

BSRBR|Newsletter - The British Society for Rheumatology
BSRBR|Newsletter - The British Society for Rheumatology
BSRBR|Newsletter - The British Society for Rheumatology

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>BSRBR|Newsletter</strong><br />
<strong>The</strong> <strong>British</strong> <strong>Society</strong> <strong>for</strong><br />
<strong>Rheumatology</strong><br />
Biologics Register<br />
<strong>The</strong> Newsletter of the <strong>British</strong> <strong>Society</strong> <strong>for</strong> <strong>Rheumatology</strong> Biologics Register<br />
October 2009<br />
Editorial<br />
Report on the BSR Biologics<br />
Register Committee<br />
I am happy to confirm that a major step in the direction of establishing an<br />
ankylosing spondylitis register has been achieved in line with Professor Barry<br />
Bresnihan’s proposal that BSRBR should expand to include an assessment of the<br />
effects of biological agents in other diseases. With help from National Ankylosing<br />
Spondylitis <strong>Society</strong> (NASS), the pharmaceutical company Wyeth and funds from<br />
BSR itself, a sum of £30,000 has been raised. This enabled us to appoint<br />
Dr Lorna Layward to the role of Register Development Officer.<br />
<strong>The</strong> main elements of Lorna’s role will be to:<br />
• seek an agreement about the principle questions that an<br />
ankylosing spondylitis register would seek to answer;<br />
• develop the tendering process <strong>for</strong> a centre to run the<br />
register;<br />
• approach the clinical trials network to obtain prior support<br />
<strong>for</strong> this register on the basis of the clinical questions being<br />
addressed; and finally (and rather importantly!)<br />
• engage the pharmaceutical industry and any other parties<br />
who might be interested in actually funding such a register<br />
<strong>for</strong> a minimum of five years.<br />
If you would like to input your views on any of these issues in setting up the AS register<br />
please email Lorna on: llayward@rheumatology.org.uk<br />
I would also like to take this opportunity of thanking Barry <strong>for</strong> the huge amount of work<br />
he put in to his assessment of the register, un<strong>for</strong>tunately Barry has fallen ill and we<br />
would there<strong>for</strong>e like to wish him the very best.<br />
David A Isenberg MD FRCP, ARC Diamond Jubilee Professor of<br />
<strong>Rheumatology</strong> at University College London<br />
Working with the arc<br />
Epidemiology unit in Manchester<br />
BSRBR has been a tremendous success, quite rightly described by<br />
David Isenberg as the “jewel in the crown of BSR”. <strong>The</strong> triumphs are well<br />
publicised in a host of highly in<strong>for</strong>mative papers published in the world’s<br />
leading rheumatology journals. However, people may not be aware that the<br />
BSRBR’s wealth of data can be accessed by all. Here Dr Chris Deighton<br />
explains how, with the help of the arc Epidemiology Unit in Manchester,<br />
analysis from the BSRBR has helped in negotiations with NICE.<br />
We all express concerns about current NICE restrictions on access to anti-TNF<br />
<strong>for</strong> RA patients, but without the help of BSRBR we would not even have the<br />
current availability of these drugs in the NHS. Let me share with you some of the<br />
help that Manchester unit have provided <strong>for</strong> those of us who negotiate with NICE<br />
both in the past and in ongoing appraisals.<br />
From the first negotiations with NICE on access to anti-TNF <strong>for</strong> RA, we struggled<br />
to demonstrate that these drugs are cost-effective according to NICE health<br />
Continues on page 2 . . .<br />
BSR Biologics<br />
Register and<br />
what is does<br />
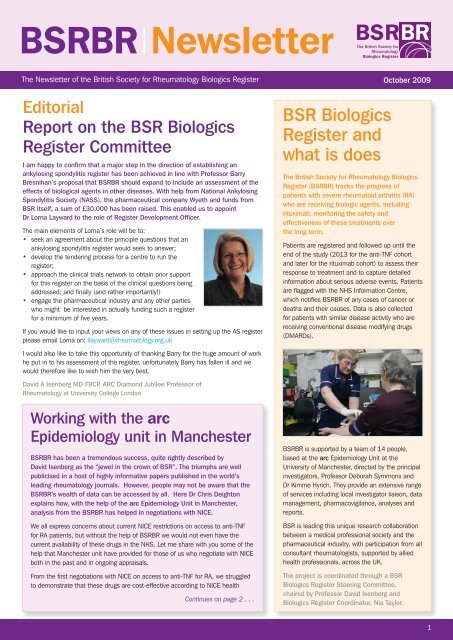
<strong>The</strong> <strong>British</strong> <strong>Society</strong> <strong>for</strong> <strong>Rheumatology</strong> Biologics<br />
Register (BSRBR) tracks the progress of<br />
patients with severe rheumatoid arthritis (RA)<br />
who are receiving biologic agents, including<br />
rituximab, monitoring the safety and<br />
effectiveness of these treatments over<br />
the long term.<br />
Patients are registered and followed up until the<br />
end of the study (2013 <strong>for</strong> the anti-TNF cohort<br />
and later <strong>for</strong> the rituximab cohort) to assess their<br />
response to treatment and to capture detailed<br />
in<strong>for</strong>mation about serious adverse events. Patients<br />
are flagged with the NHS In<strong>for</strong>mation Centre,<br />
which notifies BSRBR of any cases of cancer or<br />
deaths and their causes. Data is also collected<br />
<strong>for</strong> patients with similar disease activity who are<br />
receiving conventional disease modifying drugs<br />
(DMARDs).<br />
BSRBR is supported by a team of 14 people,<br />
based at the arc Epidemiology Unit at the<br />
University of Manchester, directed by the principal<br />
investigators, Professor Deborah Symmons and<br />
Dr Kimme Hyrich. <strong>The</strong>y provide an extensive range<br />
of services including local investigator liaison, data<br />
management, pharmacovigilance, analyses and<br />
reports.<br />
BSR is leading this unique research collaboration<br />
between a medical professional society and the<br />
pharmaceutical industry, with participation from all<br />
