Importance of Crown to Root and Crown to Implant ... - DentalCEToday
Importance of Crown to Root and Crown to Implant ... - DentalCEToday
Importance of Crown to Root and Crown to Implant ... - DentalCEToday

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Continuing Education<br />
Course Number: 135<br />
<strong>Importance</strong> <strong>of</strong> <strong>Crown</strong> <strong>to</strong> <strong>Root</strong><br />
<strong>and</strong> <strong>Crown</strong> <strong>to</strong> <strong>Implant</strong> Ratios<br />
Authored by Gary Greenstein, DDS, MS, <strong>and</strong><br />
John S. Cavallaro Jr, DDS<br />
Upon successful completion <strong>of</strong> this CE activity 2 CE credit hours may be awarded<br />
A Peer-Reviewed CE Activity by<br />
Dentistry Today, Inc, is an ADA CERP Recognized Provider. ADA CERP is<br />
a service <strong>of</strong> the American Dental Association <strong>to</strong> assist dental pr<strong>of</strong>essionals<br />
in indentifying quality providers <strong>of</strong> continuing dental education. ADA CERP<br />
does not approve or endorse individual courses or instruc<strong>to</strong>rs, nor does it<br />
imply acceptance <strong>of</strong> credit hours by boards <strong>of</strong> dentistry. Concerns or<br />
complaints about a CE provider may be directed <strong>to</strong> the provider or <strong>to</strong><br />
ADA CERP at ada.org/go<strong>to</strong>/cerp.<br />
Approved PACE Program Provider<br />
FAGD/MAGD Credit Approval<br />
does not imply acceptance<br />
by a state or provincial board <strong>of</strong><br />
dentistry or AGD endorsement.<br />
June 1, 2009 <strong>to</strong> May 31, 2012<br />
AGD Pace approval number: 309062<br />
Opinions expressed by CE authors are their own <strong>and</strong> may not reflect those <strong>of</strong> Dentistry Today. Mention <strong>of</strong><br />
specific product names does not infer endorsement by Dentistry Today. Information contained in CE articles <strong>and</strong><br />
courses is not a substitute for sound clinical judgment <strong>and</strong> accepted st<strong>and</strong>ards <strong>of</strong> care. Participants are urged <strong>to</strong><br />
contact their state dental boards for continuing education requirements.
<strong>Importance</strong> <strong>of</strong> <strong>Crown</strong> <strong>to</strong> <strong>Root</strong><br />
<strong>and</strong> <strong>Crown</strong> <strong>to</strong> <strong>Implant</strong> Ratios<br />
Effective Date: 03/1/2011 Expiration Date: 03/1/2013<br />
LEARNING OBJECTIVES<br />
After reading this article, the individual will learn:<br />
• The clinical importance <strong>of</strong> crown <strong>to</strong> root ratios (CRRs)<br />
<strong>and</strong> crown <strong>to</strong> implant ratios (CIRs).<br />
• Suggestions for res<strong>to</strong>ring teeth <strong>and</strong> implants based on<br />
a search <strong>of</strong> the literature focusing on CRRs <strong>and</strong> CIRs.<br />
ABOUT THE AUTHORS<br />
Dr. Greenstein is clinical pr<strong>of</strong>essor,<br />
Department <strong>of</strong> Periodon<strong>to</strong>logy, College<br />
<strong>of</strong> Dental Medicine, Columbia University;<br />
Private Practice, Surgical Implan<strong>to</strong>logy<br />
<strong>and</strong> Periodontics, Freehold, NJ. He is a<br />
board Diplomate <strong>and</strong> Fellow <strong>of</strong> the<br />
American Academy <strong>of</strong> Periodon<strong>to</strong>logy, <strong>and</strong> has authored<br />
more than 100 articles on periodontal <strong>and</strong> implant therapy.<br />
He can be reached via e-mail at ggperio@aol.com.<br />
Disclosure: Dr. Greenstein reports no disclosures.<br />
Dr. Cavallaro is clinical direc<strong>to</strong>r <strong>of</strong> the<br />
<strong>Implant</strong> Fellowship Program, College <strong>of</strong><br />
Dental Medicine, Columbia University,<br />
New York, NY; private practice, surgical<br />
implan<strong>to</strong>logy <strong>and</strong> prosthodontics, Brooklyn,<br />
NY. He is a member <strong>of</strong> the Academy<br />
<strong>of</strong> Osseointegration <strong>and</strong> a former Fellow <strong>of</strong> the Greater New<br />
York Academy <strong>of</strong> Prosthodontics. He can be reached at<br />
docsamurai@si.rr.com.<br />
Disclosure: Dr. Cavallaro reports no disclosures.<br />
INTRODUCTION<br />
His<strong>to</strong>rically, crown <strong>to</strong> root ratios (CRRs) <strong>of</strong> teeth were used<br />
as a parameter <strong>to</strong> help decide if teeth should be res<strong>to</strong>red<br />
with or without splinting <strong>to</strong> adjacent teeth or employed as<br />
Continuing Education<br />
Recommendations for Fluoride Varnish Use in Caries Management<br />
abutments in dental prostheses. However, guidelines were<br />
based upon empiricisms rather than scientific data. This<br />
resulted in teeth being extracted that could have been<br />
retained. With respect <strong>to</strong> dental implants, the desire <strong>to</strong><br />
reduce crown <strong>to</strong> implant ratios (CIRs) could result in an<br />
area being unnecessarily bone augmented <strong>to</strong> provide<br />
additional support for a longer implant. Therefore, it would<br />
be advantageous if an assessment <strong>of</strong> the dental literature<br />
provided guidance as <strong>to</strong> the survival <strong>of</strong> res<strong>to</strong>red teeth <strong>and</strong><br />
implants with elevated crown <strong>to</strong> root or CIRs.<br />
Fixed denture prostheses (FDPs) can be retained by<br />
teeth, dental implants, or a combination <strong>of</strong> both. In either<br />
scenario, a FDP needs an adequate number <strong>and</strong> size <strong>of</strong><br />
abutments <strong>to</strong> provide support for a res<strong>to</strong>ration. The number<br />
<strong>of</strong> abutments <strong>to</strong> retain a prosthesis is dependent on<br />
numerous clinical variables, including size <strong>and</strong> design <strong>of</strong><br />
the prosthesis, number <strong>of</strong> missing teeth, occlusal <strong>and</strong><br />
parafunctional forces, opposing dentition, amount <strong>of</strong><br />
available bone around abutments, <strong>and</strong> cost. With respect <strong>to</strong><br />
providing adequate support for a prosthesis, the issue <strong>of</strong><br />
root or implant length needs <strong>to</strong> be considered.<br />
The objective <strong>of</strong> this article is <strong>to</strong> discuss the importance<br />
<strong>of</strong> CRRs <strong>and</strong> CIRs based on a search <strong>of</strong> the literature<br />
focusing on 4 overlapping <strong>to</strong>pics: (1) relevance <strong>of</strong> Ante’s law<br />
<strong>to</strong> reconstructive dentistry, (2) CRR <strong>and</strong> CIRs, (3) the utility<br />
<strong>of</strong> short versus long dental implants, <strong>and</strong> (4) the concept <strong>of</strong><br />
vertical cantilevers.<br />
ANTE’S LAW<br />
In 1926, it was suggested that the <strong>to</strong>tal periodontal<br />
membrane area <strong>of</strong> abutment teeth must equal or exceed<br />
the membrane area <strong>of</strong> teeth <strong>to</strong> be replaced. 1 This was<br />
referred <strong>to</strong> as Ante’s Law, but it actually was an opinion that<br />
was never scientifically validated. Unfortunately, application<br />
<strong>of</strong> this concept precluded employing numerous teeth as<br />
abutments, because they had lost periodontal support.<br />
Thus, teeth were extracted that might have had a better<br />
prognosis than expected. 2 In this regard, a systematic<br />
review (6 publications) by Lulic, et al 3 surveyed the<br />
literature from 1966 <strong>to</strong> 2006. They evaluated the survival <strong>of</strong><br />
FDPs when periodontally healthy teeth whose periodontium<br />
was severely reduced were incorporated in<strong>to</strong> prostheses.<br />
To be included in the review the res<strong>to</strong>rations had <strong>to</strong> be in<br />
1
Continuing Education<br />
<strong>Importance</strong> <strong>of</strong> <strong>Crown</strong> <strong>to</strong> <strong>Root</strong> <strong>and</strong> <strong>Crown</strong> <strong>to</strong> <strong>Implant</strong> Ratios<br />
function for 5 years. While not specifically stated in the text,<br />
it is reasonable <strong>to</strong> presume that teeth with reduced<br />
periodontiums incorporated in<strong>to</strong> FDPs <strong>of</strong>ten demonstrate<br />
increased CRRs. Lulic, et al 3 reported that among 579<br />
FDPs, the survival rate was 96.4% <strong>and</strong> 92.9% after 5 years<br />
<strong>and</strong> 10 years, respectively. These findings are similar <strong>to</strong><br />
data concerning survival <strong>of</strong> FDPs fabricated on teeth with<br />
good periodontal support. 4,5<br />
In summary, considering the data from long-term<br />
clinical trials, it can be concluded that the concept referred<br />
<strong>to</strong> as Ante’s Law with respect <strong>to</strong> teeth has been refuted.<br />
Furthermore, since teeth <strong>and</strong> implants are retained by 2<br />
