-54- Binocular Vision & Inferior Oblique Muscle Palsy with ‘Paradoxical’ V-Pattern Strabismus FIRST Quarter of 2011 Strabology Quarterly© E. Khawam, MD and D. Fahed, MD Volume 26 (No.1) A Medical Scientific e-Periodical Pages 51-60
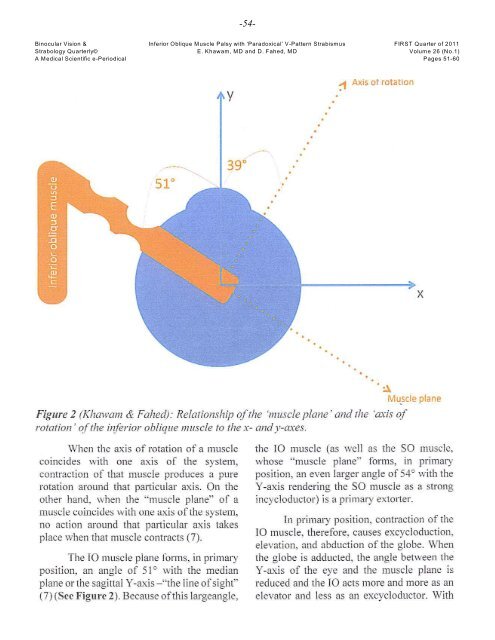
-55- Binocular Vision & Inferior Oblique Muscle Palsy with ‘Paradoxical’ V-Pattern Strabismus FIRST Quarter of 2011 Strabology Quarterly© E. Khawam, MD and D. Fahed, MD Volume 26 (No.1) A Medical Scientific e-Periodical Pages 51-60 abduction of the eye, the angle between the Y- axis of the globe and the muscle plane increases. Therefore the IO produces, increasingly, an excycloduction. Since the IO muscle is an excycloductor, an elevator, and an abductor, its paralysis therefore results in weakness of these three components: 1. Torsional Deviation: The result is an intorsion of the eye. However, the absence of incyclotropia could be due to cyclofusion, or to monocular sensory adaptation whereby a reordering of the spatial response of the retinal elements along new vertical and horizontal retinal meridians, analogous to abnormal retinal correspondence (ARC). It can also be due to spread of comitance to the synergistic muscle (8) which has an opposite torsional movement: the SR muscle that has a secondary incycloduction movement. 2. Vertical Deviation: The paretic eye is hypotropic if the uninvolved eye fixates. If the involved eye fixates, a hypertropia of the uninvolved eye is present. The hypotropia may become especially pronounced in adduction and depression, associated in such instances with overaction/contracture of its direct antagonist, the SO muscle. 3. Horizontal Deviation: The normal abducting effect of the IO muscle is greatest in upgaze. Its paralysis, therefore, results in greater esodeviation in upgaze. And, with increasing abducting action, mainly in downgaze, of its antagonist, the SO muscle, an A-pattern esodeviation is encountered. An A-pattern exodeviation, not infrequently encountered, may develop due to the marked overaction of the SO muscle(s). 4. Findings on Rotations: Weakness of the vertical action of the IO muscle, especially in the adduction position is found. However minimal weakness on rotation does not rule out the diagnosis of IO palsy. a. Overaction of its direct antagonist: the SO muscle. A prominent finding that, in my experience, is always present. b. Overaction of the yoke muscle: the SR muscle of the opposite eye. In case the affected eye is fixating in adduction, a “Rising eye phenomenon” of the fellow eye is seen in abduction. c. Underaction of the yoke of the antagonist: described by Chavasse (3) as “Inhibitional palsy of the contralateral antagonist”, the IR muscle of the opposite eye. 5. Associated Secondary Mechanical Anomalies: With time, vergence-adaptation followed by muscle-length-adaptation take place: the innervationally-overacting muscles shorten with actual loss of sarcomeres resulting in contractures with structural and fascial restrictions; and the inhibitionally pseudo-palsied muscle(s) elongate with actual increased number of sarcomeres (9). 6. Habitual Head Postures: a: Head Tilt: to the ipsilateral shoulder so that the affected IO muscle is put at rest and the tonic impulses, sent by the otolith apparatus will not have a direct action on it. Head tilt –we believe- is usually a compensatory mechanism to reduce the vertical deviation rather than the torsional one, and thus to gain fusion (10).