consultant rheumatologists, supported by allied<br />
health professionals, across the UK.<br />
<strong>The</strong> project is coordinated through a BSR<br />
Biologics Register Steering Committee,<br />
chaired by Professor David Isenberg and<br />
Biologics Register Coordinator, Nia Taylor.<br />
1
<strong>BSRBR|Newsletter</strong><br />
Continued from page 1 . . .<br />
economic analyses. This applies to first-line use of the drugs and even more so<br />
to sequential use following the failure of a first anti-TNF.<br />
BSRBR has produced a wealth of observational data on real-life use of anti-TNF<br />
in the NHS. BSRBR patients tend to have long disease duration with<br />
well-established disease, failing on many conventional DMARDs (usually many<br />
more than the two required by NICE). As such, they may not be ideal to study<br />
efficacy. NICE health economic analyses are driven by the change in Health<br />
Assessment Questionnaire (HAQ), and in patients with established disease, this<br />
is governed by factors other than disease activity, such as damage to joints.<br />
<strong>The</strong>re<strong>for</strong>e the ability of anti-TNF to influence the HAQ in the BSRBR population<br />
is much less than in patients with a more recent onset of RA. We have used this<br />
as an argument to show that as time has gone by, rheumatologists are using<br />
biological drugs in patients with earlier disease that is proving resistant to<br />
conventional DMARDs, and where data shows that these patients will respond<br />
better than the BSRBR patients.<br />
Colleagues at the arc Epidemiology Unit in Manchester have per<strong>for</strong>med helpful<br />
analyses, sometimes at short notice with tight NICE timetables with occasional<br />
late-night telephone calls be<strong>for</strong>e Appraisal Committee meetings. With health<br />
economists in Sheffield, they have per<strong>for</strong>med analyses with change in DAS28 as<br />
the driver of the model, suggesting that anti-TNF was cost-effective in treating<br />
RA, despite the limitations of the BSRBR data. This alternative approach to a<br />
health economic analysis, as well as other evidence, was instrumental in<br />
producing sufficient doubt in the veracity of the original NICE health economic<br />
models to allow access to a first anti-TNF.<br />
University of<br />
Manchester update<br />
Cohort recruitment update<br />
BSRBR recruitment to the anti-TNF and the comparison<br />
cohort <strong>for</strong> patients with RA is complete, with an overall<br />
total of over 16,000 patients. More importantly, we are<br />
extending the follow-up and will continue to collect data<br />
from you and the UK national registers <strong>for</strong> cancer and<br />
deaths <strong>for</strong> all of these patients until at least<br />
September 2013.<br />
Rituximab (RTX) recruitment is increasing and by end of<br />
August we had registered 442 people. We aim to recruit<br />
1,100 RTX treated patients to allow us to thoroughly<br />
analyse the risk of serious infection so please continue<br />
to register any new rituximab patients with us. Other cohorts<br />
that remain “open” are the anakinra cohort and<br />
patients who have a diagnosis other than RA, PsA or AS<br />
starting any anti-TNF therapy.<br />
Figure 1: Rituximab recruitment prediction<br />
(cohort requirement: n = 1100)<br />
BSRBR data showed that a second anti-TNF is effective in patients who have had<br />
an unsatisfactory response to the first anti-TNF, and given some insights into<br />
which sub-populations of patients may gain the best benefits from a second<br />
anti-TNF. This evidence will be used in ongoing negotiations over access to<br />
sequential anti-TNF therapy.<br />
<strong>The</strong> NICE approach to health economic modelling is to map the change in HAQ<br />
onto a quality of life score, and then calculate cost effectiveness from this.<br />
BSRBR analyses have shown that this approach may underestimate<br />
improvements in quality of life when they are measured directly in RA patients,<br />
and this observation supports the need to improve current NICE modelling.<br />
One of the greatest concerns over current access to anti-TNF expressed by<br />
patients and professionals is the hurdle of a DAS28 of >5.1 in order to have<br />
access to anti-TNF. <strong>The</strong>re are many clinical situations in which this is<br />
inappropriately high, such as in patients who need oral steroids to maintain<br />
disease control. An analysis of BSRBR data, per<strong>for</strong>med with the considerable<br />
assistance of Kimme Hyrich, Mark Lunt, and Deborah Symmons, showed that<br />
patients with a baseline DAS of less than 5.1 did just as well as those with a<br />
DAS28 of >5.1, suggesting that it would be just as cost-effective to use the<br />
drugs in patients with less active disease than is currently the case.<br />
I am pleased to be given the opportunity to show colleagues that as well as the<br />
obvious triumphs of the BSRBR, there is other activity that helps to support<br />
ongoing negotiations with NICE. I have always found my colleagues in<br />
Manchester to be extremely helpful in assisting our ef<strong>for</strong>ts to ensure that the<br />
most appropriate RA patients will get access to biological therapies. I am<br />
confident that they would be equally helpful with other colleagues who may<br />
