Anthem Blue Cross Avondale Represented EPO
Anthem Blue Cross Avondale Represented EPO
Anthem Blue Cross Avondale Represented EPO

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
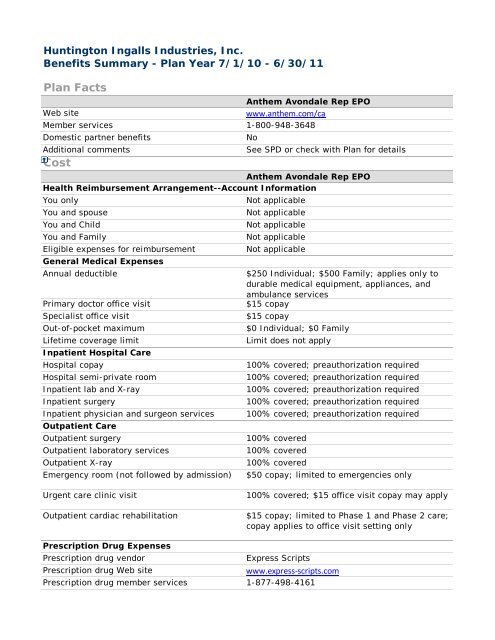
Huntington Ingalls Industries, Inc.<br />
Benefits Summary - Plan Year 7/1/10 - 6/30/11<br />
Plan Facts<br />
<strong>Anthem</strong> <strong>Avondale</strong> Rep <strong>EPO</strong><br />
Web site<br />
www.anthem.com/ca<br />
Member services 1-800-948-3648<br />
Domestic partner benefits<br />
No<br />
Additional comments<br />
See SPD or check with Plan for details<br />
Cost<br />
<strong>Anthem</strong> <strong>Avondale</strong> Rep <strong>EPO</strong><br />
Health Reimbursement Arrangement--Account Information<br />
You only<br />
Not applicable<br />
You and spouse<br />
Not applicable<br />
You and Child<br />
Not applicable<br />
You and Family<br />
Not applicable<br />
Eligible expenses for reimbursement<br />
Not applicable<br />
General Medical Expenses<br />
Annual deductible<br />
$250 Individual; $500 Family; applies only to<br />
durable medical equipment, appliances, and<br />
ambulance services<br />
Primary doctor office visit<br />
$15 copay<br />
Specialist office visit<br />
$15 copay<br />
Out-of-pocket maximum<br />
$0 Individual; $0 Family<br />
Lifetime coverage limit<br />
Limit does not apply<br />
Inpatient Hospital Care<br />
Hospital copay<br />
100% covered; preauthorization required<br />
Hospital semi-private room<br />
100% covered; preauthorization required<br />
Inpatient lab and X-ray<br />
100% covered; preauthorization required<br />
Inpatient surgery<br />
100% covered; preauthorization required<br />
Inpatient physician and surgeon services 100% covered; preauthorization required<br />
Outpatient Care<br />
Outpatient surgery<br />
100% covered<br />
Outpatient laboratory services<br />
100% covered<br />
Outpatient X-ray<br />
100% covered<br />
Emergency room (not followed by admission) $50 copay; limited to emergencies only<br />
Urgent care clinic visit<br />
Outpatient cardiac rehabilitation<br />
100% covered; $15 office visit copay may apply<br />
$15 copay; limited to Phase 1 and Phase 2 care;<br />
copay applies to office visit setting only<br />
Prescription Drug Expenses<br />
Prescription drug vendor<br />
Express Scripts<br />
Prescription drug Web site<br />
www.express-scripts.com<br />
Prescription drug member services 1-877-498-4161
Annual prescription deductible<br />
Annual Rx out-of-pocket maximum<br />
Retail generic<br />
Retail formulary brand<br />
Retail nonformulary brand<br />
Mail order generic<br />
Mail order formulary brand<br />
Mail order nonformulary brand<br />
Oral contraceptives<br />
Fertility drugs<br />
Injectables<br />
Coverage<br />
Adult Preventive Care<br />
Annual physical exam<br />
Well-woman exam (includes pap)<br />
$250 Individual; $500 Family; two family<br />
members must meet the individual deductible<br />
before family deductible is satisfied<br />
$0 Individual; $0 Family<br />
90% covered; 30 day supply<br />
80% covered; 30 day supply<br />
80% covered; 30 day supply<br />
90% covered; 90 day supply<br />
80% covered; 90 day supply<br />
80% covered; 90 day supply<br />
Retail and mail order available<br />
Not covered<br />
Applicable medical or prescription drug<br />
coinsurance or copays apply; check with <strong>Anthem</strong><br />
or Express Scripts for details<br />
<strong>Anthem</strong> <strong>Avondale</strong> Rep <strong>EPO</strong><br />
Not covered<br />
$15 copay; limited to two routine gynecological<br />
exams and Pap tests per benefit plan year; no<br />
limit for medically necessary services<br />
Mammogram 100% covered; for members after age 35;<br />
maximum benefit of $150<br />
Colonoscopy<br />
100% covered; limited to one per benefit plan<br />
year after age 50<br />
Cancer screenings<br />
Applicable copays apply; prostate exams limited<br />
to one screening after age 50<br />
Cardiovascular screenings<br />
Not covered<br />
Allergy tests and treatments<br />
100% covered after office visit copay<br />
Family Planning<br />
Fertility services<br />
Not covered<br />
In vitro fertilization<br />
Not covered<br />
Artificial insemination<br />
Not covered<br />
Female tubal ligation<br />
Applicable copays apply<br />
Male vasectomy<br />
Applicable copays apply<br />
Maternity Care<br />
Office visit: Pre/postnatal<br />
$15 copay<br />
In-hospital delivery services<br />
100% covered; preauthorization required<br />
Newborn nursery services<br />
100% covered; preauthorization required<br />
Well-Baby/Well-Child Preventive Care<br />
Pediatric exams<br />
Immunizations (child)<br />
Mental Health Care<br />
Not covered; applicable copays apply for<br />
newborn nursery charges and circumcision only<br />
Not covered
Mental Health: Combined with substance abuse Yes; outpatient only<br />
Mental Health: Outpatient coverage<br />
Mental Health: Inpatient coverage<br />
Behavioral health member services<br />
