MoPRO Annual Report - Primaris
MoPRO Annual Report - Primaris
MoPRO Annual Report - Primaris

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
2002<br />
ANNUAL<br />
REPORT
contents<br />
Section I. . . . . . . . . Pages 5-12<br />
Health Care Quality Improvement<br />
Section II . . . . . . . Pages 13-16<br />
Payment Error Prevention<br />
Section III. . . . . . . Pages 15-16<br />
Consumer Protection<br />
Section IV . . . . . . . . . . Page 17<br />
Health Care Consulting<br />
Section V . . . . . . . . . . Page 18<br />
Board of Directors
(L-R): James T. Rogers, MD, FACP (Springfield), Chairman of the Board,<br />
Richard A. Royer (Columbia), Chief Executive Officer<br />
open letter<br />
In 2000 the Centers for Medicare & Medicaid<br />
Services (CMS) set an ambitious strategic goal<br />
for MissouriPRO: statewide improvement in 23<br />
indicators of care across seven clinical topics<br />
by 2003.<br />
Needless to say, the task was daunting.<br />
Success would require working with all 101<br />
acute care hospitals and a significant portion<br />
of the 20,000 physicians that serve almost<br />
900,000 Missourians enrolled in Medicare.<br />
In spite of the challenges and very short<br />
timeframe, Missouri’s health care community<br />
heard our "call to action" and achieved<br />
improvement. By 2002, Missouri jumped from<br />
33rd to 26th in the nation in quality care<br />
provided to Medicare beneficiaries.<br />
beneficiaries and reduce hospital adverse<br />
events associated with surgical/invasive<br />
procedures. All these accomplishments help<br />
ensure quality and safe health care for<br />
Missouri’s residents.<br />
Overall, 2002 has been a tremendous year for<br />
MissouriPRO. As this report clearly<br />
demonstrates, collaboration marks the heart<br />
of our success. We thank all of our esteemed<br />
partners, Missouri Hospital Association, Missouri<br />
Association of Osteopathic Physicians and<br />
Surgeons, Missouri State Medical Society,<br />
CMS, and each and every health care<br />
provider who made a conscious choice to<br />
collaborate with us to create positive change<br />
in the quality and safety of health care in<br />
Missouri. Our accomplishments are also the<br />
result of the strong commitment and<br />
dedication of our Board of Directors and staff.<br />
We look forward to the new challenges CMS<br />
presents in 2003 and beyond.<br />
Our accomplishments this year go beyond<br />
achieving our quality improvement goals.<br />
Through the efforts of our Payment Error<br />
Prevention Program, Missouri’s inpatient<br />
payment error rate was reduced by 11%. Our<br />
internal case review process was awarded<br />
Health Utilization Management Accreditation<br />
by URAC. Moreover, we were awarded<br />
several grants; a few of which are to increase<br />
mammograms among St. Louis African<br />
American women, monitor Medigap<br />
guaranteed issue rights for Medicare<br />
Sincerely,<br />
James T. Rogers, MD, FACP<br />
Chairman<br />
Richard A. Royer<br />
Chief Executive Officer<br />
2
our<br />
Committed to positive change in<br />
health care quality<br />
Mission<br />
3
Achievements<br />
2000-2002<br />
• Missouri jumped from 35rd to 28th<br />
in the nation in overall quality of<br />
care provided to Medicare<br />
beneficiaries.<br />
• For the first time, 113 out of 114<br />
hospitals worked on improving<br />
quality of care in at least one<br />
national clinical topic.<br />
• Missouri was one of the first 10<br />
states to begin rapid cycle<br />
collaboratives among hospitals<br />
and physician offices designed<br />
to improve patient care quickly<br />
and efficiently.<br />
• Diabetes care was significantly<br />
enhanced for almost 9,000<br />
beneficiaries who received<br />
lipid profile, A1C, and retinal<br />
eye exams.<br />
• Over half (54%) of Medicare<br />
patients admitted to the hospital<br />
for a heart attack and who smoke<br />
were counseled to quit, a 16%<br />
increase from 1998 estimates,<br />
placing Missouri third in the US on<br />
this indicator of care.<br />
• Three-out-of-four Medicare<br />
beneficiaries were immunized<br />
against influenza in 2001; a nearly<br />
10% increase over two years<br />
earlier and 5% higher than the<br />
national average of 72%.<br />
• Over 68,000 Medicare women<br />
received their annual mammogram;<br />
2,588 more than in previous years.<br />
• Missouri’s inpatient Medicare<br />
payment error rate dropped 11%,<br />
an estimated savings of $4.3 million<br />
to the Medicare Trust Fund.<br />
• 40,000 seniors were reminded to<br />
get their flu and pneumonia shots<br />
through a partnership with the<br />
Show-Me State Adult Immunization<br />
Coalition.<br />
• Over $3.5 million in out-of-pocket<br />
expenses were saved for more<br />
than 15,000 Medicare consumers<br />
through counseling provided by<br />
our CLAIM Program volunteers.<br />
• Maintained 99% timeliness on all<br />
mandatory case reviews,<br />
exceeding the national<br />
requirement of 80%.<br />