have ideas <strong>for</strong> analyses of BSRBR data.<br />
Dr Chris Deighton<br />
BSRBR Steering<br />
Committee vacancies 2009<br />
<strong>The</strong> BSRBR Steering Committee oversees the<br />
operation of the Register and is directly responsible<br />
to the BSR Executive. It meets four times a year,<br />
normally in London. <strong>The</strong> Committee has<br />
responsibility in particular <strong>for</strong>:<br />
• safeguarding patient safety<br />
• ensuring financial and contractual obligations<br />
are met; and<br />
• ensuring research objectives are being met.<br />
<strong>The</strong>re is a vacancy <strong>for</strong> a consultant representative<br />
on the committee <strong>for</strong> a three-year term from<br />
November 2009. <strong>The</strong> representative would be<br />
expected to have a particular interest in the scientific<br />
output (analyses and publications) of the register.<br />
Applications <strong>for</strong> membership (on a nomination <strong>for</strong>m)<br />
are considered by current members of the Steering<br />
Committee which makes nominations to the BSR<br />
Executive <strong>for</strong> appointment.<br />
To find out more or request a nomination <strong>for</strong>m,<br />
please contact BSRBR Co-ordinator Nia Taylor<br />
(DL: 020 8742 0905, ntaylor@rheumatology.org.uk).<br />
2
<strong>BSRBR|Newsletter</strong><br />
www.rheumatology.org.uk<br />
Conference report<br />
BSRBR at <strong>Rheumatology</strong> ‘09<br />
<strong>The</strong> BSRBR was well-represented at BSR’s conference at Glasgow’s SECC in April<br />
this year. <strong>The</strong> conference attracted around 2,200 attendees over four days and<br />
feedback from the online evaluation survey was very positive; 95% said they would<br />
recommend the conference to a colleague, 81% said that the conference is a key<br />
date in their professional calendar and 91% said that they learnt new things at<br />
the conference.<br />
<strong>The</strong>re was a BSRBR stand which was manned by staff from the University of<br />
Manchester Register team, Pauline Whitelaw and Nia Taylor.<br />
Seven abstracts from the BSRBR were presented: one oral presentation and six posters.<br />
<strong>The</strong> usual lunchtime open BSRBR session was held on the Wednesday of the<br />
conference. This session attracted a record 300 delegates, so that the packed<br />
lunches ran out and more had to be ordered!<br />
Principal Investigators, Professor Deborah Symmons and Dr Kimme Hyrich, gave an<br />
update on the BSRBR, including rituximab recruitment, adverse event data and<br />
extended follow-up; Dr Andrew Keat presented the plans <strong>for</strong> developing a new register<br />
<strong>for</strong> ankylosing spondylitis; Debbie Smith gave a round up of the latest news on the<br />
NICE appraisal of TNF alpha drug switching and Professors David Isenberg and<br />
Barry Bresnihan talked about the way <strong>for</strong>ward <strong>for</strong> the BSRBR, including collaboration<br />
with other European Registries and electronic data capture.<br />
BSR’s events team have recognized the popularity of the BSRBR’s lunch time meeting<br />
and, concerned that attendance might be restricted in 2010, when conference will only<br />
run over three days, they have included the BSRBR session in the main programme.<br />
This means that it will benefit from advertising in the main programme from<br />
September and the session will last <strong>for</strong> an hour and a half instead of 60 minutes.<br />
So put the dates in your diary: the conference will be held at the<br />
ICC Birmingham between 21–23 April 2010 and the BSRBR session will be on<br />
Thursday 23 April 2010 from 13.30 to 15.00 hours.<br />
UK CRN<br />
We are delighted to in<strong>for</strong>m you that BSRBR has<br />
finally been accepted on the portfolio. Our UK<br />
CRN ID number is 7302. Over the next few months<br />
we will be uploading all the accrual data <strong>for</strong><br />
2008/2009, which will be co-ordinated centrally<br />
from the BSRBR office. In addition, we will provide<br />
figures of registrations prior to 2008 to the<br />
portfolio. If you have any immediate questions<br />
regarding this, please do not hesitate to contact<br />
the office – biologics.register@manchester.ac.uk.<br />
We will be in contact with you soon regarding your<br />
accrual data to date.<br />
➜<br />
Change of contact<br />
Pauline Whitelaw is currently taking six months<br />
unpaid leave from her post as Policy and<br />
Projects Administrator, returning early February.<br />
In her absence please contact Katie Fitzgerald<br />
at kfitzgerald@rheumatology.org.uk<br />
BSR members’ survey results<br />
<strong>The</strong> most recent membership survey carried out by BSR in May 2009<br />
asked members <strong>for</strong> their views on BSR’s new aims and strategic plan.<br />
Two questions about the <strong>Society</strong>’s activities were included. As contributors<br />
to the BSRBR, you will no doubt be pleased to know that the Register<br />
scored very highly in both questions.<br />
• 46% rated the Register as ‘very important’ – the highest proportion<br />
<strong>for</strong> any activity.<br />
• <strong>The</strong> average rating of the Register was third highest of the 16<br />
activities listed, behind Clinical Guidelines and Annual Scientific<br />
