In this issue - The American Academy of Dental Sleep Medicine
In this issue - The American Academy of Dental Sleep Medicine
In this issue - The American Academy of Dental Sleep Medicine

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
ISSUE 4 | 2013 21<br />
mm. Her mandible deviates to the right approximately 2 mm at full<br />
opening. Her midlines are not coincident: her mandibular midline<br />
sits 2.5 mm to the right <strong>of</strong> her maxillary midline in habitual closure.<br />
<strong>The</strong> patient’s oral examination revealed generalized abfractions,<br />
some <strong>of</strong> which had been restored. <strong>The</strong> longer clinical crown length<br />
<strong>of</strong> the teeth secondary to attachment loss creates more potential<br />
for cervical flexing stress and loss <strong>of</strong> cervical tooth structure.<br />
Gingival recession has developed on teeth #2, 3, 4, 5, 7, 9, 10, 11,<br />
12, 13, 14, 15, 18, 19, 20, 21, 28, 29 and 31. Her anterior teeth<br />
reflect an incisal wear pattern. <strong>The</strong> patient is missing teeth #1, 16,<br />
17 and 30. Her full mouth series <strong>of</strong> x-rays showed generalized<br />
periodontal attachment loss (osseous and gingival). A Miller’s Class<br />
1 mobility was recorded for teeth # 23, 24, 25 and 26. She opens<br />
with a 2 mm deflection to the right at full opening. Her overbite<br />
measures 3 mm, and her overjet measures 5 mm. Her oral cancer<br />
screening was negative.<br />
<strong>The</strong> patient presented with a Class II (retruded lower jaw) dental<br />
relationship on the right side and a Class I (normal) dental<br />
relationship on the left side. She had significant open contacts<br />
between teeth #10 and 11, 12 and 13 and 24 and 25. We examined<br />
her in the late afternoon, at that time <strong>of</strong> day she had no tenderness<br />
or pain <strong>of</strong> the masticatory or TMJ regions. Stethoscopic evaluation<br />
<strong>of</strong> her joints revealed slight crepitus upon opening on both sides.<br />
Her neck muscles are stiff every day and she has pain with cervical<br />
rotation on her left side. She refused further TMJ or cephalometric<br />
x-rays.<br />
Diagnosis<br />
Per OCST, the sleep physician diagnosed the patient as follows:<br />
1. Snoring<br />
2. Severe Obstructive <strong>Sleep</strong> Apnea Syndrome<br />
AHI - 37.5<br />
Supine AHI – 53.9<br />
Lowest Desat - 70.0<br />
RDI – 52.4<br />
Non – Supine AHI –<br />
Percent Below 90% - 5.6%<br />
Decision Tree<br />
I selected an Elastic Mandibular Appliance (EMA) for <strong>this</strong> patient.<br />
<strong>The</strong> EMA has upper and lower vacuform polycarbonate trays<br />
connected with forgiving stretchable straps that button onto the<br />
trays. <strong>The</strong> straps come in nine different lengths for changing or<br />
titrating protrusion, each strap numbered according to its length in<br />
millimeters. <strong>In</strong> addition, each numbered strap is available in four<br />
different color-coded elastic strengths or tensions or 36 total straps<br />
in all. Patients usually start with a s<strong>of</strong>ter strap and move to a firmer<br />
strap as their joints permit. This variable strap design <strong>of</strong> the EMA<br />
allowed for customized lateral movement and joint care that <strong>this</strong><br />
patient needed and allowed her jaw to move to its excursive posture.<br />
We delivered the EMA and she wore it for two weeks with the size<br />
17mm length straps on both sides in yellow (moderate stretch).<br />
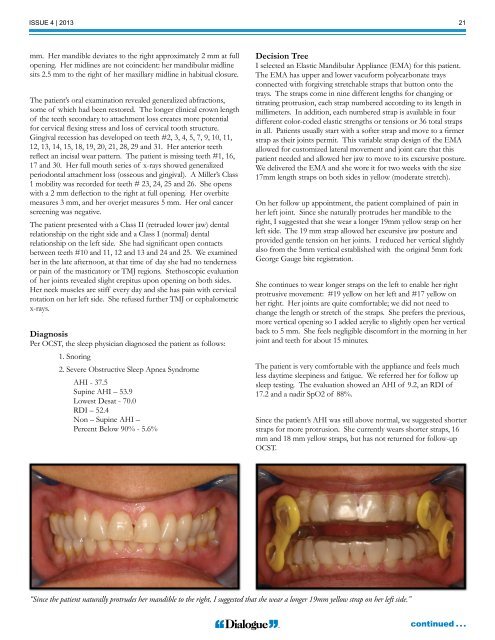
On her follow up appointment, the patient complained <strong>of</strong> pain in<br />
her left joint. Since she naturally protrudes her mandible to the<br />
right, I suggested that she wear a longer 19mm yellow strap on her<br />
left side. <strong>The</strong> 19 mm strap allowed her excursive jaw posture and<br />
provided gentle tension on her joints. I reduced her vertical slightly<br />
also from the 5mm vertical established with the original 5mm fork<br />
George Gauge bite registration.<br />
She continues to wear longer straps on the left to enable her right<br />
protrusive movement: #19 yellow on her left and #17 yellow on<br />
her right. Her joints are quite comfortable; we did not need to<br />
change the length or stretch <strong>of</strong> the straps. She prefers the previous,<br />
more vertical opening so I added acrylic to slightly open her vertical<br />
back to 5 mm. She feels negligible discomfort in the morning in her<br />
joint and teeth for about 15 minutes.<br />
<strong>The</strong> patient is very comfortable with the appliance and feels much<br />
less daytime sleepiness and fatigue. We referred her for follow up<br />
sleep testing. <strong>The</strong> evaluation showed an AHI <strong>of</strong> 9.2, an RDI <strong>of</strong><br />
17.2 and a nadir SpO2 <strong>of</strong> 88%.<br />
Since the patient’s AHI was still above normal, we suggested shorter<br />
straps for more protrusion. She currently wears shorter straps, 16<br />
mm and 18 mm yellow straps, but has not returned for follow-up<br />
OCST.<br />
“Since the patient naturally protrudes her mandible to the right, I suggested that she wear a longer 19mm yellow strap on her left side.”<br />
continued . . .