• Awarded 6 additional contracts for<br />
external review of Medicaid<br />
managed care, quality<br />
improvement in critical access<br />
hospitals, Medigap, patient safety,<br />
breast cancer public education<br />
and smoking cessation.<br />
• Received three public<br />
relations/marketing awards.<br />
4
Quality Improvement<br />
Hospitals<br />
MissouriPRO encourages hospitals to<br />
measure performance in order to<br />
understand and improve their systems of<br />
care. Evidence suggests that welldesigned<br />
system changes significantly<br />
reduce readmissions, improve quality of life,<br />
and reduce health care costs while<br />
improving patient self-management and<br />
satisfaction.<br />
We provide hospitals with reports on their<br />
performance in clinical topics chosen by<br />
CMS along with national, statewide, and<br />
benchmark rates. These reports help<br />
hospitals strategically evaluate their care.<br />
5<br />
When an opportunity for improvement in<br />
care is identified, MissouriPRO assists<br />
hospitals in examining their processes,<br />
pinpointing system breakdowns, and<br />
choosing appropriate solutions. Hospitals<br />
can make changes quickly with access to<br />
our comprehensive, evidence-based<br />
quality improvement resources, including<br />
pocket cards for physicians, tip sheets, and<br />
chart stickers. This year, over 75,000 tools<br />
were ordered by Missouri hospitals.<br />
We also offer opportunities for hospitals to<br />
interact in structured Collaboratives.<br />
Participants are exposed to interactive<br />
learning sessions where teams study<br />
methods of change, and action periods<br />
where teams test and implement changes
in their facilities. In 2002, 11 critical<br />
access hospitals participated in a<br />
Collaborative sponsored jointly by<br />
MissouriPRO and Missouri<br />
Department of Health & Senior<br />
Services (DHSS), Office of Rural<br />
Health. The project was designed<br />
to prevent system failures and<br />
medication errors. MissouriPRO<br />
also joined a team from Heartland<br />
Regional Medical Center in the first<br />
nationwide Surgical Site Infection<br />
Prevention Collaborative hosted by<br />
CMS.<br />
Further enhancing our work with<br />
hospitals is our participation in a<br />
Patient Safety Demonstration<br />
Project. MissouriPRO, in partnership<br />
with DHSS, HealthInsight (the Utah<br />
QIO), and the Utah Department of<br />
Health, is working with hospitals to<br />
identify critical processes and<br />
causes related to adverse surgical<br />
events, barriers to change, and<br />
Stroke/Atrial<br />
Fibrilation<br />
Quality Indicator<br />
Avoidance of sublingual nifedipine<br />
Antithrombotic at discharge<br />
address lessons learned.<br />
MissouriPRO has designed and<br />
conducted a chart review process<br />
to identify adverse surgical events<br />
and evaluate the use of ICD-9<br />
codes for predicting adverse<br />
events. Conferences and regional<br />
meetings have also been held to<br />
promote patient safety best<br />
practices in participating hospitals.<br />
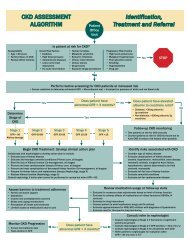
Through this approach, Missouri<br />
hospitals have achieved impressive<br />
results. Within three years hospitals<br />
improved in 14 of 17 indicators of<br />
care (see graph). Increases<br />
measuring 10% or more were<br />
recorded in smoking cessation<br />
counseling and time to angioplasty<br />
for patients admitted with an AMI,<br />
as well as in screening and/or<br />
administration of pneumonia and<br />
influenza immunizations for patients<br />
with pneumonia. Missouri was<br />
among the top 10 states in the<br />
amount of improvement for aspirin<br />
at discharge, smoking cessation<br />
counseling, and time to<br />
angioplasty.<br />
The next three years of work on<br />
CMS’ national clinical topics will be<br />
demanding. Surgical site infections<br />
will be added. We will be<br />
expected to assist hospitals in<br />
continued improvement as we<br />
simultaneously double our work<br />
with expansion into home health<br />
and nursing homes. We plan to<br />
move from individual consultations<br />
to group work in the form of<br />
Collaboratives and regional<br />
education meetings. We will<br />
continue to make our system<br />
change tools available to every<br />
hospital and place our<br />
educational materials on our<br />
website.<br />
Baseline (%) / Remeasurement (%) Rate<br />
5 10 15 20 25 30 35 40 45 50 55 60 65 70 75 80 85 90 95 100<br />
84 83<br />
92 99<br />
Quality Improvement<br />
Discharge on warfarin<br />
52 59<br />
Heart Failure<br />
Pneumonia<br />
Appropriate use/non-use of ACEI at discharge<br />
Appropriate initial empiric antibiotic<br />
Antibiotic within 8 hrs of admission<br />
79 84<br />
81 85<br />
84 84<br />
Blood culture prior to antibiotic<br />
Influenza vaccine (or screening)<br />
Pneumococcal vaccine (or screening)<br />
16 28<br />
15 25<br />
77 79<br />
Acute<br />
Myocardial<br />
Infarction<br />
