Cardiology Boards and Recertification - Mayo Clinic
Cardiology Boards and Recertification - Mayo Clinic
Cardiology Boards and Recertification - Mayo Clinic

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
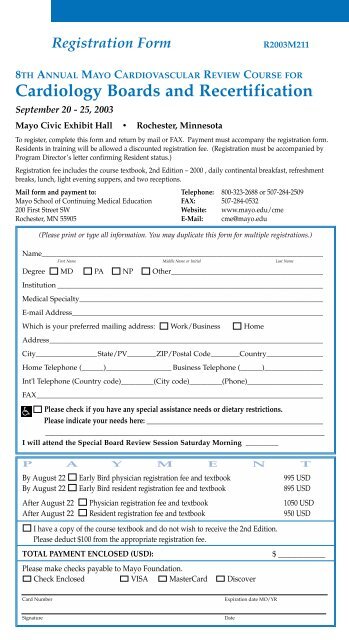
Registration Form<br />
R2003M211<br />
8TH ANNUAL MAYO CARDIOVASCULAR REVIEW COURSE FOR<br />
<strong>Cardiology</strong> <strong>Boards</strong> <strong>and</strong> <strong>Recertification</strong><br />
September 20 - 25, 2003<br />
<strong>Mayo</strong> Civic Exhibit Hall • Rochester, Minnesota<br />
To register, complete this form <strong>and</strong> return by mail or FAX. Payment must accompany the registration form.<br />
Residents in training will be allowed a discounted registration fee. (Registration must be accompanied by<br />
Program Director’s letter confirming Resident status.)<br />
Registration fee includes the course textbook, 2nd Edition – 2000 , daily continental breakfast, refreshment<br />
breaks, lunch, light evening suppers, <strong>and</strong> two receptions.<br />
Mail form <strong>and</strong> payment to: Telephone: 800-323-2688 or 507-284-2509<br />
<strong>Mayo</strong> School of Continuing Medical Education FAX: 507-284-0532<br />
200 First Street SW Website: www.mayo.edu/cme<br />
Rochester, MN 55905 E-Mail: cme@mayo.edu<br />
(Please print or type all information. You may duplicate this form for multiple registrations.)<br />
Name______________________________________________________________________________<br />
First Name Middle Name or Initial Last Name<br />
Degree MD PA NP Other__________________________________________<br />
Institution __________________________________________________________________________<br />
Medical Specialty____________________________________________________________________<br />
E-mail Address______________________________________________________________________<br />
Which is your preferred mailing address: Work/Business Home<br />
Address____________________________________________________________________________<br />
City_________________State/PV________ZIP/Postal Code________Country_________________<br />
Home Telephone (______)__________________ Business Telephone (______)_________________<br />
Int'l Telephone (Country code)_________(City code)_________(Phone)______________________<br />
FAX________________________________________________________________________________<br />
Please check if you have any special assistance needs or dietary restrictions.<br />
Please indicate your needs here: _____________________________________________________<br />
___________________________________________________________________________________<br />
I will attend the Special Board Review Session Saturday Morning _________<br />
P A Y M E N T<br />
By August 22 Early Bird physician registration fee <strong>and</strong> textbook 995 USD<br />
By August 22 Early Bird resident registration fee <strong>and</strong> textbook 895 USD<br />
After August 22 Physician registration fee <strong>and</strong> textbook 1050 USD<br />
After August 22 Resident registration fee <strong>and</strong> textbook 950 USD<br />
I have a copy of the course textbook <strong>and</strong> do not wish to receive the 2nd Edition.<br />
Please deduct $100 from the appropriate registration fee.<br />
TOTAL PAYMENT ENCLOSED (USD):<br />
$ _____________<br />
Please make checks payable to <strong>Mayo</strong> Foundation.<br />
Check Enclosed VISA MasterCard Discover<br />
Card Number<br />
Expiration date MO/YR<br />
Signature<br />
Date