different mechanisms (periodontal ligament versus<br />
osseointegration), the concept <strong>of</strong> extrapolating guidelines<br />
for patient care with one type <strong>of</strong> support <strong>to</strong> the other would<br />
be inappropriate.<br />
CROWN TO ROOT RATIOS AND CROWN TO IMPLANT<br />
RATIOS<br />
Teeth<br />
Frequently, the CRR is used <strong>to</strong> determine if a <strong>to</strong>oth could<br />
function as a suitable abutment. The term refers <strong>to</strong> a ratio<br />
calculated from a radiograph with respect <strong>to</strong> length <strong>of</strong> the<br />
<strong>to</strong>oth not within bone divided by the portion <strong>of</strong> the <strong>to</strong>oth in<br />
alveolar bone. 6 When forces are applied <strong>to</strong> a single-rooted<br />
<strong>to</strong>oth with a complete periodontium, the <strong>to</strong>oth’s center <strong>of</strong><br />
rotation, or fulcrum, is in the center <strong>of</strong> the root, two thirds<br />
down the root within the bone. 6 The main reason for<br />
increased CRRs is fabrication <strong>of</strong> taller crowns on teeth or<br />
pontics subsequent <strong>to</strong> alveolar bone loss. This results in the<br />
crown portion <strong>of</strong> the prosthesis providing a greater lever arm<br />
<strong>and</strong> the root providing less resistance. When there is<br />
additional bone loss, the center <strong>of</strong> rotation moves apically. 6<br />
With regard <strong>to</strong> CRRs discussed in the literature, a variety<br />
<strong>of</strong> ratios were reported. Ideally, the ratio should be 1:2 or 0.5;<br />
however, this is rarely seen in clinical practice. 7 Dykema, et<br />
al 7 indicated that a CRR <strong>of</strong> 1:1.5 is desirable. Similarly,<br />
Shillingburg, et al 8 suggested a 1:1.5 ratio as most favorable<br />
for an abutment <strong>and</strong> a CRR <strong>of</strong> 1:1 as a minimum for a <strong>to</strong>oth<br />
abutment. Several procedures alter the CRR as follows:<br />
overdentures with a small attachment 9 <strong>and</strong> extrusion <strong>of</strong> teeth<br />
<strong>to</strong> provide additional bone both decrease the CRR, whereas<br />
an increase in vertical dimension <strong>of</strong> occlusion <strong>and</strong> surgical<br />
crown lengthening or ridge reduction <strong>to</strong> make room for an<br />
implant abutment increase the CRR. 6 After assessing the<br />
literature, Grossmann <strong>and</strong> Sadan 6 concluded that no<br />
definitive recommendations could be established for an<br />
optimal CRR concerning teeth.<br />
To compensate for increased forces on prostheses due<br />
<strong>to</strong> increased CRRs, clinicians have splinted teeth<br />
<strong>to</strong>gether. 10 This may shift the center <strong>of</strong> rotation <strong>and</strong> transmit<br />
less horizontal forces <strong>to</strong> individual abutments or alter the<br />
response <strong>to</strong> the applied forces. 11,12 However, no objective<br />
criteria exist <strong>to</strong> define the need or extent <strong>of</strong> splinting <strong>to</strong><br />
assuage the effect <strong>of</strong> an increased CRR. 13<br />
Dental <strong>Implant</strong>s<br />
A consensus conference defined a desirable crown height<br />
space for a fixed prosthesis <strong>to</strong> be between 8 <strong>to</strong> 12 mm<br />
(bone level <strong>to</strong> opposing dentition). 14 This height leaves 3<br />
mm for s<strong>of</strong>t tissue (includes biologic width <strong>and</strong> s<strong>of</strong>t-tissue<br />
coverage <strong>of</strong> implant collar), 2 mm for occlusal porcelain,<br />
<strong>and</strong> an abutment ≥ 5-mm high. However, it was cautioned<br />
as the height <strong>of</strong> the prosthesis increases there is increased<br />
risk <strong>of</strong> component <strong>and</strong> material fracture due <strong>to</strong> elevated<br />
forces on the res<strong>to</strong>ration. 14 Therefore, increased crown<br />
height should be considered as a fac<strong>to</strong>r that can affect<br />
clinical outcomes both technically <strong>and</strong> biologically.<br />
In this regard, a projected increased CIR can be reduced<br />
by increasing the bone height surgically with ridge<br />
augmentation or distraction osteogenesis. On the other h<strong>and</strong>,<br />
if increased CIRs were proven <strong>to</strong> be safe <strong>to</strong> use, it would<br />
provide a variety <strong>of</strong> advantages including avoiding some<br />
guided bone regeneration procedures, abridged treatment<br />
time, facilitating a greater number <strong>of</strong> patients <strong>to</strong> be treated,<br />
<strong>and</strong> decreased fees. Therefore, the literature was searched<br />
<strong>to</strong> determine if increased CIRs enhance therapy or induce<br />
additional stress that eventually has a deleterious effect on<br />
bone adjacent <strong>to</strong> implants supporting prostheses or<br />
prostheses’ components.<br />
PERFORMANCE OF IMPLANTS WITH RESPECT TO<br />
CROWN TO IMPLANT RATIOS<br />
An elevated CIR has been described as a type <strong>of</strong> nonaxial<br />
loading, which can detrimentally affect a prosthesis<br />
2
Continuing Education<br />
<strong>Importance</strong> <strong>of</strong> <strong>Crown</strong> <strong>to</strong> <strong>Root</strong> <strong>and</strong> <strong>Crown</strong> <strong>to</strong> <strong>Implant</strong> Ratios<br />
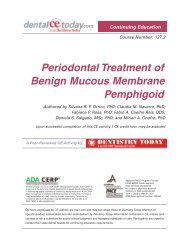
(Figure 1). 15,16 Ten studies were found in the dental<br />
literature that addressed the survivability <strong>of</strong> implants in<br />
relation <strong>to</strong> CIRs (Table 1). 17-26 Seven investigations are<br />
succinctly addressed, because they all have different<br />
characteristics; the latter 3 pertain <strong>to</strong> cantilevered prostheses<br />
<strong>and</strong> the data are summarized in Table 1.<br />
Schulte, et al 17 assessed survival <strong>of</strong> 889 res<strong>to</strong>rations in<br />
more than an average <strong>of</strong> 2.3 years (range 0.1 <strong>to</strong> 7.4 years).<br />
The average survival rate was 98.2%, <strong>and</strong> these implants<br />
(Bicon) had a mean CIR <strong>of</strong> 1.3 (range 0.5:1 <strong>to</strong> 3:1). More<br />
than 400 prostheses had a CIR ≥ 1.2. Among the 889<br />
res<strong>to</strong>rations that were moni<strong>to</strong>red, 16 implants failed, <strong>and</strong><br />
these prostheses manifested a mean CIR ratio <strong>of</strong> 1.4.<br />
Similarity <strong>of</strong> CIRs between failed <strong>and</strong> successful implants<br />
implies that the crown <strong>to</strong> implant ratio was not a critical<br />
determinant with respect <strong>to</strong> implant survival.<br />
Concerning the relationship between CIR <strong>and</strong> bone loss<br />
around implants, Tawil <strong>and</strong> Younan 18 evaluated 262 machined<br />
surfaced implants (Brånemark) in 109 patients in more than 53<br />
months. Bone loss was not related <strong>to</strong> CIRs <strong>and</strong> the survival rate<br />
<strong>of</strong> res<strong>to</strong>red implants was 99.9%. The reported CIRs <strong>and</strong> the<br />
number <strong>of</strong> cases (in brackets) were as follows: 2 (8).<br />
Blanes, et al 19 appraised the impact <strong>of</strong> CIRs on the<br />
survival <strong>of</strong> rough surfaced implants (N = 142, Straumann implants)<br />
in more than a 10-year period. They divided the<br />
patients in<strong>to</strong> 3 groups with respect <strong>to</strong> CIR: 0 <strong>to</strong> .99, 1 <strong>to</strong> 1.99,<br />
<strong>and</strong> ≥ 2. The mean clinical CIR was 1.77 <strong>and</strong> increased CIRs<br />
were not found <strong>to</strong> be associated with additional bone loss.The<br />
success rate with a CIR <strong>of</strong> >2 was 94.1% (48 <strong>of</strong> 51 implants).<br />
They concluded that implant res<strong>to</strong>rations with a CIR between<br />
2 <strong>and</strong> 3 could be successfully used in posterior regions <strong>of</strong> the<br />
dentition. However, it should be noted that the majority <strong>of</strong><br />
these implants were splinted (81.3%), which furnished an<br />
improved distribution <strong>of</strong> forces between implants.<br />
The impact <strong>of</strong> CIRs pertaining <strong>to</strong> bone loss around<br />
sintered porous surfaced implants (Endopore) was<br />
evaluated by Rokni, et al. 20 They moni<strong>to</strong>red (N = 198)<br />
implants for 4 years that were 5- <strong>to</strong> 7-mm long (short<br />
implants) <strong>and</strong> implants 9- <strong>to</strong> 12-mm long (long implants).<br />
Overall, implant res<strong>to</strong>rations had a 1.5 CIR <strong>and</strong><br />
demonstrated a 98.2% survival rate. The range <strong>of</strong> CIRs was<br />
0.81 <strong>to</strong> 3:1. The percentage <strong>of</strong> implants with a CIR between<br />
Figure 1. Single Tooth<br />
<strong>Implant</strong>: <strong>to</strong>oth position No.<br />
