Account Setup Form - US Endoscopy
Account Setup Form - US Endoscopy
Account Setup Form - US Endoscopy

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
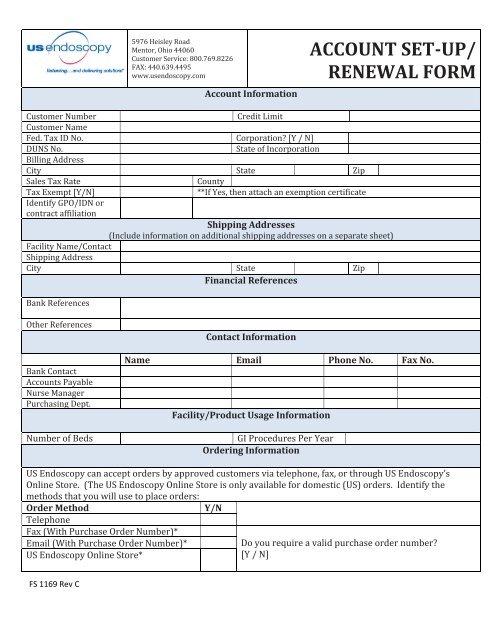
5976 Heisley Road<br />
Mentor, Ohio 44060<br />
Customer Service: 800.769.8226<br />
FAX: 440.639.4495<br />
www.usendoscopy.com<br />
<strong>Account</strong> Information<br />
ACCOUNT SET‐UP/<br />
RENEWAL FORM<br />
Customer Number Credit Limit<br />
Customer Name<br />
Fed. Tax ID No. Corporation? [Y / N]<br />
DUNS No. State of Incorporation<br />
Billing Address<br />
City State Zip<br />
Sales Tax Rate<br />
County<br />
Tax Exempt [Y/N]<br />
Identify GPO/IDN or<br />
contract affiliation<br />
**If Yes, then attach an exemption certificate<br />
Shipping Addresses<br />
(Include information on additional shipping addresses on a separate sheet)<br />
Facility Name/Contact<br />
Shipping Address<br />
City State Zip<br />
Financial References<br />
Bank References<br />
Other References<br />
Bank Contact<br />
<strong>Account</strong>s Payable<br />
Nurse Manager<br />
Purchasing Dept.<br />
Number of Beds<br />
Contact Information<br />
Name Email Phone No. Fax No.<br />
Facility/Product Usage Information<br />
GI Procedures Per Year<br />
Ordering Information<br />
<strong>US</strong> <strong>Endoscopy</strong> can accept orders by approved customers via telephone, fax, or through <strong>US</strong> <strong>Endoscopy</strong>’s<br />
Online Store. (The <strong>US</strong> <strong>Endoscopy</strong> Online Store is only available for domestic (<strong>US</strong>) orders. Identify the<br />
methods that you will use to place orders:<br />
Order Method<br />
Y/N<br />
Telephone<br />
Fax (With Purchase Order Number)*<br />
Email (With Purchase Order Number)*<br />
<strong>US</strong> <strong>Endoscopy</strong> Online Store*<br />
Do you require a valid purchase order number?<br />
[Y / N]<br />
FS 1169 Rev C
1. Remit to address: <strong>US</strong> ENDOSCOPY<br />
<strong>Account</strong>s Receivable<br />
5976 Heisley Road<br />
Mentor, Ohio 44060<br />
Credit Terms and Conditions<br />
2. The Terms and Conditions of Sale that are located on <strong>US</strong> <strong>Endoscopy</strong>’s website (www.usendoscopy.com) will apply<br />
to all product sales unless there is a separate agreement signed by <strong>US</strong> <strong>Endoscopy</strong> and Customer.<br />
3. Credit terms are Net 30 days payable by check or ACH. All invoices over 60 days are past due and subject to a<br />
1.5% finance charge per month.<br />
4. <strong>US</strong> <strong>Endoscopy</strong> reserves the right to not ship products to accounts that are past due or that exceed the established<br />
credit limit.<br />
5. <strong>US</strong> <strong>Endoscopy</strong> reserves the right to make shipments on a COD basis until a past due account has been made<br />
current.<br />
6. All prices listed are F.O.B. shipping point, freight prepaid and added to the invoice. Standard shipment protocol<br />
is FedEx Economy Two‐Day. Applicable taxes will be added unless there is an exemption number or certificate on<br />
file.<br />
7. <strong>US</strong> <strong>Endoscopy</strong>, in its sole discretion, may change its credit policies at any time. Upon acceptance of this<br />
application and the issuance of an open line of credit, you agree to abide by <strong>US</strong> <strong>Endoscopy</strong>’s credit policies.<br />
Applicant hereby agrees that the person signing below has the authority to submit <strong>Account</strong> Set‐<br />
Up/Renewal <strong>Form</strong> and obtain credit from <strong>US</strong> <strong>Endoscopy</strong>. Applicant further provides permission for<br />
<strong>US</strong> <strong>Endoscopy</strong> or its agents to contact the references listed above, or any other source, to obtain<br />
credit information. The creditor, bank, lending institution or other source has the Applicant’s<br />
permission to furnish <strong>US</strong> <strong>Endoscopy</strong> with any and all information requested.<br />
Signature of<br />
Date<br />
Officer, Partner or<br />
Owner<br />
Printed Name<br />
Title<br />
Please allow two (2) business days for processing after the form is received. <strong>US</strong> <strong>Endoscopy</strong>’s normal business hours are Monday through Friday,<br />
8am to 6pm EST. In the event that a form is submitted during a weekend or holiday, the form will be processed beginning on the following<br />
business day.<br />
Date submitted:<br />
FOR <strong>US</strong> ENDOSCOPY <strong>US</strong>E<br />
Approved by:<br />
Name:<br />
Signature:<br />
Date:<br />
FAX THIS ACCOUNT SET‐UP/RENEWAL FORM TO 440.639.4495<br />
FS 1169 Rev C