ACEI at discharge for low LVEF<br />
Early administration of beta blocker<br />
Beta blocker at discharge<br />
59<br />
74 74<br />
67<br />
72 78<br />
Smoking cessation counseling<br />
38 54<br />
Early administration of aspirin<br />
76 81<br />
Aspirin at discharge<br />
78 88<br />
Combined minutes to angioplasty/thrombolysis<br />
37 56<br />
Adult<br />
Immunizations<br />
Influenza vaccinations<br />
Pneumonia vaccinations<br />
53 64<br />
68 77<br />
Diabetes<br />
<strong>Annual</strong> HbA1c<br />
72 78<br />
Biennial lipid profile<br />
57 71<br />
Biennial retinal exam<br />
67 68<br />
Breast Cancer<br />
Biennial mammogram<br />
54 59<br />
6
Physician Offices<br />
Improving the quality of care in the outpatient setting<br />
can be taxing given the sheer numbers of physicians<br />
and clinics serving Missouri seniors. To do so, we<br />
sought to communicate continually with physicians<br />
about our free assistance and systems change tools.<br />
We employed targeted mailings and faxes,<br />
educational ads and articles in physician journals and<br />
magazines, and face-to-face contacts at physician<br />
offices, conferences, and presentations. Partnership<br />
helped us further spread this information into the<br />
physician community. In the coming three years, we<br />
will expand our work with physician offices through<br />
Collaboratives and individual consultation where<br />
possible.<br />
7<br />
Atchison<br />
Holt<br />
Nodaway<br />
Worth<br />
Gentry<br />
Andrew<br />
DeKalb<br />
Buchanan<br />
Platte<br />
Clinton<br />
Clay<br />
Jackson<br />
Cass<br />
Bates<br />
Vernon<br />
Barton<br />
Jasper<br />
Newton<br />
McDonald<br />
Mercer<br />
Harrison<br />
Daviess<br />
Johnson<br />
Dade<br />
Barry<br />
Grundy<br />
Caldwell Livingston<br />
Ray<br />
Lafayette<br />
Henry<br />
St. Clair<br />
Cedar<br />
Lawrence<br />
Carroll<br />
Hickory<br />
Polk<br />
Greene<br />
Stone<br />
Putnam<br />
Sullivan<br />
Linn<br />
Saline<br />
Pettis<br />
Benton<br />
Chariton<br />
Christian<br />
Webster<br />
Taney<br />
Morgan<br />
Dallas<br />
Schuyler<br />
Scotland<br />
Adair<br />
Macon<br />
Camden<br />
Randolph<br />
Howard<br />
Cooper<br />
Moniteau<br />
Boone<br />
Wright<br />
Cole<br />
Miller<br />
Laclede<br />
Douglas<br />
Ozark<br />
Knox<br />
Shelby<br />
Pulaski<br />
Monroe<br />
Audrain<br />
Osage<br />
Texas<br />
equal to or greater<br />
than state average<br />
state average = 72.7%<br />
(average of statewide<br />
rates for A1C, lipid<br />
profiles and retinal<br />
eye exams)<br />
Clark<br />
Lewis<br />
Callaway<br />
Maries<br />
Marion<br />
Phelps<br />
Howell<br />
Ralls<br />
Gasconade<br />
Dent<br />
Diabetes Monitoring Rates<br />
Pike<br />
Oregon<br />
Franklin<br />
Crawford<br />
Shannon<br />
less than state average<br />
Washington<br />
Iron<br />
Reynolds<br />
Carter<br />
Ripley<br />
Jefferson<br />
St. Francois<br />
Madison<br />
Wayne<br />
Butler<br />
Diabetes<br />
Many older adults die each year<br />
from diabetes or suffer from<br />
related complications including<br />
blindness, kidney failure, nerve<br />
damage, and cardiovascular<br />
disease. Complications can<br />
St. Louis<br />
St. Louis City be prevented or delayed<br />
through regular clinical<br />
monitoring and selfmanagement.<br />
Ste.<br />
Genevieve<br />
Lincoln<br />
Montgomery<br />
Warren St. Charles<br />
Cape<br />
Girardeau In 2002, eight physician<br />
offices participated in<br />
Scott<br />
MissouriPRO’s first<br />
Stoddard Mississippi<br />
Diabetes<br />
New<br />
Madrid Collaborative. Using a<br />
model that specifies the<br />
Dunklin<br />
essential elements of<br />
excellent diabetes care,<br />
these clinics have achieved<br />
impressive results. Patients<br />
meeting the national goal of two<br />
A1C tests per year increased 397%<br />
after the Collaborative, and by<br />
September, 520 patients were<br />
enrolled in active care registries.<br />
These clinics are now expanding<br />
their improvements to other<br />
chronic diseases and additional<br />
sites.<br />
Bollinger<br />
Perry<br />
Pemiscot<br />
Clinical partnerships also play a<br />
key role in diabetes improvement.<br />
This past spring, the Kansas City<br />
Quality Improvement Consortium<br />
produced and distributed<br />
evidence-based medical<br />
guidelines for the treatment of<br />
diabetes and heart failure to over<br />
1,400 physicians. Rather than<br />
referring to multiple sources, these<br />
guidelines provide one reference<br />
point for practicing physicians.<br />
Representatives of local<br />
physicians, medical associations,<br />
insurers and medical schools<br />
comprise the group, along with<br />
MissouriPRO.<br />
Missouri is improving in diabetes<br />
care. Compared to two years<br />
earlier, 12,612 more Medicare<br />
diabetes patients obtained a<br />
biennial lipid profile, 9,474 more<br />
received an annual A1C, and<br />
6,423 more had a biennial eye<br />
exam. Still, most counties in<br />
Missouri need additional<br />
improvement.