19. Radiograph <strong>of</strong> a<br />
res<strong>to</strong>red dental implant with<br />
a millimeter ruler<br />
superimposed on the film.<br />
It should be noted that <strong>to</strong><br />
compute the crown <strong>to</strong><br />
implant ratio (CIR) in this<br />
<strong>and</strong> the other figures, the<br />
following was recorded:<br />
clinical crown length was<br />
the res<strong>to</strong>red crown plus the<br />
abutment collar height plus<br />
the part <strong>of</strong> the implant body<br />
that was not encased in<br />
bone; implant length was<br />
the part <strong>of</strong> the implant<br />
encased in bone. In Figure<br />
1, the part <strong>of</strong> the implant<br />
encased in bone is 7 mm.<br />
The portion <strong>of</strong> the implant<br />
coronal <strong>to</strong> the bone plus<br />
the abutment <strong>and</strong> crown<br />
measure 12 mm. This<br />
results in a clinical CIR <strong>of</strong><br />
12/7 = 1.7.<br />
1.1 <strong>and</strong> 2 was 78.9%. <strong>Implant</strong>s with a CIR >2 (n = 20) were<br />
followed for approximately 3 years. Different sized implants<br />
had the following CIRs (indicated in brackets): 5 mm (2.6),<br />
7 mm (1.8), 9 mm (1.4) <strong>and</strong> 12 mm (1.0). There were no<br />
statistically significant relationships between CIRs <strong>and</strong><br />
bone loss. The data underscored that short implants with a<br />
sintered surface which manifested elevated CIRs did not<br />
result in their failure or bone loss.<br />
Nedir, et al 21 reported after a 7-year moni<strong>to</strong>ring period<br />
that the survival rate <strong>of</strong> short (< 10 mm) <strong>and</strong> longer implants<br />
(Straumann implants) (10 <strong>to</strong> 13 mm) (N = 276) used <strong>to</strong><br />
support single crowns or short prostheses were 100% <strong>and</strong><br />
99%, respectively. They provided the CIR for each length <strong>of</strong><br />
implant <strong>and</strong> the number <strong>of</strong> placed implants: 6-mm long,<br />
CIR-1.97, n = 6; 8-mm long, CIR-1.59, n = 97; 9-mm long,<br />
CIR-1.55, n = 8; 10-mm long, CIR-1.3, n = 194; 11-mm<br />
long, CIR-1.17, n = 71. In general, these data corroborated<br />
the predictable use <strong>of</strong> short implants <strong>to</strong> support prostheses.<br />
However, note that 6-mm implants were splinted <strong>to</strong> longer<br />
implants <strong>to</strong> support prostheses. In contrast, Rossi, et al 22<br />
moni<strong>to</strong>red for 2 years 35 patients who received a <strong>to</strong>tal <strong>of</strong> 40,<br />
6-mm long implants (Straumann) (19 with a 4.1-mm diameter;<br />
29 with a 4.8-mm diameter) that were not splinted<br />
<strong>to</strong>gether. Their mean implant CIR was 1.5 (range 0.8 <strong>to</strong> 2.3)<br />
<strong>and</strong> the implant survival rate was 95%. The mean bone loss<br />
3
Continuing Education<br />
<strong>Importance</strong> <strong>of</strong> <strong>Crown</strong> <strong>to</strong> <strong>Root</strong> <strong>and</strong> <strong>Crown</strong> <strong>to</strong> <strong>Implant</strong> Ratios<br />
Table 1. <strong>Crown</strong> <strong>to</strong> <strong>Implant</strong> Ratios (CIRs) <strong>of</strong> <strong>Implant</strong> Supported Prostheses<br />
(Single <strong>Crown</strong>s, Fixed Partial Denture [FPD], Cantilevered Bridges)<br />
CIRs <strong>of</strong> <strong>Implant</strong> Supported Single <strong>Crown</strong>s or FPD<br />
Study Number <strong>of</strong> <strong>Implant</strong>s CIR Percent Survivability<br />
Schulte, et al 17 889 1.3 mean 98.2%<br />
Tawil <strong>and</strong> Younan 18 262 a 99 %<br />
30 < 1 -<br />
70 1 <strong>to</strong> 1.2 -<br />
58 1.21 <strong>to</strong> 1.4 -<br />
29 1.41 <strong>to</strong> 1.6 -<br />
39 1.61 <strong>to</strong> 2 -<br />
8 > 2 -<br />
Blanes, et al 19 1.77 mean -<br />
8 0 <strong>to</strong> 0.99 -<br />
133 1 <strong>to</strong> 1.99 -<br />
51 > 2 b 91.4%<br />
Rokni, et al 20 1.5 mean 98.2%<br />
22 0.81 <strong>to</strong> 1 -<br />
156 1.1 <strong>to</strong> 2 -<br />
20 > 2 -<br />
Nedir, et al 21 111 1.55 <strong>to</strong> 1.97 c 100<br />
Rossi, et al 22 40 1.5 mean 95%<br />
range 0.8 <strong>to</strong> 2.3<br />
Urdaneta, et al 23 326 1.6 mean 98%<br />
40 ≥ 2 95%<br />
206 1.0 <strong>to</strong> 1.99 -<br />
11 < 1.0 -<br />
a mean CIR for all the implants was not provided, survival percentage is for all groups combined<br />
b survival rates only provided for CIRs ≥ 2.<br />
c CIR was computed related <strong>to</strong> specific implant lengths—6-mm long, CIR-1.97, n = 6; 8-mm long, CIR-1.59, n = 97; 9-mm long, CIR-1.55,<br />
n = 8, 10-mm long.<br />
CIRs <strong>of</strong> <strong>Implant</strong> Supported Cantilevered Prostheses<br />
Study Number <strong>of</strong> <strong>Implant</strong>s CIR Mean Length <strong>of</strong> <strong>Implant</strong>s or Percent<br />
Range <strong>of</strong> Sizes<br />
Survivability<br />
Wennstrom, et al 24 68 1.60 12.7 97%<br />
Brägger, et al 25 33 1.84 not recorded 98.4%<br />
Hälg, et al 26 46 1.65 6 <strong>to</strong> 12 mm 95.7%<br />
for implants that lost bone (29 <strong>of</strong> 38 implants) between<br />
loading <strong>and</strong> the 2-year followup was 0.43 mm. Two implants<br />
failed <strong>and</strong> were removed before res<strong>to</strong>rations were placed.<br />
Recently, Urdaneta, et al 23 assessed the effect <strong>of</strong><br />
increased CIR with respect <strong>to</strong> bone loss <strong>and</strong> other prosthetic<br />
complications. In more than a 70-month period, they<br />
4
moni<strong>to</strong>red 326 implants (Bicon)<br />
whose mean CIR was 1.6. Forty<br />
patients had a CIR > 2. They<br />
concluded that an increased CIR did<br />
not result in an increased amount <strong>of</strong><br />
bone loss, implant failure, or crown<br />
failures, but there was an increased<br />
amount <strong>of</strong> prosthetic problems<br />
associated with an increased CIR<br />
(eg, crown loosening [21/326] <strong>and</strong><br />
fracture <strong>of</strong> 2-mm wide posterior<br />
abutments [3/61]).<br />
Another study specifically evaluated<br />
bone loss related <strong>to</strong> CIRs (no<br />
survival data provided). Gomez-Polo,<br />
et al 27 assessed the correlation<br />
between crown-implant ratios <strong>and</strong><br />
bone resorption in 69 patients with 85<br />
implants. After 5.7 years, they reported that CIRs <strong>of</strong> 0.43 <strong>to</strong><br />
1.5 were not associated with peri-implant bone loss.<br />
A systematic review by Blanes 28 that addressed CIRs<br />
included only 2 <strong>of</strong> the above studies, 18,19 because<br />
investigations did not meet their inclusion criteria (eg,<br />
moni<strong>to</strong>ring for > 4 years). They concluded that CIRs do not<br />
affect peri-implant crestal bone loss. In addition, they<br />
reported that the survival rate <strong>of</strong> prostheses with a CIR <strong>of</strong><br />
more than 2 was 94.1%. Three other studies contained data<br />
with respect <strong>to</strong> CIRs when implants were used <strong>to</strong> support<br />
short span cantilevered bridges. 24-26 The reported CIRs, the<br />
percentages <strong>of</strong> implant survival after 5 years, the number <strong>of</strong><br />
assessed implants for each study, <strong>and</strong> the mean or range<br />
<strong>of</strong> implant sizes are listed in Table 1. Elevated CIRs on<br />
abutments for cantilevered bridges associated with<br />
successful prostheses further support the concept that<br />
implant res<strong>to</strong>rations can successfully <strong>to</strong>lerate CIR values<br />
that were considered risky ratios for teeth.<br />
From a different perspective, there are still unanswered<br />
questions. For instance, Blanes 28 questioned if the fulcrum<br />
point for prostheses with a large CIR is at the crown implant<br />
connection or at the most coronal bone-implant contact<br />
area. Most studies used the former for measurements, <strong>and</strong><br />
only his investigation 19 used the bone-implant contact area<br />
as the fulcrum point <strong>to</strong> calculate CIRs. Obviously, the latter<br />
a<br />
b<br />
Figures 2a <strong>and</strong> 2b. Radiographs <strong>of</strong> unilateral fixed implant prosthesis (straight line splint). The<br />
implant in the No. 21 position is 11.5-mm long <strong>and</strong> is encased in approximately 9.5 mm <strong>of</strong> bone. The<br />
clinical crown is 11-mm long plus an abutment which has a 2 mm collar height. This results in a CIR<br />
<strong>of</strong> 11 mm + 2 mm + 2 mm = 15 mm/9.5 mm = 1.57:1. The implant in the No. 19 position is 10-mm<br />
long <strong>and</strong> is encased in 8 mm <strong>of</strong> bone while supporting an abutment with a cuff height <strong>of</strong> 1 mm plus a<br />
clinical crown, which is 12-mm long. This results in a crown <strong>to</strong> implant ratio <strong>of</strong> 12 mm + 1 mm + 2 mm<br />
= 15 mm/8 mm = 1.87. The implant in the No. 18 position is 8-mm long <strong>and</strong> is encased in 6 mm <strong>of</strong><br />
