April 2007 - Division of Biology and Medicine - Brown University
April 2007 - Division of Biology and Medicine - Brown University
April 2007 - Division of Biology and Medicine - Brown University

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Idiopathic Scoliosis In Children: An Update<br />
The diagnosis <strong>of</strong> scoliosis in a growing<br />
child is <strong>of</strong>ten a cause for great concern<br />
for the patient’s family <strong>and</strong> primary physician.<br />
Treatment in the past <strong>of</strong>ten involved<br />
lengthy hospital stays, prolonged<br />
bed rest, <strong>and</strong> postoperative casting. Even<br />
patients treated non-operatively suffered<br />
the stigma <strong>of</strong> the Milwaukee brace, a<br />
metal framed structure extending from<br />
the hips to the chin, worn 23 hours daily.<br />
Modern insight into the potential causes<br />
<strong>of</strong> scoliosis, the evaluation <strong>of</strong> a child with<br />
spinal deformity, <strong>and</strong> advanced operative<br />
<strong>and</strong> non-operative treatments allow successful<br />
treatment <strong>of</strong> patients <strong>of</strong> all ages<br />
with scoliosis.<br />
<br />
Craig P. Eberson, MD<br />
BACKGROUND<br />
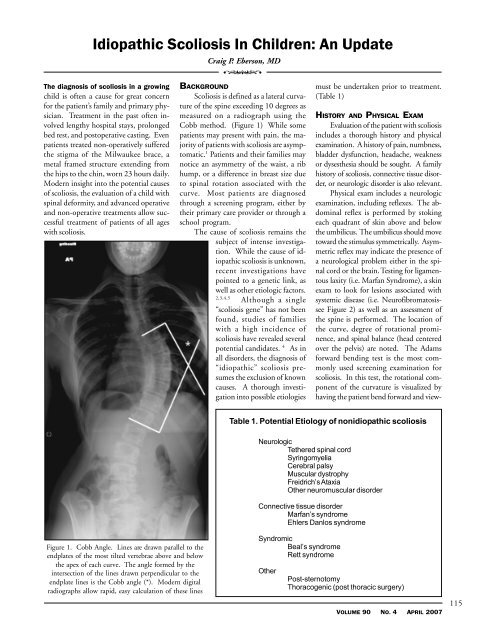
Scoliosis is defined as a lateral curvature<br />
<strong>of</strong> the spine exceeding 10 degrees as<br />
measured on a radiograph using the<br />
Cobb method. (Figure 1) While some<br />
patients may present with pain, the majority<br />
<strong>of</strong> patients with scoliosis are asymptomatic.<br />
1 Patients <strong>and</strong> their families may<br />
notice an asymmetry <strong>of</strong> the waist, a rib<br />
hump, or a difference in breast size due<br />
to spinal rotation associated with the<br />
curve. Most patients are diagnosed<br />
through a screening program, either by<br />
their primary care provider or through a<br />
school program.<br />
The cause <strong>of</strong> scoliosis remains the<br />
subject <strong>of</strong> intense investigation.<br />
While the cause <strong>of</strong> idiopathic<br />
scoliosis is unknown,<br />
recent investigations have<br />
pointed to a genetic link, as<br />
well as other etiologic factors.<br />
2,3,4,5<br />
Although a single<br />
“scoliosis gene” has not been<br />
found, studies <strong>of</strong> families<br />
with a high incidence <strong>of</strong><br />
scoliosis have revealed several<br />
potential c<strong>and</strong>idates. 4 As in<br />
all disorders, the diagnosis <strong>of</strong><br />
“idiopathic” scoliosis presumes<br />
the exclusion <strong>of</strong> known<br />
causes. A thorough investigation<br />
into possible etiologies<br />
must be undertaken prior to treatment.<br />
(Table 1)<br />
HISTORY AND PHYSICAL EXAM<br />
Evaluation <strong>of</strong> the patient with scoliosis<br />
includes a thorough history <strong>and</strong> physical<br />
examination. A history <strong>of</strong> pain, numbness,<br />
bladder dysfunction, headache, weakness<br />
or dysesthesia should be sought. A family<br />
history <strong>of</strong> scoliosis, connective tissue disorder,<br />
or neurologic disorder is also relevant.<br />
Physical exam includes a neurologic<br />
examination, including reflexes. The abdominal<br />
reflex is performed by stoking<br />
each quadrant <strong>of</strong> skin above <strong>and</strong> below<br />
the umbilicus. The umbilicus should move<br />
toward the stimulus symmetrically. Asymmetric<br />
reflex may indicate the presence <strong>of</strong><br />
a neurological problem either in the spinal<br />
cord or the brain. Testing for ligamentous<br />
laxity (i.e. Marfan Syndrome), a skin<br />
exam to look for lesions associated with<br />
systemic disease (i.e. Neur<strong>of</strong>ibromatosissee<br />
Figure 2) as well as an assessment <strong>of</strong><br />
the spine is performed. The location <strong>of</strong><br />
the curve, degree <strong>of</strong> rotational prominence,<br />
<strong>and</strong> spinal balance (head centered<br />
over the pelvis) are noted. The Adams<br />
forward bending test is the most commonly<br />
used screening examination for<br />
scoliosis. In this test, the rotational component<br />
<strong>of</strong> the curvature is visualized by<br />
having the patient bend forward <strong>and</strong> view-<br />
Table 1. Potential Etiology <strong>of</strong> nonidiopathic scoliosis<br />
Neurologic<br />
Tethered spinal cord<br />
Syringomyelia<br />
Cerebral palsy<br />
Muscular dystrophy<br />
Freidrich’s Ataxia<br />
Other neuromuscular disorder<br />
Connective tissue disorder<br />
Marfan’s syndrome<br />
Ehlers Danlos syndrome<br />
Figure 1. Cobb Angle. Lines are drawn parallel to the<br />
endplates <strong>of</strong> the most tilted vertebrae above <strong>and</strong> below<br />
the apex <strong>of</strong> each curve. The angle formed by the<br />
intersection <strong>of</strong> the lines drawn perpendicular to the<br />
endplate lines is the Cobb angle (*). Modern digital<br />
radiographs allow rapid, easy calculation <strong>of</strong> these lines<br />
Syndromic<br />
Beal’s syndrome<br />
Rett syndrome<br />
Other<br />
Post-sternotomy<br />
Thoracogenic (post thoracic surgery)<br />
VOLUME 90 NO. 4 APRIL <strong>2007</strong><br />
115