Conference<br />
• 51% of responders rated BSR’s per<strong>for</strong>mance in relation to the<br />
Register as ‘very good’ (5 on scale of 1 to 5)<br />
• <strong>The</strong> only activity which scored a higher percentage of ‘very good’<br />
was Clinical Guidelines<br />
• <strong>The</strong> average rating of the Register was the highest of the 16<br />
activities listed, above that of the Annual Scientific conference,<br />
<strong>Rheumatology</strong> Journal and Clinical Guidelines (the next three<br />
highest ratings)<br />
3
ABSTRACTS|presented at the BSR AGM 2009<br />
FACTORS ASSOCIATED WITH WORK DISABILITY IN RHEUMATOID ARTHRITIS<br />
PATIENTS: RESULTS FROM THE BSR BIOLOGICS REGISTER (BSRBR)<br />
SMM Verstappen, KD Watson, K McGrother, DPM Symmons, KL Hyrich, on behalf of<br />
the BSR Biologics Register, arc Epidemiology Unit, <strong>The</strong> University of Manchester,<br />
Manchester, United Kingdom.<br />
Background: Work disability is one of the major economic problems in patients with<br />
rheumatoid arthritis (RA). Treatment with anti-TNF agents has proven to be clinically<br />
effective in these patients, but there is limited data available on the effect of biological<br />
agents on working status in the UK.<br />
Aim: Using data from BSRBR, (i) to describe working status at start of anti-TNF<br />
treatment, and (ii) to identify predictors of onset of new work disability.<br />
Methods: 2,703 consecutive patients with RA registered with the BSRBR between<br />
01/10/2001 and 01/09/2008 (aged3.2 to 5.1) disease activity.<br />
Methods: Patients <strong>for</strong> this study were selected from the BSR Biologics Register if they<br />
had failed treatment with at least 2 standard DMARDs and fell into the moderate or<br />
high DAS28 categories. Change in HAQ over the first 12 months of enrolment were<br />
compared first between anti-TNF treated and untreated patients in each DAS group,<br />
and then between treated patients in the moderate and high DAS groups. Mean<br />
change in HAQ was modelled <strong>for</strong> each comparison using Doubly Robust estimation,<br />
which fits both a propensity and a linear regression model to minimise bias in the<br />
estimate. Results were adjusted <strong>for</strong> age, gender, disease duration, baseline HAQ and<br />
DAS28 score, number of previous DMARDS and steroid use.<br />
Results: <strong>The</strong> analysis included 4772 and 224 anti-TNF treated and 369 and 325<br />
DMARD only treated patients with high and moderate DAS28 respectively, despite 2<br />
DMARDs. In both DAS28 groups, anti-TNF treated patients tended towards lower age<br />
and higher mean DAS28 and HAQ scores at baseline, but had similar disease<br />
duration. <strong>The</strong>y had also failed on average one more DMARD than the untreated group<br />
(4 versus 3, p5.1.<br />
<strong>The</strong> current UK eligibility criteria <strong>for</strong> anti-TNF therapy, which limits therapy to patients<br />
with DAS28>5.1 should be reconsidered, as substantial functional (and there<strong>for</strong>e<br />
cost-effective) benefits may also be gained by treating those with moderately active<br />
disease.<br />
Baseline DAS28 > 3.2 – 5.1 > 5.1<br />
Treatment Group DMARD Anti-TNF DMARD Anti-TNF<br />
(325) (224) (369) (4772)<br />
HAQ baseline (mean (SD)) 1.43 1.78 1.87 2.06<br />
(0.75) (0.61) (0.62) (0.55)<br />
HAQ 12 months (mean (SD)) 1.45 1.51 1.86 1.71<br />
(0.78) (0.75) (0.63 (0.71)<br />
Mean change in HAQ (95% CI) 0.02 -0.27 -0.01 -0.35<br />
(-0.07, 0.1) (-0.4, -0.15) (-0.09, 0.07) (-0.38, -0.32)<br />
Adjusted Mean Change in HAQ ref -0.24 ref -0.28<br />
(95% CI) (-0.33, -0.14) (-0.34, -0.23)<br />
Adjusted Mean Change in HAQ ref -0.05<br />
(95% CI) (-0.16, 0.06)<br />
SECULAR CHANGES IN UK ANTI-TNF PRESCRIBING PATTERNS AND TREATMENT<br />
RESPONSE IN PATIENTS WITH RHEUMATOID ARTHRITIS: RESULTS FROM THE<br />
BSRBR<br />
Kath Watson 1 , Kimme Hyrich 1 , Mark Lunt 1 , Deborah Symmons 1 , on behalf of the<br />
BSRBR 1<br />
1<br />
. arc Epidemiology Unit, <strong>The</strong> University of Manchester, Manchester, United Kingdom.<br />
Anti-TNF therapy <strong>for</strong> rheumatoid arthritis (RA) has significantly improved outcomes<br />
<strong>for</strong> patients with severe disease. In the UK, changes in financial restrictions and<br />
increasing experience with their use may have resulted in changes to the way<br />
clinicians use anti-TNF therapies. <strong>The</strong> aim of this analysis was to study the trends in<br />
prescribing patterns of anti-TNF therapies by UK rheumatologists over a 7 year period<br />
and compare this with changes in response to treatment. Between October 2001 and<br />
June 2007, 10789 patients with RA were registered with the BSRBR. Baseline<br />
characteristics were analysed according to year of anti-TNF prescription. Only the first<br />
course of anti-TNF was included. Treatment response was determined at 6 months<br />
according to EULAR criteria. Changes in baseline disease characteristics and response<br />
rates over a seven year period were analysed using univariate linear and logistic<br />
regression analysis methods. Over these 7 years, the median level of disease activity<br />
and severity of newly treated anti-TNF patients has significantly decreased (p
www.rheumatology.org.uk<br />
(see Table). <strong>The</strong> median disease duration remained high (9 years in 2007) although<br />