bone while supporting an abutment with a 1-mm cuff height <strong>and</strong> a crown which is 12-mm long. This<br />
results in a CIR which is 12 mm + 1 mm + 2 mm = 15 mm/6 mm = 2.5. These implants benefit from<br />
the fact that the definitive PFM prosthesis is splinted—at least in a straight line fashion.<br />
results in larger CIRs (Figures 1, 2a<br />
<strong>to</strong> 2c, <strong>and</strong> 3a <strong>to</strong> 3g). The authors<br />
suggested that the bone-implant<br />
contact area was probably the<br />
Continuing Education<br />
<strong>Importance</strong> <strong>of</strong> <strong>Crown</strong> <strong>to</strong> <strong>Root</strong> <strong>and</strong> <strong>Crown</strong> <strong>to</strong> <strong>Implant</strong> Ratios<br />
c<br />
a<br />
b<br />
Figure 2c. Intraoral<br />
view <strong>of</strong> the completed<br />
cemented PFM splint.<br />
Figure 3a. Maxillary Arch<br />
Reconstruction. Intraoral<br />
view <strong>of</strong> long cus<strong>to</strong>m<br />
abutments attached <strong>to</strong><br />
short implants. The implant<br />
lengths are in brackets<br />
next <strong>to</strong> the corresponding<br />
<strong>to</strong>oth: No. 5 (8 mm), No. 6<br />
(10 mm), No. 7 (8 mm),<br />
No. 10 (8 mm), No. 11<br />
(10 mm), No. 12 (8 mm).<br />
Figure 3b. The res<strong>to</strong>red<br />
lateral incisor is 20-mm long<br />
<strong>and</strong> is supported by an<br />
implant which is 8 mm long<br />
(as part <strong>of</strong> a splinted<br />
prosthesis). The res<strong>to</strong>red<br />
length <strong>of</strong> the <strong>to</strong>oth is in<br />
excess <strong>of</strong> twice the length <strong>of</strong><br />
the corresponding implant<br />
(CIR is 2.5). In actuality, the<br />
abutment adds 2 additional<br />
milli-meters <strong>to</strong> the “crown”<br />
portion <strong>of</strong> the equation,<br />
rendering the crown <strong>to</strong> root<br />
ratio 22/8 = 2.75:1. Since<br />
this 8 mm implant is approximately<br />
7 mm in bone on<br />
the radiograph, the ultimate<br />
CIR is about 2.87:1.<br />
5
Continuing Education<br />
<strong>Importance</strong> <strong>of</strong> <strong>Crown</strong> <strong>to</strong> <strong>Root</strong> <strong>and</strong> <strong>Crown</strong> <strong>to</strong> <strong>Implant</strong> Ratios<br />
fulcrum, because components connected <strong>to</strong> the implant<br />
were stronger than the cortical bone. Another issue not<br />
resolved relates <strong>to</strong> how different prosthetic designs (eg,<br />
single crowns (Figure 1), fixed partial dentures, straight-line<br />
splinting (Figures 2a <strong>to</strong> 2c), splinting around a curve <strong>of</strong> an<br />
arch (Figures 3a <strong>to</strong> 3g) impact on the relationship between<br />
CIRs <strong>and</strong> peri-implant bone loss, technical problems <strong>and</strong><br />
survival <strong>of</strong> prostheses.<br />
The authors <strong>of</strong> this review paper agree with Blanes 28<br />
with respect <strong>to</strong> defining the clinical crown portion as the<br />
res<strong>to</strong>red crown plus the abutment collar plus the part <strong>of</strong> the<br />
implant not encased in bone (Figures 1 <strong>to</strong> 3g). In other<br />
words, the level <strong>of</strong> the bone is considered the fulcrum for<br />
computing CIRs. This does not preclude that a potential<br />
weak point <strong>of</strong> prosthetic failure may occur at the abutmentimplant<br />
interface. However, the most important fulcrum<br />
point exists at the level <strong>of</strong> the most coronal bone <strong>to</strong> implant<br />
contact. This is the location where the applied forces <strong>and</strong><br />
strains they create are resisted by the bone.<br />
SHORT VERSUS LONG DENTAL IMPLANTS<br />
In general, finite elemental analysis studies indicated that<br />
forces on dental implants are transferred <strong>to</strong> the bone crest<br />
adjacent <strong>to</strong> implants 29,30 <strong>and</strong> a small amount <strong>of</strong> stress is<br />
conveyed <strong>to</strong> the apical region. 30 These data provide an<br />
important premise supporting the use <strong>of</strong> short implants.<br />
Namely, if stresses are placed at the crest after<br />
osseointegration occurred, then the length <strong>of</strong> the implant<br />
might not be the crucial fac<strong>to</strong>r with regard <strong>to</strong> distributing<br />
c<br />
d<br />
Figure 3c. Intraoral<br />
retracted view <strong>of</strong> the<br />
cemented PFM<br />
prosthesis described in<br />
Figure 3b.<br />
Figure 3d. Smile-line <strong>of</strong><br />
the definitive prosthesis<br />
in place.<br />
prosthetic loads <strong>to</strong> the interface between bone <strong>and</strong> the<br />
implant. Accordingly, it is important <strong>to</strong> assess the survival <strong>of</strong><br />
short implants, which usually have increased CIRs when<br />
res<strong>to</strong>red. However, there are many variables (Table 2) 31 that<br />
make it difficult <strong>to</strong> compare success rates in different studies.<br />
Nevertheless, the preponderance <strong>of</strong> data indicate that short<br />
implants are very successful <strong>and</strong> that survival rates for short<br />
textured implants are comparable <strong>to</strong> longer implants. 31-34<br />
In this regard, 4 review papers evaluated survivability <strong>of</strong><br />
short dental implants <strong>and</strong> concluded that they could<br />
predictably be employed <strong>to</strong> support prostheses. 31-34 Recently,<br />
a systematic review concluded that there was no statistically<br />
significant difference in survival rates between short (≤ 8 or ≤<br />
10 mm) <strong>and</strong> conventional (> 10 mm) rough surfaced implants<br />
placed in <strong>to</strong>tally or partially edentulous patients. 35<br />
Table 2. Variables <strong>and</strong> Confounding Fac<strong>to</strong>rs When Comparing Studies With Respect <strong>to</strong> Survivability<br />
<strong>of</strong> Short <strong>Implant</strong>s 31<br />
PATIENT: Systemic health, smoking status, periodontal status, parafunction, personal hygiene, pr<strong>of</strong>essional<br />
maintenance<br />
IMPLANTS: Type, length, width, surface characteristics, shape, internal connection, external connection<br />
BONE TYPE: I, II, II, IV<br />
SURGERY: Skill <strong>of</strong> surgeon, bone grafting or not<br />
PROSTHESIS: Splinted or not, crown <strong>to</strong> implant ratio, fixed partial denture, cantilever<br />
SURVIVAL RATE: Size <strong>of</strong> the study, duration <strong>of</strong> moni<strong>to</strong>ring period<br />
Modified from Mor<strong>and</strong> <strong>and</strong> Irinakis 31<br />
6
Continuing Education<br />
<strong>Importance</strong> <strong>of</strong> <strong>Crown</strong> <strong>to</strong> <strong>Root</strong> <strong>and</strong> <strong>Crown</strong> <strong>to</strong> <strong>Implant</strong> Ratios<br />
His<strong>to</strong>rically, studies indicated longer implants had a<br />
greater survival rate than shorter implants when a 10-mm<br />
length was used as the cut point. 36 Renouard <strong>and</strong> Nis<strong>and</strong> 32<br />
documented that 11 <strong>of</strong> 12 investigations reported a higher<br />
failure rate with short implants than longer implants when<br />
machine surface implants were used. 37-47 The 12th study<br />
employed machined <strong>and</strong> hydroxyapatite-coated implants. 48<br />
In contrast, Renouard <strong>and</strong> Nis<strong>and</strong> 32 reported that 9 studies<br />
indicated that implant length did not affect the survival rate<br />
<strong>and</strong> 6 <strong>of</strong> the 9 investigations included in their assessment<br />
used textured surface implants. 49-54<br />
Many older studies <strong>and</strong> 7 recent investigations published<br />
between 2006 <strong>and</strong> 2010 33,55-60 all indicated that short implants<br />
had a high survival rate <strong>and</strong> could predictably be used <strong>to</strong><br />
support crowns <strong>and</strong> prostheses (Table 3). 18,21,33,52,55-63<br />
Currently, textured surface implants are usually employed. 33<br />
VERTICAL CANTILEVER FORCES<br />
With regards <strong>to</strong> the biomechanics <strong>of</strong> increasing the crown <strong>to</strong><br />
root or implant ratio, as a crown becomes larger, bending<br />
moments can detrimentally affect a prosthesis.To compute the<br />
magnitude <strong>of</strong> a force moment, it is necessary <strong>to</strong> multiply the<br />
force by the perpendicular distance (moment arm) from the<br />
fulcrum <strong>to</strong> the endpoint <strong>of</strong> the lever arm. 64 Conceptually, the<br />
occlusal height <strong>of</strong> a crown should not affect the force moment<br />
along the vertical axis, because if it is centered, its effective<br />
moment arm is nonexistent. 64 However, noncentered occlusal<br />
contacts or lateral loads are prevalent <strong>and</strong> can induce<br />
considerable moment arms, thereby <strong>to</strong>rquing the prosthesis.<br />
