Issue 31 Spring 2012 - Bases
Issue 31 Spring 2012 - Bases
Issue 31 Spring 2012 - Bases

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Exercise and atrial fibrillation<br />
Dr Gary Brickley provides an overview of this condition, its impact of exercise<br />
tolerance, and considerations for exercise.<br />
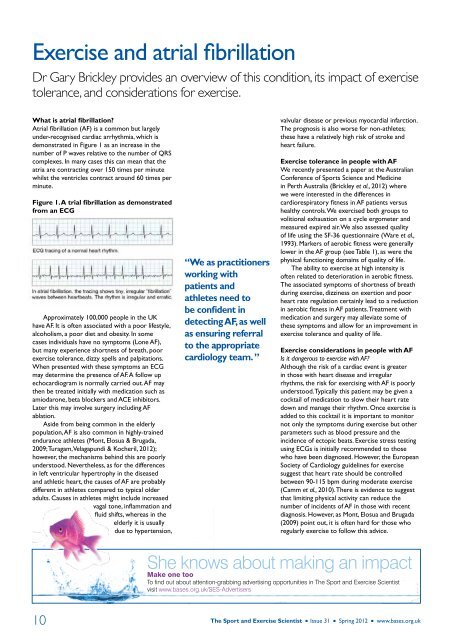
What is atrial fibrillation?<br />
Atrial fibrillation (AF) is a common but largely<br />
under-recognised cardiac arrhythmia, which is<br />
demonstrated in Figure 1 as an increase in the<br />
number of P waves relative to the number of QRS<br />
complexes. In many cases this can mean that the<br />
atria are contracting over 150 times per minute<br />
whilst the ventricles contract around 60 times per<br />
minute.<br />
Figure 1. A trial fibrillation as demonstrated<br />
from an ECG<br />
Approximately 100,000 people in the UK<br />
have AF. It is often associated with a poor lifestyle,<br />
alcoholism, a poor diet and obesity. In some<br />
cases individuals have no symptoms (Lone AF),<br />
but many experience shortness of breath, poor<br />
exercise tolerance, dizzy spells and palpitations.<br />
When presented with these symptoms an ECG<br />
may determine the presence of AF. A follow up<br />
echocardiogram is normally carried out. AF may<br />
then be treated initially with medication such as<br />
amiodarone, beta blockers and ACE inhibitors.<br />
Later this may involve surgery including AF<br />
ablation.<br />
Aside from being common in the elderly<br />
population, AF is also common in highly-trained<br />
endurance athletes (Mont, Elosua & Brugada,<br />
2009; Turagam, Velagapundi & Kocheril, <strong>2012</strong>);<br />
however, the mechanisms behind this are poorly<br />
understood. Nevertheless, as for the differences<br />
in left ventricular hypertrophy in the diseased<br />
and athletic heart, the causes of AF are probably<br />
different in athletes compared to typical older<br />
adults. Causes in athletes might include increased<br />
vagal tone, inflammation and<br />
fluid shifts, whereas in the<br />
elderly it is usually<br />
due to hypertension,<br />
“We as practitioners<br />
working with<br />
patients and<br />
athletes need to<br />
be confident in<br />
detecting AF, as well<br />
as ensuring referral<br />
to the appropriate<br />
cardiology team. ”<br />
valvular disease or previous myocardial infarction.<br />
The prognosis is also worse for non-athletes;<br />
these have a relatively high risk of stroke and<br />
heart failure.<br />
Exercise tolerance in people with AF<br />
We recently presented a paper at the Australian<br />
Conference of Sports Science and Medicine<br />
in Perth Australia (Brickley et al., <strong>2012</strong>) where<br />
we were interested in the differences in<br />
cardiorespiratory fitness in AF patients versus<br />
healthy controls. We exercised both groups to<br />
volitional exhaustion on a cycle ergometer and<br />
measured expired air. We also assessed quality<br />
of life using the SF-36 questionnaire (Ware et al.,<br />
1993). Markers of aerobic fitness were generally<br />
lower in the AF group (see Table 1), as were the<br />
physical functioning domains of quality of life.<br />
The ability to exercise at high intensity is<br />
often related to deterioration in aerobic fitness.<br />
The associated symptoms of shortness of breath<br />
during exercise, dizziness on exertion and poor<br />
heart rate regulation certainly lead to a reduction<br />
in aerobic fitness in AF patients. Treatment with<br />
medication and surgery may alleviate some of<br />
these symptoms and allow for an improvement in<br />
exercise tolerance and quality of life.<br />
Exercise considerations in people with AF<br />
Is it dangerous to exercise with AF?<br />
Although the risk of a cardiac event is greater<br />
in those with heart disease and irregular<br />
rhythms, the risk for exercising with AF is poorly<br />
understood. Typically this patient may be given a<br />
cocktail of medication to slow their heart rate<br />
down and manage their rhythm. Once exercise is<br />
added to this cocktail it is important to monitor<br />
not only the symptoms during exercise but other<br />
parameters such as blood pressure and the<br />
incidence of ectopic beats. Exercise stress testing<br />
using ECGs is initially recommended to those<br />
who have been diagnosed. However, the European<br />
Society of Cardiology guidelines for exercise<br />
suggest that heart rate should be controlled<br />
between 90-115 bpm during moderate exercise<br />
(Camm et al., 2010). There is evidence to suggest<br />
that limiting physical activity can reduce the<br />
number of incidents of AF in those with recent<br />
diagnosis. However, as Mont, Elosua and Brugada<br />
(2009) point out, it is often hard for those who<br />
regularly exercise to follow this advice.<br />
She knows about making an impact<br />
Make one too<br />
To find out about attention-grabbing advertising opportunities in The Sport and Exercise Scientist<br />
visit www.bases.org.uk/SES-Advertisers<br />
10 The Sport and Exercise Scientist n <strong>Issue</strong> <strong>31</strong> n <strong>Spring</strong> <strong>2012</strong> n www.bases.org.uk