Anthem Blue Cross Avondale Represented EPO
Anthem Blue Cross Avondale Represented EPO
Anthem Blue Cross Avondale Represented EPO

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
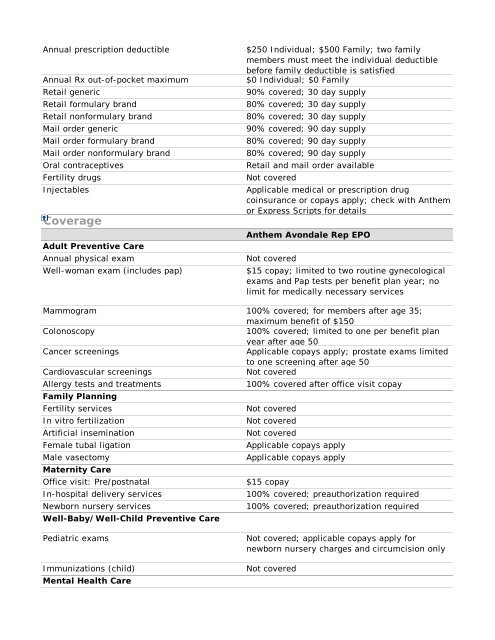
Annual prescription deductible<br />
Annual Rx out-of-pocket maximum<br />
Retail generic<br />
Retail formulary brand<br />
Retail nonformulary brand<br />
Mail order generic<br />
Mail order formulary brand<br />
Mail order nonformulary brand<br />
Oral contraceptives<br />
Fertility drugs<br />
Injectables<br />
Coverage<br />
Adult Preventive Care<br />
Annual physical exam<br />
Well-woman exam (includes pap)<br />
$250 Individual; $500 Family; two family<br />
members must meet the individual deductible<br />
before family deductible is satisfied<br />
$0 Individual; $0 Family<br />
90% covered; 30 day supply<br />
80% covered; 30 day supply<br />
80% covered; 30 day supply<br />
90% covered; 90 day supply<br />
80% covered; 90 day supply<br />
80% covered; 90 day supply<br />
Retail and mail order available<br />
Not covered<br />
Applicable medical or prescription drug<br />
coinsurance or copays apply; check with <strong>Anthem</strong><br />
or Express Scripts for details<br />
<strong>Anthem</strong> <strong>Avondale</strong> Rep <strong>EPO</strong><br />
Not covered<br />
$15 copay; limited to two routine gynecological<br />
exams and Pap tests per benefit plan year; no<br />
limit for medically necessary services<br />
Mammogram 100% covered; for members after age 35;<br />
maximum benefit of $150<br />
Colonoscopy<br />
100% covered; limited to one per benefit plan<br />
year after age 50<br />
Cancer screenings<br />
Applicable copays apply; prostate exams limited<br />
to one screening after age 50<br />
Cardiovascular screenings<br />
Not covered<br />
Allergy tests and treatments<br />
100% covered after office visit copay<br />
Family Planning<br />
Fertility services<br />
Not covered<br />
In vitro fertilization<br />
Not covered<br />
Artificial insemination<br />
Not covered<br />
Female tubal ligation<br />
Applicable copays apply<br />
Male vasectomy<br />
Applicable copays apply<br />
Maternity Care<br />
Office visit: Pre/postnatal<br />
$15 copay<br />
In-hospital delivery services<br />
100% covered; preauthorization required<br />
Newborn nursery services<br />
100% covered; preauthorization required<br />
Well-Baby/Well-Child Preventive Care<br />
Pediatric exams<br />
Immunizations (child)<br />
Mental Health Care<br />
Not covered; applicable copays apply for<br />
newborn nursery charges and circumcision only<br />
Not covered