Therefore, as the clinical crown <strong>to</strong> implant length increases,<br />
there is a greater lever arm that potentially can amplify stress<br />
on the res<strong>to</strong>ration. It is evident that with a larger clinical crown<br />
<strong>and</strong> smaller implant there potentially will be a bigger lever arm.<br />
Bidez <strong>and</strong> Misch 65 indicated that when a crown height is<br />
increased from 10 <strong>to</strong> 20 mm there is a 100% increase <strong>of</strong> force<br />
on the implant. In addition, angulation is a force magnifier <strong>and</strong><br />
Misch <strong>and</strong> Bidez 66 noted that a 12° angle increased the force<br />
on an implant by 20%.<br />
Increased stress has the potential <strong>to</strong> decrease<br />
survivability <strong>of</strong> prostheses or create biological <strong>and</strong> technical<br />
problems. Fortunately, prostheses with increased CIRs<br />
from one <strong>to</strong> 2 have demonstrated a high survivability rate<br />
(Table 1). Similarly, short implants that support prostheses<br />
e<br />
f<br />
g<br />
Figures 3e, 3f, <strong>and</strong> 3g.<br />
Maxillary right, anterior,<br />
<strong>and</strong> left side radiographs<br />
<strong>of</strong> the patient depicting<br />
the CIRs. These implants<br />
benefit from the crossarch<br />
splinting <strong>of</strong> the<br />
definitive prosthesis.<br />
that usually manifest an increased CIR have demonstrated<br />
high survival rates (Table 3). The precise height that cannot<br />
be exceeded <strong>to</strong> avoid de-osseointegration or fracture <strong>of</strong> an<br />
implant is unknown <strong>and</strong> will be affected by fac<strong>to</strong>rs such as<br />
7
Continuing Education<br />
<strong>Importance</strong> <strong>of</strong> <strong>Crown</strong> <strong>to</strong> <strong>Root</strong> <strong>and</strong> <strong>Crown</strong> <strong>to</strong> <strong>Implant</strong> Ratios<br />
Table 3. Studies Dedicated <strong>to</strong> Assessing Survival Rates <strong>of</strong> Short Dental <strong>Implant</strong>s a<br />
Study n No. <strong>of</strong> implants Length Type Surface Survival Rate Time<br />
Anitua, et al 56 293 532 7 <strong>to</strong> 8.5 mm BTI rough 99.2% 31 months<br />
Arlin, et al 55 not reported 35 6 mm ITI rough 94.3% 2 years<br />
not reported 141 8 mm 99.3%<br />
Fugazzot<strong>to</strong> 33 1,774 2,073 6 <strong>to</strong> 9 mm ITI rough 98.4% 36.2 months<br />
Goene, et al 61 188 311 7 <strong>to</strong> 8.5 Osteotite acid etched 95.8% 3 years<br />
Grant, et al 57 124 355 8 mm Nobel not reported 99% < 1 <strong>to</strong> ≥2 years<br />
Griffin, et al 58 167 168 8 mm SO, Nobel HA coated 100% 34.9 months<br />
Malo, et al 59 237 408 7 <strong>and</strong> 8.5 mm Nobel machined/TiUnite 96 <strong>to</strong> 97% 5 years<br />
Misch, et al 60 273 715 9 mm BTI rough 99.2% 12 <strong>to</strong> 60 months<br />
30 7 mm<br />
Nedir, et al 21 236 264 6 <strong>to</strong> 9 mm ITI TPS 100% 7 years<br />
264 SLA<br />
Tawil, Younan 18 111 269 7 <strong>to</strong> < 10 mm Nobel machined 95.5% 12 <strong>to</strong> 92 months<br />
Tes<strong>to</strong>ri et al 52 not reported 31 7 <strong>to</strong> 8.5 mm Osteotite acid-etched 96.7% 4 years<br />
van Steenberghe, et al 62 - 10 8 mm Astra rough 100% 2 years<br />
- 6 9 mm<br />
ten Bruggenkate, et al 63 126 253 6 mm ITI TPS 97% 1 <strong>to</strong> 7 years<br />
a Studies listed alphabetically.<br />
implant diameter, splinting <strong>of</strong> implants, <strong>and</strong> magnitude,<br />
duration, frequency, <strong>and</strong> direction <strong>of</strong> occlusal forces.<br />
Studies have indicated that with increased CIRs there<br />
was no additional bone loss compared <strong>to</strong> locations that did<br />
not have increased CIRs. 17-20,24,26 In general, there is a<br />
dearth <strong>of</strong> information that addresses how <strong>of</strong>ten technical<br />
complications occur around res<strong>to</strong>rations with increased CIRs<br />
pertaining <strong>to</strong> various prosthetic designs: single <strong>to</strong>oth, straightline<br />
splint, or fixed res<strong>to</strong>rations that have cross arch<br />
stabilization. Of the 7 studies listed in Table 1 that discussed<br />
CIRs, only 2 reported the occurrence <strong>of</strong> technical<br />
problems. 18,23 Tawil <strong>and</strong> Younan 18 noted the incidence <strong>of</strong><br />
screw loosening (7.8%) <strong>and</strong> porcelain fractures (5.2%)<br />
among teeth with increased CIRs. These data are within the<br />
23% technical complication rate for implant supported FDPs<br />
noted in the systematic review by Berglundh, et al. 67<br />
Urdaneta, et al 23 reported 3 fractures (3/61) <strong>of</strong> the 2-mm wide<br />
abutments used in the posterior areas when the CIR was 1.47<br />
<strong>and</strong> no fractures among 3-mm wide abutments (184/184)<br />
when there was an increased CIR. They also noted that 21 <strong>of</strong><br />
326 crowns loosened during the observation period <strong>and</strong> 90%<br />
<strong>of</strong> the time this occurred in the maxillary anterior region. It was<br />
suggested that splinting <strong>of</strong> multiple adjacent implants might<br />
have avoided these undesirable sequelae.<br />
Several studies that assessed the utility <strong>of</strong> horizontal<br />
cantilevers also recorded increased CIRs (Table 1). 24-26<br />
These investigations usually reported minor technical<br />
problems associated with short span cantilevered bridges<br />
that had increased CIRs (see Aglietta, et al 68 for review).<br />
While both vertical <strong>and</strong> horizontal cantilevers may increase<br />
stress on implants <strong>and</strong> the prosthesis that they<br />
support, the resultant problems may not be exactly similar.<br />
For instance, a prosthesis with an increased CIR due <strong>to</strong> a<br />
vertical cantilever may be supported on both ends with a<br />
terminal abutment <strong>and</strong> this may alter the types <strong>of</strong> technical<br />
problems that may occur.<br />
Other investigations that assessed the survival <strong>of</strong><br />
short implants did not address technical problems that<br />
may occur if an increased CIR was created upon<br />
prosthesis fabrication. 32-35 At present, no definitive<br />
8
Continuing Education<br />
<strong>Importance</strong> <strong>of</strong> <strong>Crown</strong> <strong>to</strong> <strong>Root</strong> <strong>and</strong> <strong>Crown</strong> <strong>to</strong> <strong>Implant</strong> Ratios<br />
Table 4. Clinical Suggestions for Res<strong>to</strong>ring Teeth With Increased<br />
<strong>Crown</strong> <strong>to</strong> <strong>Implant</strong> Ratios<br />
1. In posterior areas, res<strong>to</strong>re the occlusal surfaces <strong>of</strong> teeth in such a<br />
manner that the patient’s incisal or canine guidance discludes the<br />
posterior teeth <strong>and</strong> minimizes lateral contact in m<strong>and</strong>ibular<br />
excursions. 60<br />
2. Increase the number <strong>of</strong> implants supporting the prosthesis. This adds<br />
<strong>to</strong> the surface area where occlusal forces are transmitted.<br />
3. Increase the bone implant contact area with wider implants.<br />
4. Reduce the occlusal width <strong>of</strong> posterior teeth <strong>and</strong> have centric contacts<br />
centered over the implants. 31<br />
5. Avoid elevated CIR in bruxers or over engineer the case with<br />
additional implants <strong>and</strong> splint around the turn <strong>of</strong> the arch with the<br />
res<strong>to</strong>ration when possible.<br />
6. Patients can wear a night guard <strong>to</strong> reduce nocturnal stresses on the<br />
prosthesis.<br />
7. Short implants should be splinted <strong>to</strong>gether <strong>to</strong> maximize their support<br />
<strong>of</strong> the prosthesis <strong>and</strong> provide cross arch stabilization when<br />
possible. 12,65<br />
8. Use textured-surfaced implants that have a higher percentage <strong>of</strong> bone<br />
implant contact.<br />
9. Flatten cuspal inclines. 31<br />
10. Employ implants with decreased thread pitch (distance between the<br />
threads), thereby resulting in an increased number <strong>of</strong> threads per<br />
unit length <strong>and</strong> an increased surface area. 60 However, there are no<br />
data that the thread pitch altered the survival rate <strong>of</strong> prostheses with<br />
increased CIRs.<br />
short implants <strong>of</strong>ten results in increased CIRs,<br />
the clinical implication is that short implants (<<br />
10 mm) can be used <strong>to</strong> support a prosthesis<br />
<strong>and</strong> do not result in early demise <strong>of</strong> a<br />
res<strong>to</strong>ration. Ultimately, when necessary,<br />
utilization <strong>of</strong> short implants <strong>and</strong> prostheses<br />
with increased CIRs provide greater flexibility<br />
when treatment planning patients.<br />
These conclusions are in agreement with<br />