the proportion of patient with disease 5.1 following failure of ≥2<br />
DMARDs including methotrexate) (n=766) followed <strong>for</strong> 6 months. Patients completed<br />
the EQ-5D, SF-36 and HAQ at baseline and at a 6-month follow-up assessment.<br />
Predicted EQ-5D scores were estimated using the HAQ (1) or the SF-36 (2) . <strong>The</strong> mean<br />
difference between predicted and observed EQ-5D scores at baseline and change<br />
during the study was tested using the t-test.<br />
Results: <strong>The</strong> patients recruited to this study had a mean age of 58, disease duration<br />
of 12 years and predominance of females (Table). HAQ and SF-36 physical<br />
component summary score (PCS) indicated considerable physical disability, and the<br />
patients had low HRQoL scores. Predicted EQ-5D scores were higher than observed<br />
scores at baseline, although this was only significant where estimated using the HAQ<br />
(p=0.007). Over 6 months of follow-up patients improved in physical function and<br />
HRQoL, with change exceeding the minimum important difference (MID) <strong>for</strong> the HAQ<br />
(MID 0.20), EQ-5D (MID 0.05-0.07), PCS (MID 2-3) and mental component<br />
summary scores (MCS) (MID 3). Change in predicted EQ-5D scores (both methods)<br />
also exceeded the MID, and corresponded well with observed EQ-5D scores. Although<br />
change in EQ-5D appeared to be underestimated when predicted from HAQ scores<br />
and overestimated when predicted from the SF-36, neither were significantly different.<br />
Age Mean (SD) 58.3 (12.2)<br />
Gender N (%) 583 (76%)<br />
Disease duration Mean (SD) 11.8 (10.9)<br />
Baseline<br />
6-month change<br />
n=766 n=699<br />
HAQ Mean (SD) 1.72 (0.71) -0.22 (0.54)<br />
SF-36 PCS Mean (SD) 20.4 (10.8) 4.6 (10.3)<br />
SF-36 MCS Mean (SD) 45.0 (11.3) 3.0 (11.4)<br />
EQ-5D Observed 0.40 (0.33) 0.08 (0.32)<br />
Predicted (using HAQ) 0.44 (0.26) 0.07 (0.24)<br />
Difference, mean (95% CI) 0.04 (0.01, 0.07) -0.02 (-0.05, 0.01)<br />
Observed 0.40 (0.33) 0.08 (0.32)<br />
Predicted (using SF-36) 0.42 (0.25) 0.10 (0.23)<br />
Difference, mean (95% CI) 0.02 (-0.01, 0.05) 0.02 (-0.01, 0.05)<br />
Conclusions: Predicted EQ-5D scores from the HAQ and the SF-36 were reasonable<br />
estimates of mean baseline and change EQ-5D scores in the RA patients with severe<br />
disease. However small differences in response to change could have implications in<br />
assessing the cost-effectiveness of treatments; underestimation of change (e.g.<br />
EQ-5D estimated from the HAQ) may lead to underestimation of cost-effectiveness,<br />
whilst over-estimation (e.g. SF-36 to EQ-5D) may overestimate cost-effectiveness.<br />
For this reason, estimating EQ-5D scores may be valid where no alternative exists or<br />
<strong>for</strong> sensitivity analyses, however we recommend that prospective studies should<br />
include at least one measure of HRQoL which allows the estimation of utilities.<br />
References (1) Bansback N, Marra C, et al. Arthritis Rheum 2007; 57:963-71. (2)<br />
Ara R & Brazier J. Value in Health 2008; 1131-43<br />
THE INFLUENCE OF ANTI-TNF THERAPY UPON CANCER INCIDENCE IN PATIENTS<br />
WITH RHEUMATOID ARTHRITIS (RA) WHO HAVE HAD PRIOR MALIGNANCY:<br />
RESULTS FROM THE BSRBR<br />
WG Dixon, KD Watson, M Lunt, BSRBR Control Centre Consortium, KL Hyrich, DPM<br />
Symmons, on behalf of the BSR Biologics Register.<br />
Purpose: Anti-TNF therapy is rarely prescribed to patients with a history of prior<br />
malignancy following theoretical safety concerns, clinical trial exclusion criteria and<br />
national guidelines. Thus, there is currently no published evidence regarding the safety<br />
of anti-TNF therapy in patients with prior malignancy. Our aim was to explore the<br />
influence of anti-TNF therapy upon the incidence of cancer in patients with prior<br />
malignancy, using data from a large national register.<br />
Methods: 10735 consecutive anti-TNF treated patients with RA registered with the<br />
BSRBR were followed prospectively. <strong>The</strong>y were compared to 3236 patients with active<br />
RA on disease modifying anti-rheumatic drugs (DMARD). Patients with a malignancy<br />
prior to registration were identified by record linkage with the UK Office <strong>for</strong> National<br />
Statistics (ONS). Further analysis was restricted to these patients. Incident<br />
malignancies up to 30/9/07 were identified from consultant and patient<br />
questionnaires and ONS. Local recurrence and metastases were included as incident<br />
cancers. Carcinoma-in-situ and non-melanoma skin cancers were excluded from both<br />
prior and incident malignancies. Patients contributed follow-up time until 30/9/07 or<br />
death, whichever came first. An individual patient could contribute >1 incident<br />
malignancy. Incidence rate ratios (IRR) were calculated comparing the anti-TNF to<br />
the DMARD-treated cohorts. Results: 177 (1.6%) anti-TNF and 118 (3.6%)<br />
DMARD-treated patients had a history of prior malignancy. Registration occurred within<br />
10 years of the prior malignancy in 75 (42%) of the anti-TNF and 71 (60%) of the<br />
DMARD treated patients. After median follow-up times of 3.06 and 1.93 years in the<br />
anti-TNF and DMARD-treated cohorts, there were 13 incident cancers in 11/177 (6%)<br />
anti-TNF treated patients compared to 10 cancers in 10/118 (8%) DMARD-treated<br />
