SERIOUS ADVERSE EVENT FORM - Universitätsklinikum Essen
SERIOUS ADVERSE EVENT FORM - Universitätsklinikum Essen
SERIOUS ADVERSE EVENT FORM - Universitätsklinikum Essen

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
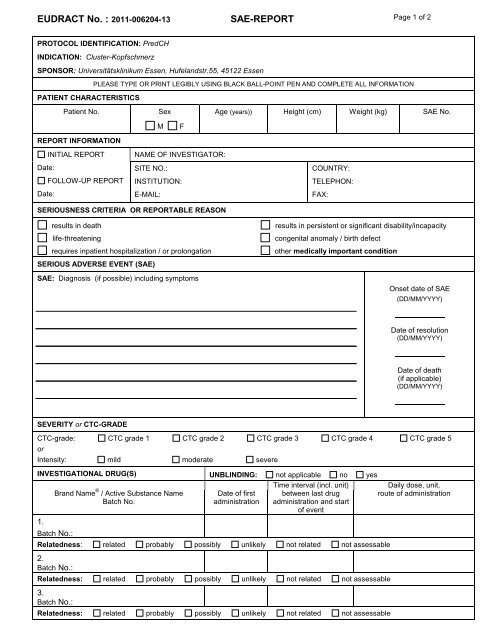
EUDRACT No. : 2011-006204-13 SAE-REPORT Page 1 of 2<br />
PROTOCOL IDENTIFICATION: PredCH<br />
INDICATION: Cluster-Kopfschmerz<br />
SPONSOR: Universitätsklinikum <strong>Essen</strong>, Hufelandstr.55, 45122 <strong>Essen</strong><br />
PLEASE TYPE OR PRINT LEGIBLY USING BLACK BALL-POINT PEN AND COMPLETE ALL IN<strong>FORM</strong>ATION<br />
PATIENT CHARACTERISTICS<br />
Patient No.<br />
Sex<br />
Age (years)) Height (cm) Weight (kg) SAE No.<br />
M<br />
F<br />
REPORT IN<strong>FORM</strong>ATION<br />
INITIAL REPORT<br />
Date:<br />
FOLLOW-UP REPORT<br />
Date:<br />
NAME OF INVESTIGATOR:<br />
SITE NO.:<br />
INSTITUTION:<br />
E-MAIL:<br />
COUNTRY:<br />
TELEPHON:<br />
FAX:<br />
<strong>SERIOUS</strong>NESS CRITERIA OR REPORTABLE REASON<br />
results in death<br />
life-threatening<br />
requires inpatient hospitalization / or prolongation<br />
results in persistent or significant disability/incapacity<br />
congenital anomaly / birth defect<br />
other medically important condition<br />
<strong>SERIOUS</strong> <strong>ADVERSE</strong> <strong>EVENT</strong> (SAE)<br />
SAE: Diagnosis (if possible) including symptoms<br />
Onset date of SAE<br />
(DD/MM/YYYY)<br />
Date of resolution<br />
(DD/MM/YYYY)<br />
Date of death<br />
(if applicable)<br />
(DD/MM/YYYY)<br />
SEVERITY or CTC-GRADE<br />
CTC-grade: CTC grade 1 CTC grade 2 CTC grade 3 CTC grade 4 CTC grade 5<br />
or<br />
Intensity: mild moderate severe<br />
INVESTIGATIONAL DRUG(S) UNBLINDING: not applicable no yes<br />
1.<br />
Brand Name ® / Active Substance Name<br />
Batch No.<br />
Batch No.:<br />
Date of first<br />
administration<br />
Time interval (incl. unit)<br />
between last drug<br />
administration and start<br />
of event<br />
Relatedness: related probably possibly unlikely not related not assessable<br />
2.<br />
Batch No.:<br />
Relatedness: related probably possibly unlikely not related not assessable<br />
3.<br />
Batch No.:<br />
Relatedness: related probably possibly unlikely not related not assessable<br />
Daily dose, unit,<br />
route of administration
PLEASE TYPE OR PRINT LEGIBLY USING BLACK BALL-POINT PEN AND COMPLETE ALL IN<strong>FORM</strong>ATION<br />
PATIENT IN<strong>FORM</strong>ATION<br />
Patient- No. Age (years) SAE No. INITIAL REPORT Date:<br />
FOLLOW-UP Date:<br />
RELEVANT MEDICAL HISTORY (pre-existing / concurrent conditions) Start date Stop date<br />
1.<br />
2.<br />
3.<br />
RELEVANT CONCOMITANT MEDICATION<br />
Indication<br />
Daily dose, unit,<br />
route of<br />
administration<br />
Date of first<br />
administration<br />
Date of last<br />
administration<br />
1.<br />
2.<br />
3.<br />
RELEVANT LAB FINDINGS OR INVESTIGATIONS<br />
Normal range Date Result<br />
1.<br />
2.<br />
3.<br />
4.<br />
TREATMENT OF SAE ACTION TAKEN WITH TRIAL MEDICATION OUTCOME OF SAE<br />
none<br />
drug treatment<br />
others<br />
Specify:<br />
COMMENT:<br />
dose not changed<br />
dose reduced<br />
dose increased<br />
drug withdrawn, date: ___________<br />
Has a rechallenge been done?<br />
yes no unknown<br />
Did reaction recur on readministration?<br />
yes no unknown<br />
unknown<br />
not applicable<br />
recovered / resolved<br />
recovering / resolving<br />
not recovered / not resolved<br />
recovered / resolved with sequelae<br />
fatal<br />
cause of death:<br />
autopsy? yes no<br />
unknown<br />
INVESTIGATOR SIGNATURE<br />
Name Signature Date (DD/MM/YYYY)<br />
FAX WITHIN 24 Hours TO PD. Dr. M. Obermann: FAX No. 0201-723-5542