recent statements by the European Association for<br />
Osseointegration, 69 which indicated the following:<br />
● Consensus statement: “Res<strong>to</strong>rations with<br />
a CIR up <strong>to</strong> 2 do not induce peri-implant<br />
bone loss.”<br />
● Clinical implications: “A FDP or single-<strong>to</strong>oth<br />
res<strong>to</strong>ration with a CIR up <strong>to</strong> 2 is an acceptable<br />
prosthetic option.”<br />
Nevertheless, it is recognized that a<br />
prosthesis with an increased CIR is subject <strong>to</strong><br />
increased occlusal forces. This can result in<br />
amplified stress on the prosthesis <strong>and</strong> the<br />
surrounding bone. 70,71 Accordingly, it is<br />
advantageous <strong>to</strong> reduce forces on res<strong>to</strong>rations<br />
with an increased CIR. Ten suggestions are<br />
listed in Table 4 for how <strong>to</strong> diminish stresses on<br />
prostheses with an increased CIR, thereby<br />
possibly reducing biological <strong>and</strong> technical<br />
complications <strong>and</strong> increasing the survivability<br />
<strong>of</strong> these constructs.<br />
statements can be made about an increased rate <strong>of</strong><br />
technical problems associated with increased CIRs, since<br />
this issue has not been highly documented in studies.<br />
CONCLUSIONS<br />
The available data (Table 1) demonstrate that prostheses<br />
with increased CIRs up <strong>to</strong> 2 have a high survival rate.<br />
Furthermore, increased CIRs did not result in additional<br />
peri-implant bone loss. 17,19,20,23-26 Therefore, when there is<br />
a dearth <strong>of</strong> bone or ana<strong>to</strong>mic structures that preclude<br />
placement <strong>of</strong> longer implants, treatment planning a<br />
prosthesis that results in an increased CIR is a reasonable,<br />
predictable procedure. Furthermore, since placement <strong>of</strong><br />
REFERENCES<br />
1. Ante IH. The fundamental principles <strong>of</strong> abutments.<br />
Mich State Dent Soc Bull. 1926;8:232-257.<br />
2. Greenstein G, Greenstein B, Cavallaro J. Prerequisite for<br />
treatment planning implant dentistry: periodontal prognostication<br />
<strong>of</strong> compromised teeth. Compend Contin Educ Dent.<br />
2007;28:436-447.<br />
3. Lulic M, Brägger U, Lang NP, et al. Ante’s (1926) law revisited:<br />
a systematic review on survival rates <strong>and</strong> complications <strong>of</strong><br />
fixed dental prostheses (FDPs) on severely reduced<br />
periodontal tissue support. Clin Oral <strong>Implant</strong>s Res.<br />
2007;18(suppl 3):63-72.<br />
4. Pjetursson BE, Tan K, Lang NP, et al. A systematic review <strong>of</strong><br />
the survival <strong>and</strong> complication rates <strong>of</strong> fixed partial dentures<br />
(FPDs) after an observation period <strong>of</strong> at least 5 years: IV.<br />
Cantilever or extension FPDs. Clin Oral <strong>Implant</strong>s Res.<br />
2004;15:667-676.<br />
9
Continuing Education<br />
<strong>Importance</strong> <strong>of</strong> <strong>Crown</strong> <strong>to</strong> <strong>Root</strong> <strong>and</strong> <strong>Crown</strong> <strong>to</strong> <strong>Implant</strong> Ratios<br />
5. Tan K, Pjetursson BE, Lang NP, et al. A systematic review <strong>of</strong><br />
the survival <strong>and</strong> complication rates <strong>of</strong> fixed partial dentures<br />
(FPDs) after an observation period <strong>of</strong> at least 5 years: III.<br />
Conventional FPDs. Clin Oral <strong>Implant</strong>s Res. 2004;15:654-666.<br />
6. Grossmann Y, Sadan A. The prosthodontic concept <strong>of</strong><br />
crown-<strong>to</strong>-root ratio: a review <strong>of</strong> the literature. J Prosthet<br />
Dent. 2005;93:559-562.<br />
7. Dykema RW, Goodacre CJ, Phillips RW. Johns<strong>to</strong>n’s Modern<br />
Practice in Fixed Prosthodontics. 4th ed. Philadelphia, PA:<br />
WB Saunders; 1986:8-21.<br />
8. Shillingburg HT Jr, Hobo S, Whitsett LD, et al. Fundamentals<br />
<strong>of</strong> Fixed Prosthodontics. 3rd ed. Chicago, IL: Quintessence<br />
Publishing; 1997:89-90.<br />
9. Langer Y, Langer A. <strong>Root</strong>-retained overdentures: Part I—<br />
Biomechanical <strong>and</strong> clinical aspects. J Prosthet Dent.<br />
1991;66:784-789.<br />
10. Schluger S, Yuodelis RA, Page RC, et al. Periodontal<br />
Diseases: Basic Phenomena, Clinical Management, <strong>and</strong><br />
Occlusal <strong>and</strong> Res<strong>to</strong>rative Interrelationships. 2nd ed.<br />
Philadelphia, PA: Lea & Febiger; 1990:405-412.<br />
11. Faucher RR, Bryant RA. Bilateral fixed splints. Int J<br />
Periodontics Res<strong>to</strong>rative Dent. 1983;3:8-37.<br />
12. Guichet DL, Yoshinobu D, Capu<strong>to</strong> AA. Effect <strong>of</strong> splinting <strong>and</strong><br />
interproximal contact tightness on load transfer by implant<br />
res<strong>to</strong>rations. J Prosthet Dent. 2002;87:528-535.<br />
13. Grossmann Y, Finger IM, Block MS. Indications for splinting<br />
implant res<strong>to</strong>rations. J Oral Maxill<strong>of</strong>ac Surg. 2005;63:1642-1652.<br />
14. Misch CE, Goodacre CJ, Finley JM, et al. Consensus<br />
conference panel report: crown-height space guidelines for<br />
implant dentistry—part 2. <strong>Implant</strong> Dent. 2006;15:113-121.<br />
15. Rangert BR, Sullivan RM, Jemt TM. Load fac<strong>to</strong>r control for<br />
implants in the posterior partially edentulous segment. Int J<br />
Oral Maxill<strong>of</strong>ac <strong>Implant</strong>s. 1997;12:360-370.<br />
16. Glantz PO, Nilner K. Biomechanical aspects <strong>of</strong> prosthetic<br />
implant-borne reconstructions. Periodon<strong>to</strong>l 2000.<br />
1998;17:119-124.<br />
17. Schulte J, Flores AM, Weed M. <strong>Crown</strong>-<strong>to</strong>-implant ratios <strong>of</strong> single<br />
<strong>to</strong>oth implant-supported res<strong>to</strong>rations. J Prosthet Dent. 2007;98:1-5.<br />
18. Tawil G, Younan R. Clinical evaluation <strong>of</strong> short, machinedsurface<br />
implants followed for 12 <strong>to</strong> 92 months. Int J Oral<br />
Maxill<strong>of</strong>ac <strong>Implant</strong>s. 2003;18:894-901.<br />
19. Blanes RJ, Bernard JP, Blanes ZM, et al. A 10-year<br />
prospective study <strong>of</strong> ITI dental implants placed in the<br />
posterior region. II: Influence <strong>of</strong> the crown-<strong>to</strong>-implant ratio<br />
<strong>and</strong> different prosthetic treatment modalities on crestal bone<br />
loss. Clin Oral <strong>Implant</strong>s Res. 2007;18:707-714.<br />
20. Rokni S, Todescan R, Watson P, et al. An assessment <strong>of</strong><br />
crown-<strong>to</strong>-root ratios with short sintered porous-surfaced<br />
implants supporting prostheses in partially edentulous<br />
patients. Int J Oral Maxill<strong>of</strong>ac <strong>Implant</strong>s. 2005;20:69-76.<br />
21. Nedir R, Bisch<strong>of</strong> M, Briaux JM, et al. A 7-year life table<br />
analysis from a prospective study on ITI implants with<br />
special emphasis on the use <strong>of</strong> short implants. Results from<br />
a private practice. Clin Oral <strong>Implant</strong>s Res. 2004;15:150-157.<br />
22. Rossi F, Ricci E, Marchetti C, et al. Early loading <strong>of</strong> single<br />
crowns supported by 6-mm-long implants with a moderately<br />
rough surface: a prospective 2-year follow-up cohort study.<br />
Clin Oral <strong>Implant</strong>s Res. 2010;21:937-943.<br />
23. Urdaneta RA, Rodriguez S, McNeil DC, et al. The effect <strong>of</strong><br />
increased crown-<strong>to</strong>-implant ratio on single-<strong>to</strong>oth locking-taper<br />
implants. Int J Oral Maxill<strong>of</strong>ac <strong>Implant</strong>s. 2010;25:729-743.<br />
24. Wennström J, Zurdo J, Karlsson S, et al. Bone level change at<br />
implant-supported fixed partial dentures with <strong>and</strong> without<br />
cantilever extension after 5 years in function. J Clin Periodon<strong>to</strong>l.<br />
2004;31:1077-1083.<br />
25. Brägger U, Karoussis I, Persson R, et al. Technical <strong>and</strong><br />
biological complications/failures with single crowns <strong>and</strong> fixed<br />
partial dentures on implants: a 10-year prospective cohort<br />
study. Clin Oral <strong>Implant</strong>s Res. 2005;16:326-334.<br />
26. Hälg GA, Schmid J, Hämmerle CH. Bone level changes at<br />
implants supporting crowns or fixed partial dentures with or<br />
without cantilevers. Clin Oral <strong>Implant</strong>s Res. 2008;19:983-990.<br />
27. Gomez-Polo M, Bartens F, Sala L, et al. The correlation<br />
between crown-implant ratios <strong>and</strong> marginal bone resorption: a<br />
preliminary clinical study. Int J Prosthodont. 2010;23:33-37.<br />
28. Blanes RJ. To what extent does the crown-implant ratio<br />
affect the survival <strong>and</strong> complications <strong>of</strong> implant-supported<br />
reconstructions A systematic review. Clin Oral <strong>Implant</strong>s<br />
Res. 2009;20(suppl 4):67-72.<br />
29. Lum LB. A biomechanical rationale for the use <strong>of</strong> short implants.<br />
