

Download pdf - aagbi
Download pdf - aagbi
Download pdf - aagbi

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
10<br />
staff responsible for all aspects of scrubbing,<br />
cleaning and autoclaving. They also worked<br />
in the minor theatre where suturing and<br />
dressing changes were performed as well as<br />
acting as anaesthetic assistants.<br />
Operating theatre<br />
Our surgical workload was largely<br />
determined by how much equipment was<br />
available at a given time. The average was<br />
about 110 cases per month but we<br />
sometimes had to stop all elective<br />
procedures when supplies were running low.<br />
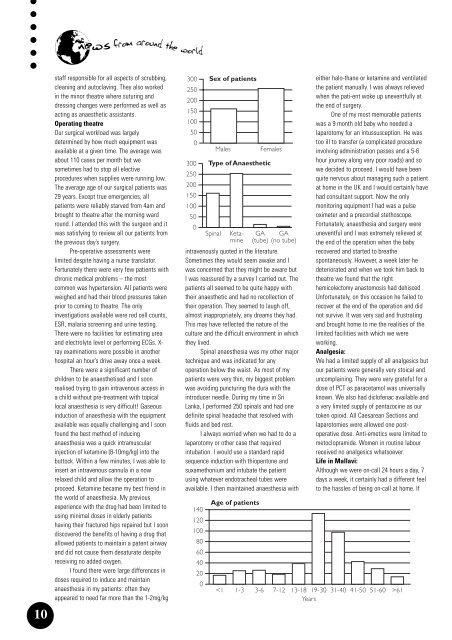
The average age of our surgical patients was<br />
29 years. Except true emergencies, all<br />
patients were reliably starved from 4am and<br />
brought to theatre after the morning ward<br />
round. I attended this with the surgeon and it<br />
was satisfying to review all our patients from<br />
the previous day’s surgery.<br />
Pre-operative assessments were<br />
limited despite having a nurse translator.<br />
Fortunately there were very few patients with<br />
chronic medical problems – the most<br />
common was hypertension. All patients were<br />
weighed and had their blood pressures taken<br />
prior to coming to theatre. The only<br />
investigations available were red cell counts,<br />
ESR, malaria screening and urine testing.<br />
There were no facilities for estimating urea<br />
and electrolyte level or performing ECGs. X-<br />
ray examinations were possible in another<br />
hospital an hour’s drive away once a week.<br />
There were a significant number of<br />
children to be anaesthetised and I soon<br />
realised trying to gain intravenous access in<br />
a child without pre-treatment with topical<br />
local anaesthesia is very difficult! Gaseous<br />
induction of anaesthesia with the equipment<br />
available was equally challenging and I soon<br />
found the best method of inducing<br />
anaesthesia was a quick intramuscular<br />
injection of ketamine (8-10mg/kg) into the<br />
buttock. Within a few minutes, I was able to<br />
insert an intravenous cannula in a now<br />
relaxed child and allow the operation to<br />
proceed. Ketamine became my best friend in<br />
the world of anaesthesia. My previous<br />
experience with the drug had been limited to<br />
using minimal doses in elderly patients<br />
having their fractured hips repaired but I soon<br />
discovered the benefits of having a drug that<br />
allowed patients to maintain a patent airway<br />
and did not cause them desaturate despite<br />
receiving no added oxygen.<br />
I found there were large differences in<br />
doses required to induce and maintain<br />
anaesthesia in my patients: often they<br />
appeared to need far more than the 1-2mg/kg<br />
300 Sex of patients<br />
250<br />
200<br />
150<br />
100<br />
50<br />
0<br />
300<br />
250<br />
200<br />
150<br />
100<br />
50<br />
0<br />
intravenously quoted in the literature.<br />
Sometimes they would seem awake and I<br />
was concerned that they might be aware but<br />
I was reassured by a survey I carried out. The<br />
patients all seemed to be quite happy with<br />
their anaesthetic and had no recollection of<br />
their operation. They seemed to laugh off,<br />
almost inappropriately, any dreams they had.<br />
This may have reflected the nature of the<br />
culture and the difficult environment in which<br />
they lived.<br />
Spinal anaesthesia was my other major<br />
technique and was indicated for any<br />
operation below the waist. As most of my<br />
patients were very thin, my biggest problem<br />
was avoiding puncturing the dura with the<br />
introducer needle. During my time in Sri<br />
Lanka, I performed 250 spinals and had one<br />
definite spinal headache that resolved with<br />
fluids and bed rest.<br />
I always worried when we had to do a<br />
laparotomy or other case that required<br />
intubation. I would use a standard rapid<br />
sequence induction with thiopentone and<br />
suxamethonium and intubate the patient<br />
using whatever endotracheal tubes were<br />
available. I then maintained anaesthesia with<br />
140<br />
120<br />
100<br />
80<br />
60<br />
40<br />
20<br />
0<br />
Spinal<br />
Males<br />
Age of patients<br />
61<br />
Years