Immunizations<br />
Thousands of people are hospitalized and die each year from flu and pneumonia—two vaccinepreventable<br />
diseases. Most are over age 65. Although effective vaccines exist for these diseases,<br />
Missouri’s immunization rates are substantially lower than the Healthy People 2010 goal of 90%.<br />
The Show-Me State Adult Immunization Coalition is a strategic partnership of private corporations,<br />
community organizations, and government agencies. The Coalition partnered with 27 local health<br />
departments on a statewide flu shot campaign for the 2002-2003 flu season. Flu brochures with local<br />
flu clinic locations and dates were mailed to over 40,000 Medicare beneficiaries in 27 counties with the<br />
lowest immunization rates. MissouriPRO also targeted physicians practicing in counties with the lowest<br />
immunization rates, in an effort to alert them of the poor rates within their county and offer free tools to<br />
increase immunization rates.<br />
Quality Improvement<br />
Through these efforts, we are making steady progress toward our 90% immunization goal. Three-out-offour<br />
Medicare beneficiaries were immunized against influenza in 2001, a nearly 10% increase over two<br />
years earlier. The percentage of Medicare beneficiaries who have been immunized against<br />
pneumonia since 1991 also increased to 64—11% higher than two years earlier.<br />
Atchison<br />
Holt<br />
Nodaway<br />
Worth<br />
Gentry<br />
Andrew<br />
DeKalb<br />
Buchanan<br />
Platte<br />
Mammography Rates<br />
Clinton<br />
Clay<br />
Jackson<br />
Cass<br />
Bates<br />
Vernon<br />
Barton<br />
Jasper<br />
Newton<br />
McDonald<br />
less than national<br />
average<br />
equal to or greater<br />
than national average<br />
national average = 60.2%<br />
(Medicare women age 50-69<br />
who received a mammogram)<br />
Mercer<br />
Harrison<br />
Daviess<br />
Johnson<br />
Dade<br />
Barry<br />
Grundy<br />
Caldwell Livingston<br />
Ray<br />
Lafayette<br />
Henry<br />
St. Clair<br />
Cedar<br />
Lawrence<br />
Carroll<br />
Hickory<br />
Polk<br />
Greene<br />
Stone<br />
Putnam<br />
Sullivan<br />
Linn<br />
Saline<br />
Pettis<br />
Benton<br />
Chariton<br />
Dallas<br />
Christian<br />
Webster<br />
Taney<br />
Morgan<br />
Schuyler<br />
Scotland<br />
Adair<br />
Macon<br />
Camden<br />
Randolph<br />
Howard<br />
Cooper<br />
Moniteau<br />
Boone<br />
Wright<br />
Cole<br />
Miller<br />
Laclede<br />
Douglas<br />
Ozark<br />
Knox<br />
Shelby<br />
Pulaski<br />
Monroe<br />
Osage<br />
Texas<br />
Clark<br />
Lewis<br />
Callaway<br />
Maries<br />
Marion<br />
Ralls<br />
Audrain<br />
Phelps<br />
Howell<br />
Gasconade<br />
Dent<br />
Pike<br />
Crawford<br />
Shannon<br />
Oregon<br />
Washington<br />
Iron<br />
Reynolds<br />
Carter<br />
Ripley<br />
Breast Cancer<br />
According to the American Cancer Society, next year 4,000 women in<br />
Missouri could be diagnosed with breast cancer and nearly 800 could<br />
die from the disease. While mammography is effective at detecting<br />
breast cancer in its earliest, most treatable stages, this service is underutilized<br />
among older women. Only 59% of Medicare women age 50 to<br />
69 had a mammogram between 10/1999 and 10/2001—7% below<br />
Missouri’s achievable benchmark of 67%.<br />
Jefferson<br />
Patient reminder systems have proven to be very effective in ensuring<br />
women receive a mammogram. Over 195 clinics and physician offices<br />
use the mammography recall system provided by MissouriPRO.<br />
Lincoln<br />
Montgomery<br />
Warren St. Charles<br />
St. Louis<br />
Franklin<br />
Community partnerships and strategies support the clinical changes.<br />
MissouriPRO, the American Cancer Society, and the Breast and<br />
Cervical Cancer Control Project, developed a 2002 Mother’s Day<br />
Campaign to raise awareness about the value of mammography<br />
screenings. Sixty-four mammography centers implemented the<br />
St. Louis<br />
City<br />
campaign in their communities. In fall 2002, we promoted use of<br />
Barnes-Jewish Hospital’s Mammography Van in St. Louis. Reminders<br />
Ste. were mailed to 4,000 Medicare women who did not get a<br />
Genevieve<br />
Perry mammogram in the last two years. The reminders, mailed<br />
Madison Cape twice for reinforcement, included information about the<br />
Girardeau<br />
value of mammography, Medicare coverage, and the van<br />
Scott<br />
schedule at local Schnucks markets. A grant from the<br />
Stoddard Mississippi<br />
Butler<br />
St. Louis Affiliate of the Susan G. Komen Breast Cancer<br />
New<br />
Madrid Foundation will allow us to expand this partnership activity<br />