J Oral Implan<strong>to</strong>l. 1991;17:126-131.<br />
30. Rieger MR, Mayberry M, Brose MO. Finite element analysis <strong>of</strong><br />
six endosseous implants. J Prosthet Dent. 1990;63:671-676.<br />
31. Mor<strong>and</strong> M, Irinakis T. The challenge <strong>of</strong> implant therapy in the<br />
posterior maxilla: providing a rationale for the use <strong>of</strong> short<br />
implants. J Oral Implan<strong>to</strong>l. 2007;33:257-266.<br />
32. Renouard F, Nis<strong>and</strong> D. Impact <strong>of</strong> implant length <strong>and</strong><br />
diameter on survival rates. Clin Oral <strong>Implant</strong>s Res.<br />
2006;17(suppl 2):35-51.<br />
33. Fugazzot<strong>to</strong> PA. Shorter implants in clinical practice: rationale<br />
<strong>and</strong> treatment results. Int J Oral Maxill<strong>of</strong>ac <strong>Implant</strong>s.<br />
2008;23:487-496.<br />
34. Misch CE. Short dental implants: a literature review <strong>and</strong><br />
rationale for use. Dent Today. 2005;24:64-68.<br />
35. Kotsovilis S, Fourmousis I, Karoussis IK, et al. A systematic<br />
review <strong>and</strong> meta-analysis on the effect <strong>of</strong> implant length on the<br />
survival <strong>of</strong> rough-surface dental implants. J Periodon<strong>to</strong>l.<br />
2009;80:1700-1718.<br />
36. Goodacre CJ, Campagni WV, Aquilino SA. Tooth preparations<br />
for complete crowns: an art form based on scientific principles.<br />
J Prosthet Dent. 2001;85:363-376.<br />
37. van Steenberghe D, Lekholm U, Bolender C, et al. Applicability<br />
<strong>of</strong> osseointegrated oral implants in the rehabilitation <strong>of</strong> partial<br />
edentulism: a prospective multicenter study on 558 fixtures. Int J<br />
Oral Maxill<strong>of</strong>ac <strong>Implant</strong>s. 1990;5:272-281.<br />
38. Friberg B, Jemt T, Lekholm U. Early failures in 4,641<br />
consecutively placed Brånemark dental implants: a study from<br />
stage 1 surgery <strong>to</strong> the connection <strong>of</strong> completed prostheses. Int<br />
J Oral Maxill<strong>of</strong>ac <strong>Implant</strong>s. 1991;6:142-146.<br />
39. Jemt T. Failures <strong>and</strong> complications in 391 consecutively<br />
10
Continuing Education<br />
<strong>Importance</strong> <strong>of</strong> <strong>Crown</strong> <strong>to</strong> <strong>Root</strong> <strong>and</strong> <strong>Crown</strong> <strong>to</strong> <strong>Implant</strong> Ratios<br />
inserted fixed prostheses supported by Brånemark implants in<br />
edentulous jaws: a study <strong>of</strong> treatment from the time <strong>of</strong><br />
prosthesis placement <strong>to</strong> the first annual checkup. Int J Oral<br />
Maxill<strong>of</strong>ac <strong>Implant</strong>s. 1991;6:270-276.<br />
40. Bahat O. Treatment planning <strong>and</strong> placement <strong>of</strong> implants in the<br />
posterior maxillae: report <strong>of</strong> 732 consecutive Nobelpharma<br />
implants. Int J Oral Maxill<strong>of</strong>ac <strong>Implant</strong>s. 1993;8:151-161.<br />
41. Jemt T, Lekholm U. <strong>Implant</strong> treatment in edentulous<br />
maxillae: a 5-year follow-up report on patients with different<br />
degrees <strong>of</strong> jaw resorption. Int J Oral Maxill<strong>of</strong>ac <strong>Implant</strong>s.<br />
1995;10:303-311.<br />
42. Wyatt CC, Zarb GA. Treatment outcomes <strong>of</strong> patients with<br />
implant-supported fixed partial prostheses. Int J Oral<br />
Maxill<strong>of</strong>ac <strong>Implant</strong>s. 1998;13:204-211.<br />
43. Lekholm U, Gunne J, Henry P, et al. Survival <strong>of</strong> the<br />
Brånemark implant in partially edentulous jaws: a 10-year<br />
prospective multicenter study. Int J Oral Maxill<strong>of</strong>ac <strong>Implant</strong>s.<br />
1999;14:639-645.<br />
44. Bahat O. Brånemark system implants in the posterior<br />
maxilla: clinical study <strong>of</strong> 660 implants followed for 5 <strong>to</strong> 12<br />
years. Int J Oral Maxill<strong>of</strong>ac <strong>Implant</strong>s. 2000;15:646-653.<br />
45. Naert I, Koutsikakis G, Duyck J, et al. Biologic outcome <strong>of</strong><br />
implant-supported res<strong>to</strong>rations in the treatment <strong>of</strong> partial<br />
edentulism. Part I: a longitudinal clinical evaluation. Clin<br />
Oral <strong>Implant</strong>s Res. 2002;13:381-389.<br />
46. Weng D, Jacobson Z, Tarnow D, et al. A prospective<br />
multicenter clinical trial <strong>of</strong> 3i machined-surface implants:<br />
results after 6 years <strong>of</strong> follow-up. Int J Oral Maxill<strong>of</strong>ac <strong>Implant</strong>s.<br />
2003;18:417-423.<br />
47. Herrmann I, Lekholm U, Holm S, et al. Evaluation <strong>of</strong> patient<br />
<strong>and</strong> implant characteristics as potential prognostic fac<strong>to</strong>rs for<br />
oral implant failures. Int J Oral Maxill<strong>of</strong>ac <strong>Implant</strong>s.<br />
2005;20:220-230.<br />
48. Winkler S, Morris HF, Ochi S. <strong>Implant</strong> survival <strong>to</strong> 36 months as<br />
related <strong>to</strong> length <strong>and</strong> diameter. Ann Periodon<strong>to</strong>l. 2000;5:22-31.<br />
49. Buser D, Mericske-Stern R, Bernard JP, et al. Long-term<br />
evaluation <strong>of</strong> non-submerged ITI implants. Part 1: 8-year life<br />
table analysis <strong>of</strong> a prospective multicenter study with 2359<br />
implants. Clin Oral <strong>Implant</strong>s Res. 1997;8:161-172.<br />
50. Ellegaard B, Baelum V, Karring T. <strong>Implant</strong> therapy in<br />
periodontally compromised patients. Clin Oral <strong>Implant</strong>s Res.<br />
1997;8:180-188.<br />
51. Brocard D, Barthet P, Baysse E, et al. A multicenter report on<br />
1,022 consecutively placed ITI implants: a 7-year<br />
longitudinal study. Int J Oral Maxill<strong>of</strong>ac <strong>Implant</strong>s.<br />
2000;15:691-700.<br />
52. Tes<strong>to</strong>ri T, Wiseman L, Woolfe S, et al. A prospective multicenter<br />
clinical study <strong>of</strong> the Osseotite implant: four-year interim report.<br />
Int J Oral Maxill<strong>of</strong>ac <strong>Implant</strong>s. 2001;16:193-200.<br />
53. Feldman S, Boitel N, Weng D, et al. Five-year survival<br />
distributions <strong>of</strong> short-length (10 mm or less) machinedsurfaced<br />
<strong>and</strong> Osseotite implants. Clin <strong>Implant</strong> Dent Relat<br />
Res. 2004;6:16-23.<br />
54. Romeo E, Lops D, Margutti E, et al. Long-term survival <strong>and</strong><br />
success <strong>of</strong> oral implants in the treatment <strong>of</strong> full <strong>and</strong> partial<br />
arches: a 7-year prospective study with the ITI dental implant<br />
system. Int J Oral Maxill<strong>of</strong>ac <strong>Implant</strong>s. 2004;19:247-259.<br />
55. Arlin ML. Short dental implants as a treatment option: results<br />
from an observational study in a single private practice. Int J<br />
Oral Maxill<strong>of</strong>ac <strong>Implant</strong>s. 2006;21:769-776.<br />
56. Anitua E, Orive G, Aguirre JJ, et al. Five-year clinical<br />
evaluation <strong>of</strong> short dental implants placed in posterior areas: a<br />
retrospective study. J Periodon<strong>to</strong>l. 2008;79:42-48.<br />
57. Grant BT, Pancko FX, Kraut RA. Outcomes <strong>of</strong> placing short<br />
dental implants in the posterior m<strong>and</strong>ible: a retrospective study<br />
<strong>of</strong> 124 cases. J Oral Maxill<strong>of</strong>ac Surg. 2009;67:713-717.<br />
58. Griffin TJ, Cheung WS. The use <strong>of</strong> short, wide implants in<br />
posterior areas with reduced bone height: a retrospective<br />
investigation. J Prosthet Dent. 2004;92:139-144.<br />
59. Maló P, de Araújo Nobre M, Rangert B. Short implants<br />
placed one-stage in maxillae <strong>and</strong> m<strong>and</strong>ibles: a retrospective<br />
clinical study with 1 <strong>to</strong> 9 years <strong>of</strong> follow-up. Clin <strong>Implant</strong><br />
Dent Relat Res. 2007;9:15-21.<br />
60. Misch CE, Steignga J, Barboza E, et al. Short dental implants<br />
in posterior partial edentulism: a multicenter retrospective 6-<br />
year case series study. J Periodon<strong>to</strong>l. 2006;77:1340-1347.<br />
61. Goené R, Bianchesi C, Hüerzeler M, et al. Performance <strong>of</strong><br />
short implants in partial res<strong>to</strong>rations: 3-year follow-up <strong>of</strong><br />
Osseotite implants. <strong>Implant</strong> Dent. 2005;14:274-280.<br />
62. van Steenberghe D, De Mars G, Quirynen M, et al. A<br />
prospective split-mouth comparative study <strong>of</strong> two screw-shaped<br />
self-tapping pure titanium implant systems. Clin Oral <strong>Implant</strong>s<br />
Res. 2000;11:202-209.<br />
63. ten Bruggenkate CM, Asikainen P, Foitzik C, et al. Short (6-mm)<br />
nonsubmerged dental implants: results <strong>of</strong> a Multicenter clinical trial<br />
<strong>of</strong> 1 <strong>to</strong> 7 years. Int J Oral Maxill<strong>of</strong>ac <strong>Implant</strong>s. 1998;13:791-798.<br />
64. Bidez MW, Misch CE. Biomechanics. In: Misch CE.<br />
Contemporary <strong>Implant</strong> Dentistry. 3rd ed. St. Louis, MO:<br />
