Mail to: - Texas Department of Insurance
Mail to: - Texas Department of Insurance
Mail to: - Texas Department of Insurance

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
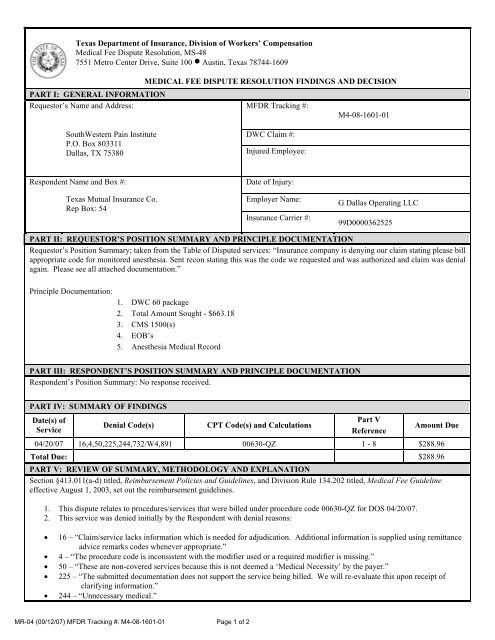
<strong>Texas</strong> <strong>Department</strong> <strong>of</strong> <strong>Insurance</strong>, Division <strong>of</strong> Workers’ Compensation<br />
Medical Fee Dispute Resolution, MS-48<br />
7551 Metro Center Drive, Suite 100 • Austin, <strong>Texas</strong> 78744-1609<br />
MEDICAL FEE DISPUTE RESOLUTION FINDINGS AND DECISION<br />
PART I: GENERAL INFORMATION<br />
Reques<strong>to</strong>r’s Name and Address: MFDR Tracking #:<br />
M4-08-1601-01<br />
SouthWestern Pain Institute<br />
P.O. Box 803311<br />
Dallas, TX 75380<br />
DWC Claim #:<br />
Injured Employee:<br />
Respondent Name and Box #:<br />
<strong>Texas</strong> Mutual <strong>Insurance</strong> Co.<br />
Rep Box: 54<br />
Date <strong>of</strong> Injury:<br />
Employer Name:<br />
<strong>Insurance</strong> Carrier #:<br />
G Dallas Operating LLC<br />
99D0000362525<br />
PART II: REQUESTOR’S POSITION SUMMARY AND PRINCIPLE DOCUMENTATION<br />
Reques<strong>to</strong>r’s Position Summary; taken from the Table <strong>of</strong> Disputed services: “<strong>Insurance</strong> company is denying our claim stating please bill<br />
appropriate code for moni<strong>to</strong>red anesthesia. Sent recon stating this was the code we requested and was authorized and claim was denial<br />
again. Please see all attached documentation.”<br />
Principle Documentation:<br />
1. DWC 60 package<br />
2. Total Amount Sought - $663.18<br />
3. CMS 1500(s)<br />
4. EOB’s<br />
5. Anesthesia Medical Record<br />
PART III: RESPONDENT’S POSITION SUMMARY AND PRINCIPLE DOCUMENTATION<br />
Respondent’s Position Summary: No response received.<br />
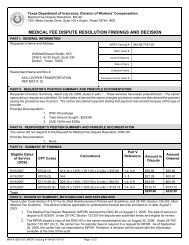
PART IV: SUMMARY OF FINDINGS<br />
Date(s) <strong>of</strong><br />
Service<br />
Denial Code(s)<br />
CPT Code(s) and Calculations<br />
Part V<br />
Reference<br />
Amount Due<br />
04/20/07 16,4,50,225,244,732/W4,891 00630-QZ 1 - 8 $288.96<br />
Total Due: $288.96<br />
PART V: REVIEW OF SUMMARY, METHODOLOGY AND EXPLANATION<br />
Section §413.011(a-d) titled, Reimbursement Policies and Guidelines, and Division Rule 134.202 titled, Medical Fee Guideline<br />
effective August 1, 2003, set out the reimbursement guidelines.<br />
1. This dispute relates <strong>to</strong> procedures/services that were billed under procedure code 00630-QZ for DOS 04/20/07.<br />
2. This service was denied initially by the Respondent with denial reasons:<br />
• 16 – “Claim/service lacks information which is needed for adjudication. Additional information is supplied using remittance<br />
advice remarks codes whenever appropriate.”<br />
• 4 – “The procedure code is inconsistent with the modifier used or a required modifier is missing.”<br />
• 50 – “These are non-covered services because this is not deemed a ‘Medical Necessity’ by the payer.”<br />
• 225 – “The submitted documentation does not support the service being billed. We will re-evaluate this upon receipt <strong>of</strong><br />
clarifying information.”<br />
• 244 – “Unnecessary medical.”<br />
MR-04 (09/12/07) MFDR Tracking #: M4-08-1601-01 Page 1 <strong>of</strong> 2
• 732 – “Accurate coding is essential for reimbursement. Services are not reimbursable as billed. CPT and/modifier billed<br />
incorrectly.<br />
3. These services was denied by the Respondent, after reconsideration with denial reasons:<br />
• W4 – “No additional reimbursement allowed after review <strong>of</strong> appeal/reconsideration.”<br />
• 891 – “The insurance company is reducing or denying payment after reconsidering a bill.”<br />
4. The Reques<strong>to</strong>r submitted relevant documentation <strong>to</strong> substantiate the level <strong>of</strong> anesthesia service billed. Per Rule 134.600 (c)<br />
(1) (B) carrier is liable for all reasonable and necessary medical costs relating <strong>to</strong> the health care: preauthorization <strong>of</strong><br />
