HECS Reimbursement Scheme Bank account details form
HECS Reimbursement Scheme Bank account details form
HECS Reimbursement Scheme Bank account details form

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
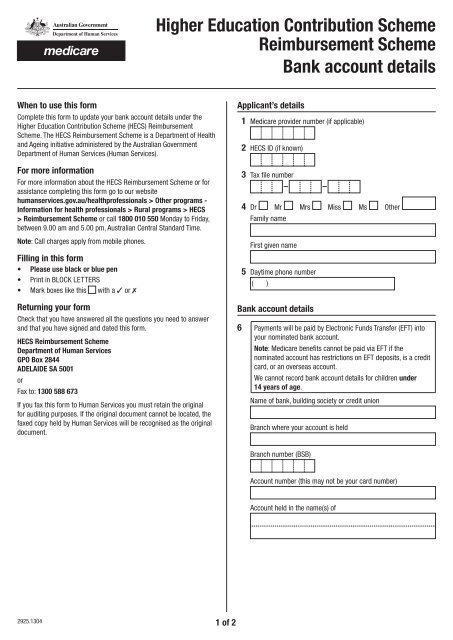
Higher Education Contribution <strong>Scheme</strong><br />
<strong>Reimbursement</strong> <strong>Scheme</strong><br />
<strong>Bank</strong> <strong>account</strong> <strong>details</strong><br />
When to use this <strong>form</strong><br />
Complete this <strong>form</strong> to update your bank <strong>account</strong> <strong>details</strong> under the<br />
Higher Education Contribution <strong>Scheme</strong> (<strong>HECS</strong>) <strong>Reimbursement</strong><br />
<strong>Scheme</strong>. The <strong>HECS</strong> <strong>Reimbursement</strong> <strong>Scheme</strong> is a Department of Health<br />
and Ageing initiative administered by the Australian Government<br />
Department of Human Services (Human Services).<br />
For more in<strong>form</strong>ation<br />
For more in<strong>form</strong>ation about the <strong>HECS</strong> <strong>Reimbursement</strong> <strong>Scheme</strong> or for<br />
assistance completing this <strong>form</strong> go to our website<br />
humanservices.gov.au/healthprofessionals > Other programs -<br />
In<strong>form</strong>ation for health professionals > Rural programs > <strong>HECS</strong><br />
> <strong>Reimbursement</strong> <strong>Scheme</strong> or call 1800 010 550 Monday to Friday,<br />
between 9.00 am and 5.00 pm, Australian Central Standard Time.<br />
Note: Call charges apply from mobile phones.<br />
Filling in this <strong>form</strong><br />
• Please use black or blue pen<br />
• Print in BLOCK LETTERS<br />
• Mark boxes like this with a ✓ or 7<br />
Returning your <strong>form</strong><br />
Check that you have answered all the questions you need to answer<br />
and that you have signed and dated this <strong>form</strong>.<br />
<strong>HECS</strong> <strong>Reimbursement</strong> <strong>Scheme</strong><br />
Department of Human Services<br />
GPO Box 2844<br />
ADELAIDE SA 5001<br />
or<br />
Fax to: 1300 588 673<br />
If you fax this <strong>form</strong> to Human Services you must retain the original<br />
for auditing purposes. If the original document cannot be located, the<br />
faxed copy held by Human Services will be recognised as the original<br />
document.<br />
Applicant’s <strong>details</strong><br />
1 Medicare provider number (if applicable)<br />
2 <strong>HECS</strong> ID (if known)<br />
3 Tax file number<br />
4 Dr Mr Mrs Miss Ms Other<br />
Family name<br />
First given name<br />
5 Daytime phone number<br />
( )<br />
<strong>Bank</strong> <strong>account</strong> <strong>details</strong><br />
6 Payments will be paid by Electronic Funds Transfer (EFT) into<br />
your nominated bank <strong>account</strong>.<br />
Note: Medicare benefits cannot be paid via EFT if the<br />
nominated <strong>account</strong> has restrictions on EFT deposits, is a credit<br />
card, or an overseas <strong>account</strong>.<br />
We cannot record bank <strong>account</strong> <strong>details</strong> for children under<br />
14 years of age.<br />
Name of bank, building society or credit union<br />
Branch where your <strong>account</strong> is held<br />
Branch number (BSB)<br />
Account number (this may not be your card number)<br />
Account held in the name(s) of<br />
2925.1304 1 of 2
Declaration<br />
7 I agree to:<br />
• authorise the Department of Human Services to direct all<br />
payments relating to the Higher Education Contribution<br />
<strong>Scheme</strong> <strong>Reimbursement</strong> <strong>Scheme</strong> and the provider number<br />
identified on this <strong>form</strong> into the nominated bank <strong>account</strong>.<br />
I declare that:<br />
• the in<strong>form</strong>ation provided in this <strong>form</strong> is complete and correct.<br />
I understand that:<br />
• giving false or misleading in<strong>form</strong>ation is a serious offence.<br />
Applicant’s signature<br />
Date<br />
- / /<br />
Privacy notice<br />
Centrelink, Medicare, Child Support and CRS Australia are services<br />
within the Australian Government Department of Human Services<br />
(Human Services).<br />
Your personal in<strong>form</strong>ation is protected by law, including the<br />
Privacy Act 1988. Your in<strong>form</strong>ation is collected for Social Security,<br />
Family Assistance, Medicare, Child Support and CRS purposes. This<br />
in<strong>form</strong>ation may be required by the powers provided within each<br />
services’ legislation or voluntarily given by you when you apply for<br />
services or payments.<br />
Your in<strong>form</strong>ation will be used for the assessment and administration<br />
of payments and services. Your in<strong>form</strong>ation may also be used within<br />
Human Services, where you have provided consent or it is required or<br />
authorised by law. Human Services may disclose your in<strong>form</strong>ation to<br />
Commonwealth Departments, other persons, bodies or agencies ONLY<br />
where you have provided consent or it is required or authorised by law.<br />
You can get more in<strong>form</strong>ation about privacy by going to our website<br />
humanservices.gov.au/privacy or requesting a copy of the full<br />
privacy policy at any of our Service Centres.<br />
2925.1304 2 of 2