in 2003 to African American women in St. Louis.<br />
St. Francois<br />
Wayne<br />
Bollinger<br />
Dunklin<br />
Pemiscot<br />
8
Nursing Homes<br />
Improvements in medical care and technology<br />
result in people living longer. With a longer life<br />
span and shorter acute care stays, the burden of<br />
care is falling to nursing homes and home health<br />
agencies. Providing quality improvement<br />
resources in these settings will become an<br />
important focus of our work in the coming years<br />
while maintaining improvement in the acute<br />
care and outpatient settings.<br />
9
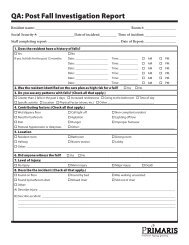
Fall Prevention<br />
To prepare for this work, MissouriPRO<br />
initiated the Fall Prevention Project for<br />
Skilled Nursing Facilities. Preventing falls<br />
and maintaining mobility is a vital quality<br />
of life issue for nursing home residents but<br />
can be difficult to achieve due to age,<br />
frailty, and physical dependence.<br />
The 12 nursing homes chosen for participation<br />
were receptive to improvement and<br />
eager to learn methods to enhance the<br />
quality of life for their residents. They<br />
received hands-on individual consultation<br />
and education along with a toolkit<br />
containing guidelines and techniques to<br />
assist them in their quality improvement<br />
work. The toolkit included samples of<br />
materials that the homes could modify for<br />
their use, such as policies and procedures,<br />
forms for risk and neurological assessments<br />
and fall investigation, and resident care<br />
plans.<br />
Facilities were encouraged to adopt a<br />
care model with the essential elements of<br />
a sustainable fall prevention program—risk<br />
assessment, care planning, and exercise.<br />
MissouriPRO assisted facilities in developing<br />
and implementing a risk assessment for<br />
every resident, with particular emphasis on<br />
new residents shortly after admission.<br />
Included in this assessment was identification<br />
of medications that could cause falls.<br />
Several facilities rewrote their policies and<br />
procedures related to falls to establish an<br />
ongoing process that would not vary with<br />
staffing changes. Risk assessments were<br />
completed on each facility’s setting to<br />
identify and eliminate environmental<br />
hazards that could contribute to falls.<br />
Using this information, a falls team could<br />
develop individual care plans and revise<br />
them regularly.<br />
Several facilities were especially successful<br />
with the "Falling Leaf Program," a special<br />
observation program that included all<br />
facility staff. The program identifies a small<br />
number of residents at high risk for falls and<br />
provides specialized observations and<br />
interventions to determine resident’s<br />
needs.<br />
This project is also a success for<br />
MissouriPRO. It allowed us to test<br />
interventions and strategies to improve<br />
care and outcomes in a setting other than<br />
acute care. It has also established a<br />
relationship with nursing homes and<br />
helped define future activities for the next<br />
three years where we will be expected to<br />
achieve statewide improvement in three<br />
clinical indicators.<br />
Over the year of the project,<br />
beginning July 2000, facilities<br />
reduced their repeat falls by 30%.<br />
Most of the improvement was due<br />
to the use of a resident<br />
observation program, low beds<br />
and system reviews. Not only did<br />
facilities develop successful fall<br />
prevention programs; they<br />
learned the essentials of the<br />
quality improvement process.<br />
They embraced the team<br />
approach to assessment, care<br />
planning, interventions, and<br />
mobility activities for residents.<br />
10<br />
Quality Improvement
Managed Care<br />
Approximately 140,000 older adults in<br />
Missouri are covered by a Medicare<br />
managed care plan. The Quality<br />
Improvement Systems for Managed<br />
Care (QISMC) Program helps protect<br />
their right to quality health care.<br />
MissouriPRO assists plans to implement<br />
QISMC by providing them with<br />
technical assistance on project<br />
development and evaluation, as well<br />
as access to our quality improvement<br />
resources.<br />
In 2002, we also supported collaborative<br />
efforts directly impacting care in<br />
Medicare managed care plans. The<br />
Kansas City Quality Improvement<br />
Consortium, which included<br />
commercial and publicly funded<br />
MCOs, disseminated uniform treatment<br />