any health care listed in subsection (p) <strong>of</strong> this section that was approved prior <strong>to</strong> providing the health care.<br />
Therefore the carrier is liable for all reasonable and necessary medical costs relating <strong>to</strong> this procedure.<br />
5. The Reques<strong>to</strong>r was given preauthorization for a LT Sacroiliac injection and LT Sciatic nerve/piriformis injection, according<br />
<strong>to</strong> the preauthorization letter dated April 02, 2007 and Case Number: 1906118.<br />
6. Per Commissioner’s Bulletin #B-0028-07, if a specified health care treatment or service is preauthorized,<br />
treatment/service and related ancillary charges for services provided within a the preauthorized service is not subject <strong>to</strong><br />
retrospective review <strong>of</strong> the medical necessity <strong>of</strong> the treatment service.<br />
90 minutes ÷ 15 = 6 units<br />
CPT code 00630-QZ =8 units + 6 units = 14 units<br />
$16.51(2007conversion fac<strong>to</strong>r) x 125%= $20.64<br />
$20.64 x 14 units =$288.96 (MAR)<br />
7. Therefore, according <strong>to</strong> rule 134.202(c) (1) reimbursement <strong>of</strong> $288.96 is recommended.<br />
8. A referral has been made <strong>to</strong> Legal and Enforcement.<br />
PART VI: GENERAL PAYMENT POLICIES/REFERENCES<br />
<strong>Texas</strong> Labor Code Section 413.011(a-d), Section 413.031 and Section 413.0311<br />
28 <strong>Texas</strong> Administrative Code Section 134.1, Section 134.202, 134.600<br />
<strong>Texas</strong> Government Code, Chapter 2001, Subchapter G<br />
Commissioner’s Bulletin #B-0028-07<br />
PART VII: DIVISION DECISION<br />
Based upon the documentation submitted by the parties and in accordance with the provisions <strong>of</strong> <strong>Texas</strong> Labor Code Section 413.031,<br />
the Division has determined that the Reques<strong>to</strong>r is entitled <strong>to</strong> reimbursement. The Division hereby ORDERS the Carrier <strong>to</strong> remit <strong>to</strong> the<br />
Reques<strong>to</strong>r the amount <strong>of</strong> $288.96 plus applicable accrued interest per Division Rule 134.130, due within 30 days <strong>of</strong> receipt <strong>of</strong> this<br />
Order.<br />
ORDER :<br />
01/11/08<br />
Authorized Signature Medical Fee Dispute Resolution Officer Date<br />
PART VIII: YOUR RIGHT TO REQUEST JUDICIAL REVIEW<br />
Either party <strong>to</strong> this medical fee dispute has a right <strong>to</strong> request an appeal. A request for hearing must be in writing and it must be<br />
received by the DWC Chief Clerk <strong>of</strong> Proceedings within 20 (twenty) days <strong>of</strong> your receipt <strong>of</strong> this decision. A request for hearing<br />
should be sent <strong>to</strong>: Chief Clerk <strong>of</strong> Proceedings, <strong>Texas</strong> <strong>Department</strong> <strong>of</strong> <strong>Insurance</strong>, Division <strong>of</strong> Workers Compensation, P.O. Box<br />
17787, Austin, <strong>Texas</strong>, 78744. Please include a copy <strong>of</strong> the Medical Fee Dispute Resolution Findings and Decision <strong>to</strong>gether with<br />
other required information specified in Division Rule 148.3(c).<br />
Under <strong>Texas</strong> Labor Code Section 413.0311, your appeal will be handled by a Division hearing under Title 28 <strong>Texas</strong> Administrative<br />
Code Chapter 142 Rules if the <strong>to</strong>tal amount sought does not exceed $2,000. If the <strong>to</strong>tal amount sought exceeds $2,000, a hearing<br />
will be conducted by the State Office <strong>of</strong> Administrative Hearings under <strong>Texas</strong> Labor Code Section 413.031.<br />
Si prefiere hablar con una persona en español acerca de ésta correspondencia, favor de llamar a 512-804-4812.<br />
MR-04 (09/12/07) MFDR Tracking #: M4-08-1601-01 Page 2 <strong>of</strong> 2
MR-04 (09/12/07) MFDR Tracking #: M4-08-1601-01 Page 3 <strong>of</strong> 2