Camp Wow Medical Form - Saint Patrick Parish
Camp Wow Medical Form - Saint Patrick Parish
Camp Wow Medical Form - Saint Patrick Parish

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
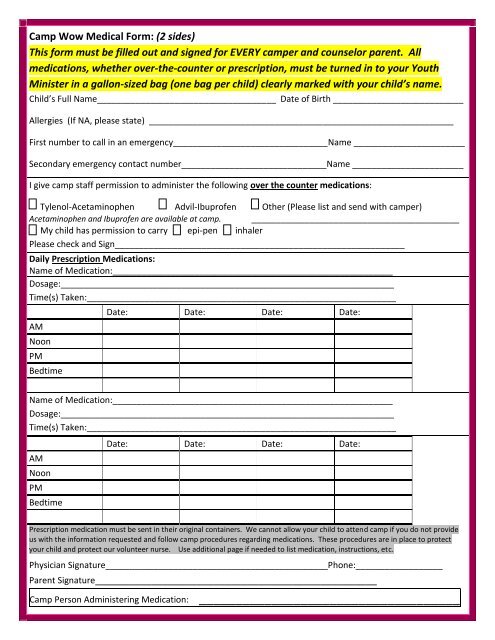
<strong>Camp</strong> <strong>Wow</strong> <strong>Medical</strong> <strong>Form</strong>: (2 sides)<br />
This form must be filled out and signed for EVERY camper and counselor parent. All<br />
medications, whether over-the-counter or prescription, must be turned in to your Youth<br />
Minister in a gallon-sized bag (one bag per child) clearly marked with your child’s name.<br />
Child’s Full Name_____________________________________ Date of Birth ___________________________<br />
Allergies (If NA, please state) _______________________________________________________________<br />
First number to call in an emergency________________________________Name _______________________<br />
Secondary emergency contact number______________________________Name _______________________<br />
I give camp staff permission to administer the following over the counter medications:<br />
Tylenol-Acetaminophen Advil-Ibuprofen Other (Please list and send with camper)<br />
Acetaminophen and Ibuprofen are available at camp. ___________________________________________<br />
My child has permission to carry epi-pen inhaler<br />
Please check and Sign____________________________________________________________<br />
Daily Prescription Medications:<br />
Name of Medication:__________________________________________________________<br />
Dosage:_____________________________________________________________________<br />
Time(s) Taken:________________________________________________________________<br />
AM<br />
Noon<br />
PM<br />
Bedtime<br />
Date: Date: Date: Date:<br />
Name of Medication:__________________________________________________________<br />
Dosage:_____________________________________________________________________<br />
Time(s) Taken:________________________________________________________________<br />
AM<br />
Noon<br />
PM<br />
Bedtime<br />
Date: Date: Date: Date:<br />
Prescription medication must be sent in their original containers. We cannot allow your child to attend camp if you do not provide<br />
us with the information requested and follow camp procedures regarding medications. These procedures are in place to protect<br />
your child and protect our volunteer nurse. Use additional page if needed to list medication, instructions, etc.<br />
Physician Signature______________________________________________Phone:__________________<br />
Parent Signature__________________________________________________<br />
<strong>Camp</strong> Person Administering Medication: ____________________________________
<strong>Camp</strong> <strong>Wow</strong> <strong>Medical</strong> <strong>Form</strong> (2)<br />
_______________________________<br />
My teen’s last tetanus shot was (date)<br />
Insurance Information<br />
Policy in the name of: ______________________________________________________________________<br />
Insurance Company Name: __________________________________________________________________<br />
Please indicate any special instructions, or information we may need in an<br />
emergency:________________________________________________________________________________<br />
__________________________________________________________________________________________<br />
__________________________________________________________________________________________<br />
I fully understand the consequences of and sign this LIABILITY WAIVER AND PERMISSION knowingly, freely,<br />
and willingly.<br />
_______________________________________________________<br />
Signature of Parent or Guardian<br />
Date<br />
Print Name - ____________________________________________<br />
_______________________________________________________<br />
Signature of Youth<br />
Date<br />
Print Name - ____________________________________________<br />
Updated 6/11/12