guidelines for diabetes, heart failure,<br />
depression, and asthma to over 1,400<br />
physicians in Kansas City. We were<br />
instrumental in developing and<br />
distributing these guidelines which<br />
included CMS’ national indicators for<br />
heart failure and diabetes. In the<br />
St. Louis region, MissouriPRO is a<br />
member of the St. Louis Diabetes<br />
Coalition, also comprised of both public<br />
and commercial health plans.<br />
11
Quality Improvement<br />
Underserved Populations<br />
In St. Louis a 70-year-old African American<br />
gentleman has never had the flu shot and,<br />
in his judgement, never will. "I’ve never had<br />
the flu, so why start now?" He is set in his<br />
ways, he admits. He’s not alone.<br />
In the metropolitan St. Louis area, a mere<br />
37% of African Americans age 65 and older<br />
were immunized against the flu, according<br />
to 1997 Behavioral Risk Factor Surveillance<br />
System data. This compares to 80% for non-<br />
African Americans.<br />
Since identifying this gap, MissouriPRO is<br />
working to increase influenza immunization<br />
rates among African Americans living in<br />
St. Louis. A central feature of the project is<br />
an intensive discovery phase to gain a<br />
culturally competent understanding of the<br />
community and to identify barriers to<br />
change.<br />
that included local flu clinic information<br />
mailed to Medicare consumers.<br />
A comprehensive and culturally-directed<br />
mass media campaign drove home the<br />
message of the importance and safety of<br />
flu shots.<br />
Our results so far have shown strong<br />
evidence for providing accessible clinics<br />
supported by effective social marketing<br />
methods and culturally competent<br />
interventions to increase flu<br />
immunizations among older<br />
African Americans. We are<br />
committed to continuing<br />
this project for an additional<br />
three years. Our goal is to<br />
build on successes to establish<br />
a sustainable communitybased<br />
framework.<br />
Working closely with the St. Louis<br />
Influenza Immunization Advisory<br />
Committee, the number of local<br />
flu clinics were increased or<br />
relocated and promoted to<br />
increase access. To promote the<br />
clinics, we developed a variety of<br />
social marketing strategies to<br />
reach older African Americans<br />
during the 2001-2002 and 2002-<br />
2003 flu seasons. Our most<br />
successful strategy was a postcard<br />
12
Payment Error Prevention<br />
This year Missouri’s inpatient Medicare<br />
payment error rate declined to 2.01%, from<br />
2.25% two years earlier. This 11% reduction<br />
followed nearly three years of quality<br />
improvement interventions facilitated by<br />
MissouriPRO as part of our Payment Error<br />
Prevention Program (PEPP) activities.<br />
The PEPP, initiated by CMS in 2000, was<br />
designed to reduce the national payment<br />
error rate and to reduce the percentage of<br />
Medicare dollars improperly paid for<br />
inpatient services. It was a response to an<br />
Office of the Inspector General audit.<br />
13
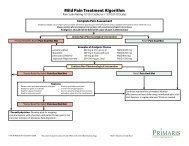
Project Results<br />
The statewide payment error rate declined following<br />
implementation of several projects facilitated by MissouriPRO.<br />
Declines in error rates were achieved in all projects associated<br />
with unnecessary admissions. The error rate related to<br />
inappropriate same day readmissions dropped to 27%, a<br />
decline of 14% from two years earlier. Hospitals that had the<br />
highest number of same day readmissions (Level III) at the<br />
beginning of the project showed a more dramatic decline in<br />
errors, dropping to 5% from 59% (see graph #1). The number<br />
of claims for DRG 462 dropped from a statewide high of 82 to<br />
14 at last measurement (see graph #2). Errors associated with<br />
short stay admissions increased from 8% to 30%, even though<br />
hospitals targeted for more intense intervention because of<br />
their high rate of short stay admissions had an error rate<br />
decline of 11% at last measurement.<br />
Our project designed to decrease DRG coding errors<br />
associated with several pulmonary conditions showed a<br />
relative improvement of 14% - 20% at remeasurement for<br />
DRGs 99/100. However, these were the only two DRG<br />
conditions among the 8 reviewed, with improvement. A<br />
recent measurement found a statewide error rate of 12%; 2%<br />
higher from two years earlier. Statistically significant increases<br />
in error rates were observed in DRGs 79/80 and DRG 475.<br />
Error Rate<br />
100%<br />
80%<br />
