

BSRBR|Newsletter - The British Society for Rheumatology
BSRBR|Newsletter - The British Society for Rheumatology
BSRBR|Newsletter - The British Society for Rheumatology

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>BSRBR|Newsletter</strong><br />
Continued from page 1 . . .<br />
economic analyses. This applies to first-line use of the drugs and even more so<br />
to sequential use following the failure of a first anti-TNF.<br />
BSRBR has produced a wealth of observational data on real-life use of anti-TNF<br />
in the NHS. BSRBR patients tend to have long disease duration with<br />
well-established disease, failing on many conventional DMARDs (usually many<br />
more than the two required by NICE). As such, they may not be ideal to study<br />
efficacy. NICE health economic analyses are driven by the change in Health<br />
Assessment Questionnaire (HAQ), and in patients with established disease, this<br />
is governed by factors other than disease activity, such as damage to joints.<br />
<strong>The</strong>re<strong>for</strong>e the ability of anti-TNF to influence the HAQ in the BSRBR population<br />
is much less than in patients with a more recent onset of RA. We have used this<br />
as an argument to show that as time has gone by, rheumatologists are using<br />
biological drugs in patients with earlier disease that is proving resistant to<br />
conventional DMARDs, and where data shows that these patients will respond<br />
better than the BSRBR patients.<br />
Colleagues at the arc Epidemiology Unit in Manchester have per<strong>for</strong>med helpful<br />
analyses, sometimes at short notice with tight NICE timetables with occasional<br />
late-night telephone calls be<strong>for</strong>e Appraisal Committee meetings. With health<br />
economists in Sheffield, they have per<strong>for</strong>med analyses with change in DAS28 as<br />
the driver of the model, suggesting that anti-TNF was cost-effective in treating<br />
RA, despite the limitations of the BSRBR data. This alternative approach to a<br />
health economic analysis, as well as other evidence, was instrumental in<br />
producing sufficient doubt in the veracity of the original NICE health economic<br />
models to allow access to a first anti-TNF.<br />
University of<br />
Manchester update<br />
Cohort recruitment update<br />
BSRBR recruitment to the anti-TNF and the comparison<br />
cohort <strong>for</strong> patients with RA is complete, with an overall<br />
total of over 16,000 patients. More importantly, we are<br />
extending the follow-up and will continue to collect data<br />
from you and the UK national registers <strong>for</strong> cancer and<br />
deaths <strong>for</strong> all of these patients until at least<br />
September 2013.<br />
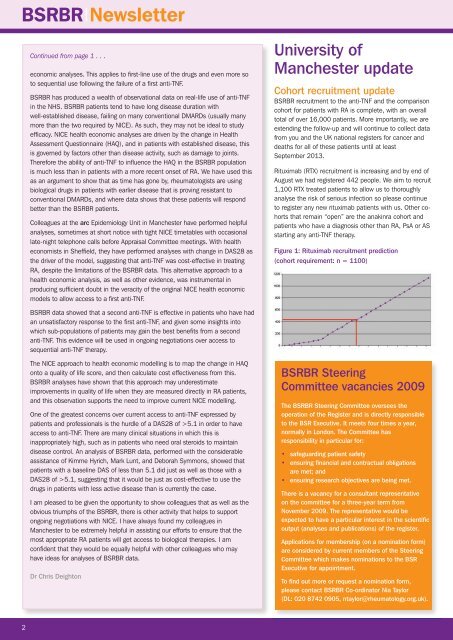
Rituximab (RTX) recruitment is increasing and by end of<br />
August we had registered 442 people. We aim to recruit<br />
1,100 RTX treated patients to allow us to thoroughly<br />
analyse the risk of serious infection so please continue<br />
to register any new rituximab patients with us. Other cohorts<br />
that remain “open” are the anakinra cohort and<br />
patients who have a diagnosis other than RA, PsA or AS<br />
starting any anti-TNF therapy.<br />
Figure 1: Rituximab recruitment prediction<br />
(cohort requirement: n = 1100)<br />
BSRBR data showed that a second anti-TNF is effective in patients who have had<br />
an unsatisfactory response to the first anti-TNF, and given some insights into<br />
which sub-populations of patients may gain the best benefits from a second<br />
anti-TNF. This evidence will be used in ongoing negotiations over access to<br />
sequential anti-TNF therapy.<br />
<strong>The</strong> NICE approach to health economic modelling is to map the change in HAQ<br />
onto a quality of life score, and then calculate cost effectiveness from this.<br />
BSRBR analyses have shown that this approach may underestimate<br />
improvements in quality of life when they are measured directly in RA patients,<br />
and this observation supports the need to improve current NICE modelling.<br />
One of the greatest concerns over current access to anti-TNF expressed by<br />
patients and professionals is the hurdle of a DAS28 of >5.1 in order to have<br />
access to anti-TNF. <strong>The</strong>re are many clinical situations in which this is<br />
inappropriately high, such as in patients who need oral steroids to maintain<br />
disease control. An analysis of BSRBR data, per<strong>for</strong>med with the considerable<br />
assistance of Kimme Hyrich, Mark Lunt, and Deborah Symmons, showed that<br />
patients with a baseline DAS of less than 5.1 did just as well as those with a<br />
DAS28 of >5.1, suggesting that it would be just as cost-effective to use the<br />
drugs in patients with less active disease than is currently the case.<br />
I am pleased to be given the opportunity to show colleagues that as well as the<br />
obvious triumphs of the BSRBR, there is other activity that helps to support<br />
ongoing negotiations with NICE. I have always found my colleagues in<br />
Manchester to be extremely helpful in assisting our ef<strong>for</strong>ts to ensure that the<br />
most appropriate RA patients will get access to biological therapies. I am<br />
confident that they would be equally helpful with other colleagues who may<br />
have ideas <strong>for</strong> analyses of BSRBR data.<br />
Dr Chris Deighton<br />
BSRBR Steering<br />
Committee vacancies 2009<br />
<strong>The</strong> BSRBR Steering Committee oversees the<br />
operation of the Register and is directly responsible<br />
to the BSR Executive. It meets four times a year,<br />
normally in London. <strong>The</strong> Committee has<br />
responsibility in particular <strong>for</strong>:<br />
• safeguarding patient safety<br />
• ensuring financial and contractual obligations<br />
are met; and<br />
• ensuring research objectives are being met.<br />
<strong>The</strong>re is a vacancy <strong>for</strong> a consultant representative<br />
on the committee <strong>for</strong> a three-year term from<br />
November 2009. <strong>The</strong> representative would be<br />
expected to have a particular interest in the scientific<br />
output (analyses and publications) of the register.<br />
Applications <strong>for</strong> membership (on a nomination <strong>for</strong>m)<br />
are considered by current members of the Steering<br />
Committee which makes nominations to the BSR<br />
Executive <strong>for</strong> appointment.<br />
To find out more or request a nomination <strong>for</strong>m,<br />
please contact BSRBR Co-ordinator Nia Taylor<br />
(DL: 020 8742 0905, ntaylor@rheumatology.org.uk).<br />
2













