________________________________________________<br />
Are you currently (or recently) under a specialty physician’s care? ___Y ___N If yes, why? ____________________________<br />
________________________________________________________________________________________________<br />
Is there a family history of allergies? ___Y ___N If yes, please list. _____________________________________________<br />
Please circle any of the following you have experienced:<br />
Facial Numbness Hoarseness High Fevers/Chills/Sweats<br />
Reflux/Heartburn Pneumonia Injury/Falls<br />
Fatigue Unexpected weigh gain/loss Nausea/Vomiting<br />
Head Trauma Weakness Night Pain<br />
Bowel Dysfunction Urinary Frequency Changes Stuttered Speech<br />
Orientation problems Difficulty with Judgment Maintaining Topic of Conversation<br />
Memory Focusing/Attending Vision Problems<br />
Reading Writing Slurred Speech<br />
Word Finding Problem Solving Expressing Thoughts<br />
Following Directions Coughing/Choking Throat Pain<br />
Swallowing/Chewing<br />
Radiation/Chemo Therapy<br />
If you have had treatment for any of the above symptoms, please describe: ____________________________________________<br />
_____________________________________________________________________________________________________<br />
_____________________________________________________________________________________________________<br />
Please circle all that apply:<br />
Aids/HIV Drug/Alcohol Abuse Psychiatric Treatment<br />
Allergies Emphysema Rheumatic Fever<br />
Anemia Fainting Rheumatic Heart Disease<br />
Asperger’s Fractures Seizures /Epilepsy<br />
Arthritis Glaucoma Shortness of Breath<br />
Asthma Heart Disease/Atrial Fibrillations Sinusitis<br />
Back Trouble Heart Attack Stomach Ulcers<br />
Bipolar Disorder Heart Murmur Stroke/TIA’s<br />
Bleeding Disease Hepatitis Swelling of Hands/Feet<br />
Bronchitis Herpes/Shingles Thyroid Disease<br />
Cancer High Blood Pressure Tuberculosis<br />
Chest Pain Jaundice Diabetes<br />
Congestive Heart Failure Kidney Disease Motor Vehicle Accident<br />
Congenital Heart Defect Learning Disabled Other ________________________<br />
Convulsions Liver Disease Other ________________________<br />
Depression<br />
Mental Retardation<br />
3