60%<br />
40%<br />
#1 Same Day Readmission Errors<br />
PEPP<br />
Interventions<br />
Reduction in payment errors followed nearly three years of<br />
collaborative quality improvement activities with Missouri’s<br />
acute care hospitals. Our focus promoted accurate coding,<br />
appropriate utilization, and complete medical record<br />
documentation to reduce errors associated with unnecessary<br />
admissions and miscoded DRG assignments.<br />
To evaluate areas of potential payment error in Missouri we<br />
used pattern analysis, medical record abstraction, and<br />
analysis of claims data. Once areas of concern were<br />
identified, hospitals were encouraged to examine their<br />
coding and utilization policies, procedures, and processes.<br />
We provided technical assistance to hospitals on selfmonitoring<br />
and auditing techniques.<br />
To help hospitals address sources of errors, several resources<br />
were developed including documentation and coding tools.<br />
This year we produced and distributed quality improvement<br />
resources designed to help hospitals reduce errors related to<br />
short stay admissions. Supporting our individual consultation,<br />
we used a variety of statewide educational efforts, ranging<br />
from our quarterly Prevention Pays newsletter, radio public<br />
service announcements, and local informational meetings<br />
throughout the state.<br />
MissouriPRO will continue to monitor payment error rates in<br />
Missouri by analyzing data from several sources including CMS<br />
and our review data. Interventions and projects will be<br />
developed and implemented on the results of our analysis.<br />
20%<br />
Remeasurement<br />
Baseline<br />
0%<br />
14<br />
Level I Level II Level III Statewide<br />
Baseline Remeasurement<br />
#2 Rehabilitation DRG (462)<br />
billed Medicare inpatient<br />
82<br />
0 20 40 60 80 100<br />
14
Consumer Protection<br />
Ensuring that the nearly 900,000<br />
Missouri Medicare consumers are<br />
aware of their rights and benefits is<br />
important to our mission. To<br />
accomplish this, we combine the<br />
strengths of our helplines, case review<br />
process, traditional education and<br />
outreach activities, and the advice<br />
and support of our Beneficiary<br />
Services/CLAIM Advisory Committee.<br />
To further supplement our beneficiary<br />
program we offer the services of<br />
CLAIM.<br />
15
Helplines<br />
For Medicare consumers help is just<br />
a phone call away. From February<br />
1, 2002, to October 31, 2002, our<br />
Medicare Helpline (1-800-347-1016)<br />
and CLAIM Program Helpline (1-800-<br />
390-3330) received over 7,000 calls.<br />
When consumers call our Medicare<br />
Helpline, staff is ready to respond to<br />
concerns regarding patient rights<br />
and quality of care.<br />
Case Review<br />
Brochures and booklets about<br />
patient rights and preventive<br />
services are mailed upon request.<br />
Assistance is offered for immediate<br />
appeals of hospital or managed<br />
care discharge letters. Also, callers<br />
concerned about the quality of care<br />
they received can file quality of care<br />
complaints. Our URAC-accredited<br />
review process ensures all concerns<br />
are addressed professionally and<br />
timely. We also review cases<br />
referred to us by fiscal intermediaries<br />
and carriers, EMTALA (anti-dumping)<br />
cases, and hospital requests for<br />
reassignment of a claim to a higherweighted<br />
DRG. Calls about issues<br />
other than these are handled by<br />
CLAIM or appropriately referred to<br />
other organizations that can provide<br />
assistance.<br />
CLAIM<br />
When consumers have specific<br />
questions about Medicare<br />
coverage, CLAIM can help. By<br />
calling CLAIM, consumers are<br />
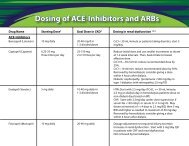
Case Review Summary 2/1/2002-10/31/2002<br />
Number<br />
Type of Review<br />
Reviewed Findings<br />
Higher weighted DRGs 878 32 requests denied<br />
PEPP reviews 605 25 admission denials<br />
10 DRG changes<br />
5 quality concerns confirmed<br />
HINNs/NODMARs 27 5 notices reversed<br />
Referrals from other agencies 36 0 DRG changes<br />
0 quality concerns confirmed<br />
0 admission denials<br />
EMTALA 59 33 five-day reviews<br />
26 sixty-day reviews<br />
Beneficiary complaints 63 20 quality concerns confirmed<br />
connected with one of over 250<br />
CLAIM volunteer counselors across<br />
the state who can answer questions<br />
about Medigap policy comparisons,<br />
Medicare benefits, Medicare Cost<br />
Savings Programs, Medicare+Choice<br />
options, long-term care insurance,<br />
