

January/February - West Virginia State Medical Association
January/February - West Virginia State Medical Association
January/February - West Virginia State Medical Association

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
| Scientific Article<br />
Melkersson-Rosenthal Syndrome with Migraine-Like<br />
Headaches Treated With Minocycline: A Case Report<br />
and Review of the Literature<br />
Matthew A. Hazey, BS<br />
<strong>Medical</strong> Student<br />
Anthony J. Van Norman, MD<br />
Resident, Section of Dermatology<br />
Drury L. Armistead, MD<br />
Assistant Professor, Section of<br />
Dermatology<br />
<strong>West</strong> <strong>Virginia</strong> University School of Medicine,<br />
Morgantown<br />
Abstract<br />
Cheilitis granulomatosa (CG), which<br />
presents clinically as persistent lip<br />
swelling, is characterized histologically by<br />
noncaseating granulomatous<br />
inflammation of unknown origin. CG may<br />
also be part of the classic triad of the<br />
Melkersson-Rosenthal Syndrome (MRS)<br />
and alone is considered by some to be an<br />
oligosymptomatic form of MRS. We report<br />
a case of CG associated with migrainelike<br />
headaches in a 44-year-old woman.<br />
The clinical presentation, histologic<br />
findings, and subsequent treatment are<br />
described. A brief review of the literature<br />
also is provided.<br />
left side (Figure 1). The patient’s<br />
symptoms were initially intermittent<br />
but became persistent. She gave a<br />
history of severe headaches that<br />
were temporally related to increased<br />
swelling of her upper lip. She was<br />
otherwise well and denied symptoms<br />
in any other organ system. Further,<br />
the patient denied a history of any<br />
drug ingestion, nor could she recall<br />
any provocative factors such as foods,<br />
contactants, or activities. Physical<br />
examination revealed soft, nonpitting<br />
edema of the upper lip, left<br />
greater than right, with overlying<br />
erythema. The tongue was normal<br />
in appearance, and there were no<br />
findings consistent with facial nerve<br />
paralysis. Serologic evaluation<br />
including complete blood count,<br />
C1 esterase inhibitor, C3, C4, serum<br />
angiotensin-converting enzyme<br />
level, and antinuclear antibody were<br />
within normal limits. Chest x-ray and<br />
magnetic resonance imaging of the<br />
brain and sinuses were performed<br />
and found to be within normal limits.<br />
A 4-mm punch biopsy specimen<br />
from the cutaneous upper lip showed<br />
scattered noncaseating granulomas,<br />
mild edema, lymphectasia, as well<br />
as superficial and deep perivascular<br />
lymphocytic inflammation (Figures<br />
2 and 3). Special stains were<br />
negative for evidence of fungi or<br />
acid-fast bacilli. No foreign bodies<br />
were seen on examination of the<br />
specimen under polarized light.<br />
Treatment was initiated with<br />
minocycline hydrochloride,100mg,<br />
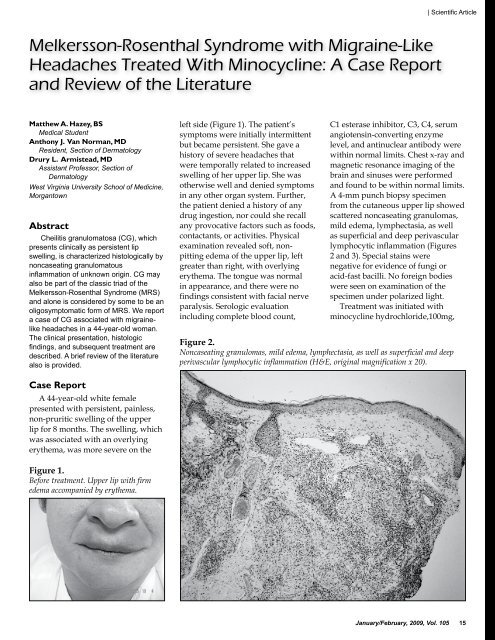
Figure 2.<br />
Noncaseating granulomas, mild edema, lymphectasia, as well as superficial and deep<br />
perivascular lymphocytic inflammation (H&E, original magnification x 20).<br />
Case Report<br />
A 44-year-old white female<br />
presented with persistent, painless,<br />
non-pruritic swelling of the upper<br />
lip for 8 months. The swelling, which<br />
was associated with an overlying<br />
erythema, was more severe on the<br />
Figure 1.<br />
Before treatment. Upper lip with firm<br />
edema accompanied by erythema.<br />
<strong>January</strong>/<strong>February</strong>, 2009, Vol. 105 15