patients. <strong>The</strong> crude rate of incident cancers was lower in the anti-TNF cohort (25.3<br />
events / 1000 person years (pyrs) (95% CI 13.4, 43.2)) compared to the DMARD<br />
cohort (41.9 / 1000 pyrs (20.1, 77.1)). <strong>The</strong> age- and sex-adjusted IRR <strong>for</strong> anti-TNF vs<br />
DMARD-treated patients with prior malignancy was 0.53 (0.22-1.26). 17 patients in<br />
the anti-TNF cohort had prior melanomas compared to 10 in the DMARD cohort. Of<br />
concern, 3/11 anti-TNF patients with prior then incident malignancy had prior<br />
melanomas. <strong>The</strong> time from melanoma to starting anti-TNF therapy was 33%) of patients with ankylosing spondylitis (AS) need to give up work<br />
be<strong>for</strong>e normal retirement. <strong>The</strong> beneficial clinical effects of anti-TNF therapy seen in<br />
patients with AS hopefully will lead to less work disability in the future.<br />
Aim: To describe working status at start of anti-TNF treatment and at three years after<br />
starting anti-TNF therapy.<br />
Methods. 229 consecutive patients with AS (aged
<strong>BSRBR|Newsletter</strong><br />
Presentation of latest<br />
results: ACR, Philadelphia,<br />
October 2009<br />
We have had two new analyses accepted <strong>for</strong> oral<br />
presentation at the ACR in Philadelphia this year<br />
and one poster:<br />
Wednesday 21st October 11 – 12:30pm<br />
Session: RA Clinical Aspects Treatment Outcomes<br />
Presentation 1: <strong>The</strong> influence of anti-TNF therapy<br />
upon incidence of non-melanoma skin cancer<br />
(NMSC) in patients with rheumatoid arthritis (RA):<br />
Results from the BSR Biologics Register (BSRBR)<br />
Presentation 2: Risk of septic arthritis in patients<br />
with rheumatoid arthritis treated with anti-TNF<br />
therapy: results from the BSR Biologics Register<br />
(BSRBR)<br />
Tuesday 20th October<br />
Poster: Serious infections in patients with<br />
Rheumatoid Arthritis (RA) treated with anakinra<br />
(ANA): Experience from the BSR Biologics Register<br />
(BSRBR)<br />
Web-based<br />
data collection<br />
We are starting to plan <strong>for</strong> a web-based data<br />
collection system <strong>for</strong> those of you who would<br />
prefer to enter data directly onto a website<br />
(<strong>for</strong> submission to the Register database)<br />
rather than completing and sending<br />
paper-based questionnaires.<br />
Our aim is to create the web entry <strong>for</strong>ms in<br />
such a way that:<br />
• it is quicker <strong>for</strong> you to complete them than<br />
filling in paper <strong>for</strong>ms (use of drop-down<br />
lists etc)<br />
• data is checked as entered, thus reducing<br />
need to correct errors by the team at<br />
Manchester.<br />
We will soon be sending a short survey to those<br />
of you responsible <strong>for</strong> sending data, to find out<br />
how easy you would find it to switch to<br />
electronic data entry. We also hope to identify<br />
some sites willing to be the “guinea pigs” <strong>for</strong><br />
this new system.<br />
If you are interested in discussing this, please<br />
contact Kath Watson at<br />
kath.watson@manchester.ac.uk or Nia Taylor at<br />
ntaylor@rheumatology.org.uk.<br />
Recent Publications<br />
For a full list of BSRBR publications list please visit the<br />
“Health Professionals” area of our website<br />
(www.manchester.ac.uk/medicine/arc/BSRBR)<br />
and click on “Publications”.<br />
Saad AA, Ashcroft DM, Watson KD, Hyrich KL, Noyce PR, Symmons DP;<br />
<strong>British</strong> <strong>Society</strong> <strong>for</strong> <strong>Rheumatology</strong> Biologics Register. Persistence with<br />
anti-tumour necrosis factor therapies in patients with psoriatic arthritis:<br />
observational study from the <strong>British</strong> <strong>Society</strong> <strong>for</strong> <strong>Rheumatology</strong> Biologics<br />
Register. Arthritis Res <strong>The</strong>r. 2009; 11(2):R52. Epub 2009 Apr 8.<br />
Harrison MJ, Dixon WG, Watson KD, King Y, Groves R, BSRBR Control<br />
Centre Consortium, Hyrich KL, Symmons DP on behalf of the BSRBR.<br />
Rates of new-onset psoriasis in patients with rheumatoid arthritis receiving<br />
anti-tumour necrosis factor alpha therapy: results from the BSRBR.<br />
Ann Rheum Dis. 2009 Feb; 68(2):209-15.<br />
Lunt M, Solomon D, Rothman K, Glynn R, Hyrich K, <strong>The</strong> BSRBR Control<br />
Centre Consortium, BSRBR, Symmons DP, Stürmer T. Different Methods of<br />
Balancing Covariates Leading to Different Effect Estimates in the Presence<br />
of Effect Modification. Am J Epidem. 2009 Jan 19. [Epub ahead of print]<br />
Hyrich KL, Lunt. M, Dixon WG, Watson KD, Symmons. DPM, BSRBR.<br />
Effects of switching between anti-TNF therapies on HAQ response in<br />
patients who do not respond to their first anti-TNF drug. Results from the<br />
national <strong>British</strong> <strong>Society</strong> <strong>for</strong> <strong>Rheumatology</strong> Biologics Register (BSRBR).<br />
<strong>Rheumatology</strong> (Ox<strong>for</strong>d). 2008 Jul; 47(7):1000-5.<br />
Hyrich KL, Watson KD, Isenberg DA, Symmons DP. <strong>The</strong> <strong>British</strong> <strong>Society</strong><br />
<strong>for</strong> <strong>Rheumatology</strong> Biologics Register: 6 years on. <strong>Rheumatology</strong> (Ox<strong>for</strong>d).<br />