appeals of denied claims, and<br />
assistance with prescription drug<br />
coverage. Thanks to our CLAIM<br />
counselors, Medicare consumers<br />
saved over $1,250,000 in out-ofpocket<br />
expenses last year and are<br />
more knowledgeable health care<br />
consumers.<br />
Outreach<br />
Phone calls alone are not relied<br />
upon to reach the Medicare<br />
consumer—we actively reach out to<br />
them before they need us. We offer<br />
a variety of traditional education<br />
and outreach efforts, ranging from<br />
our consumer newsletter, to<br />
calendars and radio PSAs, to local<br />
informational meetings throughout<br />
the state. This year we produced<br />
two consumer newsletters, presented<br />
at 98 health fairs, mailed 7,500<br />
calendars, and sponsored five radio<br />
PSAs.<br />
As Missouri’s older adult population<br />
grows and diversifies, MissouriPRO<br />
continues to turn to our Beneficiary<br />
Services/CLAIM Advisory Committee<br />
for guidance. Comprised of<br />
Medicare consumers, senior<br />
advocates, and representatives of<br />
various organizations, this committee<br />
contributes perspective on and<br />
assistance with reaching older<br />
adults. Over the next three years we<br />
will be expanding the membership<br />
of our consumer advisory committee<br />
as well as its responsibilities.<br />
Consumer Protection<br />
16
Health Care Consulting<br />
The MissouriPRO continues its dedication to<br />
assisting health care professionals deliver<br />
quality, cost-effective care through our<br />
health care consulting services. In<br />
addition to our work with health care<br />
providers under our Medicare contract,<br />
the MissouriPRO offers consulting and<br />
grants administration services to state and<br />
federal governments, non-profit and forprofit<br />
organizations.<br />
These services include expertise in program<br />
design and evaluation, data collection<br />
and analysis, quality improvement systems,<br />
medical record review and abstraction,<br />
compliance, and external reviews. The<br />
MissouriPRO was recently certified in<br />
Utilization Review Accreditation and<br />
Certification (URAC) for utilization<br />
management review.<br />
activities of our Medicare contract and of<br />
the organization as a whole. Our<br />
constituent and business development<br />
team works to develop new business<br />
opportunities and services to the health<br />
care community and to identify emerging<br />
business opportunities and trends. This<br />
includes proactively developing new<br />
business opportunities, responding to grant<br />
and contract proposals, and developing<br />
projects to be funded by private<br />
foundations.<br />
Through this work, the MissouriPRO<br />
continues to advance health care<br />
practices and policies forward by<br />
providing strategic interventions, data<br />
analysis, contract management and<br />
consultation to our partners in the health<br />
care community.<br />
Our efforts include informing our state and<br />
national elected officials and state<br />
agencies on the quality improvement<br />
17<br />
Credits<br />
Editors: Deborah Finley & Melody Kroll<br />
Design & Layout: Firehouse Design<br />
Printing: Brown Printing
MissouriPRO Board<br />
Standing (L-R):<br />
Kenneth E. Ross, DO (House Springs)<br />
Marc Smith, PhD (Jefferson City)<br />
David A. Hardy, MD, FACS (Richmond Heights)<br />
H. Jerry Murrell, MD (Columbia)<br />
Robert E. King, DO (Springfield)<br />
Carl G. Bynum, DO, MPH (Jefferson City)<br />
James T. Rogers, MD, FACP (Springfield)<br />
Jeffrey G. Copeland, MD, FACS (St. Charles)<br />
Turner L. Minnigerode, MD (Kansas City)<br />
Jerry D. Kennett, MD (Columbia)<br />
Gregg R. Laiben, MD (Kansas City)<br />
Richard A. Royer (Columbia)<br />
S. Gordon Jones, Jr., MD (Sikeston)<br />
G. Richard Hastings II (Lee’s Summit)<br />
Walter F. Davisson, MD (Chesterfield)<br />
Joseph M. Yasso, Jr., DO (Independence)<br />
Mark Aeder, MD, FACS (Kansas City)<br />
Seated (L-R):<br />
Pat Mills, MBA, CPA (Jefferson City)<br />
James D. Smith, DO (Kirksville)<br />
Janis VanMeter (Lewistown)<br />
Hazel Borders (Kansas City)<br />
Bonnie Bowles (Jefferson City)<br />
Donald J. Babb (Bolivar)<br />
MO-02-31-GEN This material was prepared by MissouriPRO under contract with the<br />
Centers for Medicare & Medicaid Services (CMS). The contents presented do not necessarily reflect CMS policy.<br />
18
3425 Constitution Court, Suite E<br />
Jefferson City, MO 65109<br />
Helplines<br />
Provider: 1-800-735-6776<br />
Beneficiary: 1-800-347-1016<br />
CLAIM: 1-800-390-3330