Behavioral health vendor<br />
Behavioral health Web site<br />
Substance Abuse Care<br />
Detox: Outpatient coverage<br />
Detox: Inpatient coverage<br />
Rehab: Outpatient coverage<br />
Rehab: Inpatient coverage<br />
Dental<br />
Dental implants<br />
Accidental injury to teeth<br />
Surgical removal of tumors, cysts, and<br />
impacted teeth<br />
Vision Care<br />
Routine vision exams<br />
Regular lenses and frames<br />
Contact lenses<br />
Hearing Care<br />
Hearing evaluations<br />
Hearing aids<br />
Medical Therapy<br />
Acupuncture<br />
Chiropractic<br />
Outpatient physical therapy<br />
Outpatient speech therapy<br />
Outpatient occupational therapy<br />
Care at Alternate Sites<br />
Noncustodial home health care<br />
Prescribed care in noncustodial skilled nursing<br />
facility<br />
Hospice care<br />
Other Services<br />
80% covered; limited to 24 hour crisis<br />
intervention and evaluation/outpatient<br />
counseling; limited to 50 visits per year<br />
100% covered; limited to 30 days per year<br />
Same as medical plan<br />
Same as medical plan<br />
Same as medical plan<br />
80% covered; limited to 24 hour crisis<br />
intervention and evaluation/outpatient<br />
counseling; limited to 50 visits per year<br />
100% covered; limited to 2 episodes per<br />
lifetime; dependents not covered<br />
80% covered; limited to 24 hour crisis<br />
intervention and evaluation/outpatient<br />
counseling; limited to 50 visits per year<br />
Not covered<br />
Not covered<br />
$15 copay<br />
Applicable copays apply; limited to surgical<br />
removal of tumors and cysts; removal of<br />
impacted teeth not covered<br />
Not covered<br />
Not covered<br />
Not covered<br />
Not covered<br />
Not covered<br />
Not covered<br />
50% covered; limited to $500 per benefit plan<br />
year; including x-rays<br />
$15 copay; limited to 60 visits per benefit plan<br />
year<br />
$15 copay; limited to 60 visits per benefit plan<br />
year<br />
$15 copay; limited to 60 visits per benefit plan<br />
year<br />
100% covered; limited to 30 days;<br />
preauthorization required<br />
100% covered; limited to 50 days;<br />
preauthorization required<br />
100% covered
Ambulance services<br />
Durable medical equipment<br />
Prosthetic devices<br />
Access<br />
Out-of-area dependent coverage<br />
Out-of-area participant coverage<br />
Domestic partner benefits<br />
Ease of Use<br />
Ability to self-refer to OB/GYN<br />
Ability to self-refer to specialists<br />
Member Satisfaction<br />
80% covered after deductible is met; limited to<br />
nearest hospital and emergencies only<br />
80% covered after deductible is met;<br />
preauthorization required<br />
80% covered after deductible is met;<br />
preauthorization required<br />
<strong>Anthem</strong> <strong>Avondale</strong> Rep <strong>EPO</strong><br />
Yes<br />
Yes<br />
No<br />
<strong>Anthem</strong> <strong>Avondale</strong> Rep <strong>EPO</strong><br />
Yes<br />
Yes<br />
<strong>Anthem</strong> <strong>Avondale</strong> Rep <strong>EPO</strong><br />
% satisfied with plan overall<br />
Health plan average<br />
Not available<br />
National average 88%<br />
% satisfied with quality of care provided<br />
Health plan average<br />
Not available<br />
National average 94%<br />
% satisfied with plan's convenience/ease of use<br />
Health plan average<br />
Not available<br />
National average 90%<br />
% satisfied with types of services covered<br />
Health plan average<br />
Not available<br />
National average 89%<br />
Care Management: Education<br />
and Assistance<br />
Asthma care management<br />
Cancer care management<br />
Diabetes care management<br />
Heart disease care management<br />
Hypertension care management<br />
Smoking cessation program<br />
Weight control program<br />
Prenatal care management<br />
<strong>Anthem</strong> <strong>Avondale</strong> Rep <strong>EPO</strong><br />
No<br />
No<br />
No<br />
No<br />
No<br />
No<br />
No<br />
No
The comparison charts are compiled using information that applies to a large number of health plan users and<br />
is commonly reported by the health plans. Depending on the chart type, such as charts for dental and vision<br />
plans, certain information and/or sections won't appear because the necessary data isn't available. If you have<br />
questions about a topic that isn't covered in the charts, refer to the plan's SPD or contact the health provider's<br />
member services department for additional information. Also, keep in mind that the information on access and<br />
quality of care is provided by the health plans. Neither Huntington Ingalls Industries nor Hewitt Associates is<br />
responsible for the accuracy of this information. If there is a discrepancy between the information displayed on<br />
these charts and the official plan documents, the official plan documents will control. Huntington Ingalls<br />
Industries reserves the right to amend, suspend, or terminate the plan(s) or program(s) at any time.