2008 Oct; 47(10):1441-3.<br />
All BSRBR follow-up extended to 2013<br />
As already mentioned, we have<br />
extended the follow-up of all patients<br />
in the BSRBR to 2013. This means<br />
that annual follow-ups will be sent out<br />
after five years of follow-up asking<br />
about any changes in therapy and any<br />
serious adverse events that have<br />
occurred in the past year. <strong>The</strong>re<strong>for</strong>e<br />
we are only interested in those events<br />
that fulfil our definition of serious and<br />
those non serious adverse events that<br />
led to discontinuation of a drug<br />
(see table).<br />
Website suggestions?<br />
Please send suggestions <strong>for</strong> improvements/in<strong>for</strong>mation you would<br />
like to be able to access on the BSRBR website to<br />
pat.creighton@manchester.ac.uk.<br />
Definition of serious adverse events<br />
1. Death<br />
2. Hospitalisation<br />
3. IV antibiotics<br />
4. Significant loss of function<br />
5. Congenital mal<strong>for</strong>mation<br />
6. Life threatening<br />
Please also record all events that<br />
led to a drug discontinuation.<br />
6
<strong>BSRBR|Newsletter</strong><br />
www.rheumatology.org.uk<br />
Events of Special<br />
Interest <strong>for</strong>ms reminder<br />
We urge you to download our new “Events of Special<br />
Interest” <strong>for</strong>ms from our website<br />
www.manchester.ac.uk/medicine/arc/BSRBR under<br />
the “Health Professionals” section. This is so you<br />
can complete these <strong>for</strong>ms at the same time as you<br />
initially report one of these events to us on the<br />
follow-up <strong>for</strong>m. This means that we will not have to<br />
bother you <strong>for</strong> more in<strong>for</strong>mation on the event at a<br />
later date and will save you having to access the<br />
case notes again. <strong>The</strong> following events are those<br />
<strong>for</strong> which we need to have one of these <strong>for</strong>ms<br />
completed:<br />
• Aplastic anaemia<br />
• Central demyelination<br />
• Congestive heart failure<br />
• Infusion/immunologic reactions (rituximab only)<br />
• Lymphoproliferative tumour<br />
• Myocardial infarction<br />
• Pregnancy<br />
• Pulmonary embolism<br />
• Serious infections<br />
• Stroke<br />
• Surgery<br />
• Tuberculosis<br />
If not received with the follow-up <strong>for</strong>m, we will<br />
post the <strong>for</strong>m out to you to enable us to collect<br />
this in<strong>for</strong>mation.<br />
BSRBR Events of Special Interest Forms<br />
NICE update<br />
Multiple Technology Appraisals<br />
Rheumatoid arthritis – drugs <strong>for</strong> treatment after failure of a TNF inhibitor<br />
BSR submitted evidence on 10 August 2009 based on the final scope of<br />
this appraisal. <strong>The</strong> submission consisted of two papers: one from the arc<br />
epidemiology unit at Manchester with the latest evidence from the Biologics<br />
Register and one from the BSR Clinical Affairs Committee based on the<br />
revised BSR Biologics Guidelines. <strong>The</strong> appraisal was re-started in November<br />
2008, following the NICE Appeal Committee’s recommendation that NICE<br />
reconsider the issue of allowing patients prescription of an alternative<br />
anti-TNF if their first anti-TNF does not work satisfactorily. <strong>The</strong> first appraisal<br />
committee meeting will take place on 4 February 2010.<br />
Psoriatic arthritis - etanercept, infliximab and adalimumab (review)<br />
BSR submitted comments on the final scope on 26 August 2009.<br />
Single Technology Appraisals<br />
Abatacept - Juvenile idiopathic arthritis<br />
NICE in<strong>for</strong>med us that this technology appraisal had been suspended, as<br />
the manufacturer of Abatacept was not in a position to submit evidence<br />
due to a delay in the regulatory process. We will keep you updated on any<br />
developments.<br />
Certolizumab<br />
BSR submitted an organisational statement <strong>for</strong> this appraisal in June 2009.<br />
<strong>The</strong> first appraisal committee meeting took place on 23 September 2009,<br />
with the guidance expected to be issued in February 2010.<br />
Golimumab<br />
<strong>The</strong> three appraisals on Golimumab (<strong>for</strong> the treatment of rheumatoid arthritis<br />
after failure of previous antirheumatic drugs, <strong>for</strong> the treatment of rheumatoid<br />
arthritis (methotrexate-naïve) and <strong>for</strong> the treatment of ankylosing spondylitis)<br />
have all been suspended at the request of the manufacturer, as they were<br />
not in a position to submit evidence. We will keep you updated on any<br />
developments.<br />
Tocilizumab<br />
NICE Appraisal Committee’s preliminary recommendation (1st October)<br />
is that Tocilizumab is not recommended <strong>for</strong> the treatment of moderate to<br />
severe active rheumatoid arthritis. <strong>The</strong>se recommendations are under<br />
consultation and the deadline <strong>for</strong> comments is 22nd October 2009.<br />
Clinical guideline updates<br />
Tuberculosis - update of clinical guidelines<br />
BSR is participating in the revision of these guidelines, and took part in the<br />
stakeholder workshop held on 29 September 2009.<br />
7
<strong>BSRBR|Newsletter</strong><br />
Outstanding Death Data<br />
update: 50% of requests<br />
now returned<br />
We have now had over 1,200 deaths in the<br />
anti-TNF cohort reported to the BSRBR and, in the<br />
last newsletter, we outlined a particular problem we<br />
were having due to missing death in<strong>for</strong>mation in<br />
around a third of these patient deaths. One of the<br />
primary outcomes of the Biologics Register has<br />
been to study the long-term safety of anti-TNF<br />
therapy and one of the most important outcomes<br />
has been death. All patients registered with the<br />
BSRBR are flagged with the NHS In<strong>for</strong>mation<br />
Centre (<strong>for</strong>merly the Office <strong>for</strong> National Statistics).<br />
<strong>The</strong>re<strong>for</strong>e, we are notified of all deaths and receive<br />
a copy of the death certificate. Un<strong>for</strong>tunately, we<br />
do not receive in<strong>for</strong>mation on whether the patient<br />
was receiving a biologic drug at the time of death.<br />
Without these details, it may be necessary to<br />
exclude these important patients from analyses,<br />
thus losing all of their in<strong>for</strong>mation collected to date.<br />
So far we have received 212 responses from 410<br />
requests <strong>for</strong> such death in<strong>for</strong>mation so we are still<br />
have 50% outstanding. We realise how difficult it<br />
can be to obtain this in<strong>for</strong>mation when a patient<br />
has died. If you have received one of these letters<br />
and are having trouble accessing data <strong>for</strong> any<br />
reason please contact the office on<br />
biologics.register@manchester.ac.uk.<br />
➜<br />
Reminder:<br />
Continued importance of follow-up data!<br />
If important drug therapy data or details relating<br />
to a serious adverse event are missing, it will often<br />
result in data being excluded from <strong>for</strong>thcoming<br />
BSRBR analyses, limiting the usefulness of the data<br />
collected at baseline. At the same time, we do really<br />
appreciate the burden we are putting on you and your<br />
team. Again, if you would like a list of patients who are<br />
not responding to our questionnaires please contact<br />
Pat Creighton at pat.creighton@manchester.ac.uk.<br />
Reporting adverse events<br />
Abbott – Adalimumab<br />
Chiara Dell'aria Burani BSc, MSc<br />
Affiliate Safety Representative<br />
Pharmacovigilance UK, Ireland & Malta<br />
Abbott UK, Abbott House,<br />
Vanwall Business Park,<br />
Vanwall Road, Maidenhead,<br />
Berkshire SL6 4XE - UK<br />
PcV: +44 (0)800 121 8267<br />
Tel +44 (0)1628 644175<br />
Fax +44 (0)1628 644236<br />
Email:<br />
chiara.dellaria-burani@abbott.com<br />
Biovitrum – Anakinra<br />
Gema Retama<br />
Senior Pharmacovigilance Specialist<br />
Biovitrum<br />
Quintiles Drug Safety and Medical<br />
Affairs, Europe Quintiles Ireland<br />
Limited East Point<br />
Business Park Fairview<br />
Dublin 3<br />
Tel: 0035318195242<br />
Fax: 0035318099501<br />
Email: gema.retama@quintiles.com<br />
Roche – Rituximab<br />
Dr Boshishi Mohlala,<br />
Drug Surveillance Physician<br />
Drug Safety and Risk Management<br />
www.rheumatology.org.uk<br />
It is essential that in<strong>for</strong>mation on all occurrences of all adverse events on<br />
registered patients is reported promptly to the BSRBR offices at the arc EU in<br />
Manchester. All available data <strong>for</strong> each adverse event should always be provided<br />
to assist the Register’s pharmacovigilance ef<strong>for</strong>t and ensure we have the best<br />
in<strong>for</strong>mation to assess the safety of these treatments both short-term and over<br />
the life of the register.<br />
If you also notify the MHRA of a suspected adverse drug reaction or a<br />
suspected defect in a product through the yellow card scheme please will<br />
you record this in the in<strong>for</strong>mation provided to the BSBR.<br />
In addition you may also notify or seek advice from the relevant company in<br />
relation to safety <strong>for</strong> each product using the following contacts:<br />
Roche Products Limited<br />
6 Falcon Way, Shire Park<br />
Welwyn Garden City AL7 1TW - UK<br />
Tel: +44( 0)1707-367554<br />
Fax:+44 (0)1707 384504<br />
Email: boshishi.mohlala@roche.com<br />
Schering Plough – Infliximab<br />
Graham Marshall<br />
Drug Safety Manager (UK and Ireland)<br />
Schering-Plough Ltd<br />
Welwyn Garden City<br />
Hert<strong>for</strong>dshire AL7 1TW - UK<br />
Tel: +44 (0)1707 363686<br />
Fax: +44 (0)1707 363696<br />
Mob: +44 (0)777 197 3280<br />
Email: graham.marshall@sp.com<br />
Wyeth – Etanercept<br />
Catherine Binns RN<br />
Head of Drug Safety<br />
Wyeth Pharmaceuticals<br />
Huntercombe Lane South<br />
Taplow, Maidenhead<br />
Berkshire SL6 0PH - UK<br />
Tel: +44 (0)1628 604377<br />
Fax: +44 (0)1628414025<br />
Dir: +44 (0)1628 413931<br />
Mob: +44 (0)7990 530138<br />
Email: binnsc@wyeth.com<br />
For all queries about this newsletter and suggestions <strong>for</strong> future issues, please contact:<br />
Nia Taylor, BSR Biologics Register Coordinator<br />
E: ntaylor@rheumatology.org.uk<br />
W: www.rheumatology.org.uk<br />
<strong>British</strong> <strong>Society</strong> <strong>for</strong> <strong>Rheumatology</strong>, Bride House, 18-20 Bride Lane, London EC4Y 8EE<br />
Registered Charity No. 1067124 Company No. 3470316, VAT No. 404 5637 66