Mosby; 2008:557-598.<br />
65. Bidez MW, Misch CE. Force transfer in implant dentistry: basic<br />
concepts <strong>and</strong> principles. J Oral Implan<strong>to</strong>l. 1992;18:264-274.<br />
66. Misch CE, Bidez MW. <strong>Implant</strong>-protected occlusion: a<br />
biomechanical rationale. Compendium. 1994;15:1330-1334.<br />
67. Berglundh T, Persson L, Klinge B. A systematic review <strong>of</strong> the<br />
incidence <strong>of</strong> biological <strong>and</strong> technical complications in implant<br />
dentistry reported in prospective longitudinal studies <strong>of</strong> at least<br />
5 years. J Clin Periodon<strong>to</strong>l. 2002;29(suppl 3):197-212.<br />
68. Aglietta M, Siciliano VI, Zwahlen M, et al. A systematic<br />
review <strong>of</strong> the survival <strong>and</strong> complication rates <strong>of</strong> implant<br />
supported fixed dental prostheses with cantilever extensions<br />
after an observation period <strong>of</strong> at least 5 years. Clin Oral<br />
<strong>Implant</strong>s Res. 2009;20:441-451.<br />
69. Sanz M, Naert I; Working Group 2. Biomechanics/risk<br />
management (Working Group 2). Clin Oral <strong>Implant</strong>s Res.<br />
2009;20(suppl 4):107-111.<br />
70. Akça K, Iplikçio lu H. Finite element stress analysis <strong>of</strong> the<br />
effect <strong>of</strong> short implant usage in place <strong>of</strong> cantilever<br />
extensions in m<strong>and</strong>ibular posterior edentulism. J Oral<br />
Rehabil. 2002;29:350-356.<br />
71. Tawil G, Aboujaoude N, Younan R. Influence <strong>of</strong> prosthetic<br />
parameters on the survival <strong>and</strong> complication rates <strong>of</strong> short<br />
implants. Int J Oral Maxill<strong>of</strong>ac <strong>Implant</strong>s. 2006;21:275-282.<br />
11
POST EXAMINATION INFORMATION<br />
Continuing Education<br />
<strong>Importance</strong> <strong>of</strong> <strong>Crown</strong> <strong>to</strong> <strong>Root</strong> <strong>and</strong> <strong>Crown</strong> <strong>to</strong> <strong>Implant</strong> Ratios<br />
To receive continuing education credit for participation in<br />
this educational activity you must complete the program<br />
post examination <strong>and</strong> receive a score <strong>of</strong> 70% or better.<br />
Traditional Completion Option:<br />
You may fax or mail your answers with payment <strong>to</strong> Dentistry<br />
Today (see Traditional Completion Information on following<br />
page). All information requested must be provided in order<br />
<strong>to</strong> process the program for credit. Be sure <strong>to</strong> complete your<br />
“Payment,” “Personal Certification Information,” “Answers,”<br />
<strong>and</strong> “Evaluation” forms. Your exam will be graded within 72<br />
hours <strong>of</strong> receipt. Upon successful completion <strong>of</strong> the postexam<br />
(70% or higher), a letter <strong>of</strong> completion will be mailed<br />
<strong>to</strong> the address provided.<br />
Online Completion Option:<br />
Use this page <strong>to</strong> review the questions <strong>and</strong> mark your<br />
answers. Return <strong>to</strong> dentalce<strong>to</strong>day.com <strong>and</strong> sign in. If you<br />
have not previously purchased the program, select it from<br />
the “Online Courses” listing <strong>and</strong> complete the online<br />
purchase process. Once purchased the program will be<br />
added <strong>to</strong> your User His<strong>to</strong>ry page where a Take Exam link<br />
will be provided directly across from the program title.<br />
Select the Take Exam link, complete all the program<br />
questions <strong>and</strong> Submit your answers. An immediate grade<br />
report will be provided. Upon receiving a passing grade,<br />
complete the online evaluation form. Upon submitting the<br />
form your Letter Of Completion will be provided<br />
immediately for printing.<br />
General Program Information:<br />
Online users may log in <strong>to</strong> dentalce<strong>to</strong>day.com any time in<br />
the future <strong>to</strong> access previously purchased programs <strong>and</strong><br />
view or print letters <strong>of</strong> completion <strong>and</strong> results.<br />
POST EXAMINATION QUESTIONS<br />
1. Fac<strong>to</strong>rs which influence the number <strong>of</strong> abutments <strong>to</strong><br />
support a fixed dental prosthesis (FDP) include<br />
which <strong>of</strong> the following<br />
a. Number <strong>of</strong> missing teeth.<br />
b. Anticipated occlusal forces.<br />
c. Amount <strong>of</strong> available bone around abutments.<br />
d. All <strong>of</strong> the above.<br />
2. With respect <strong>to</strong> teeth, the following procedures<br />
reduce the CRRs:<br />
a. A low pr<strong>of</strong>ile overdenture abutment.<br />
b. Tooth extrusion.<br />
c. Both A <strong>and</strong> B.<br />
d. Occlusal onlays.<br />
3. Strategies <strong>to</strong> consider when fabricating fixed dental<br />
prostheses with increased CIRs include the<br />
following:<br />
a. Minimize lateral excursions on posterior prostheses<br />
<strong>and</strong> increase the number <strong>of</strong> supporting implants.<br />
b. Increase clinical crown height.<br />
c. Employ textured surfaced implants.<br />
d. Both A <strong>and</strong> C.<br />
4. In this review paper, the authors define the clinical<br />
crown as:<br />
a. The sum <strong>of</strong> the res<strong>to</strong>red crown plus the abutment<br />
collar plus the portion <strong>of</strong> the implant coronal <strong>to</strong> the<br />
bone.<br />
b. The height <strong>of</strong> the titanium abutment minus 2 mm for<br />
biologic width space.<br />
c. The sum <strong>of</strong> the interarch space plus the height <strong>of</strong> the<br />
res<strong>to</strong>red crown plus the height <strong>of</strong> the abutment.<br />
d. The height <strong>of</strong> the res<strong>to</strong>red crown.<br />
5. In the study <strong>of</strong> increased CIRs by Rossi, et al the<br />
assessed implants were:<br />
a. The 6-mm long implants.<br />
b. The 4.1-mm diameter implants <strong>and</strong> the 4.8-mm<br />
diameter implants.<br />
c. Splinted implants.<br />
d. Both A <strong>and</strong> B.<br />
6. To calculate the bending moment, it is necessary <strong>to</strong><br />
multiply the force by what<br />
a. The perpendicular distance (moment arm) from the<br />
fulcrum <strong>to</strong> the endpoint <strong>of</strong> the lever arm.<br />
b. The perpendicular distance (moment arm) from the<br />
fulcrum <strong>to</strong> the apex <strong>of</strong> the <strong>to</strong>oth.<br />
c. The perpendicular distance (moment arm) from the<br />
fulcrum <strong>to</strong> the cemen<strong>to</strong>-enamel junction.<br />
d. The perpendicular distance (moment arm) from the<br />
fulcrum <strong>to</strong> closest <strong>to</strong>oth.<br />
12
Continuing Education<br />
<strong>Importance</strong> <strong>of</strong> <strong>Crown</strong> <strong>to</strong> <strong>Root</strong> <strong>and</strong> <strong>Crown</strong> <strong>to</strong> <strong>Implant</strong> Ratios<br />
7. In the study pertaining <strong>to</strong> increased CIRs by Blanes,<br />
et al the assessed implants had which features<br />
a. Moni<strong>to</strong>red for 2.5 years.<br />
b. Res<strong>to</strong>red with CIRs <strong>of</strong> 6 or more.<br />
c. Smooth surfaced implants.<br />
d. None <strong>of</strong> the above.<br />
8. In this review paper, the authors define the location<br />
<strong>of</strong> the fulcrum between the clinical crown <strong>and</strong> the<br />
implant as:<br />
a. Occurring at the junction <strong>of</strong> the res<strong>to</strong>ration <strong>and</strong> the<br />
implant abutment.<br />
b. Occurring at the level <strong>of</strong> the first bone <strong>to</strong> implant<br />
contact.<br />
c. Occurring at the implant-abutment interface.<br />
d. Occurring within the body <strong>of</strong> the implant half way<br />
from the osseous crest <strong>to</strong> the apex <strong>of</strong> the implant.<br />
9. Fac<strong>to</strong>rs which will affect an implant’s ability <strong>to</strong> resist<br />
biologic <strong>and</strong> technical complications include:<br />
a. Increasing implant diameter.<br />
b. Use <strong>of</strong> porcelain fused <strong>to</strong> metal crowns.<br />
c. Splinting <strong>of</strong> implants, particularly across the turn <strong>of</strong><br />
the arch.<br />
d. Both A <strong>and</strong> C.<br />
10. Which procedures increase the CRR with respect <strong>to</strong><br />
teeth<br />
a. Increasing vertical dimension.<br />
b. Surgical crown lengthening.<br />
c. Both A <strong>and</strong> B.<br />
d. Ridge augmentation.<br />
11. Urdaneta, et al demonstrated that an increased CIR<br />
resulted in what effect on bone around the dental<br />
implants<br />
a. Additional bone loss.<br />
b. No additional bone loss.<br />
c. Bone apposition.<br />
d. Increased osseous density <strong>of</strong> bone.<br />
12. The preponderance <strong>of</strong> data in Table 3 indicate that<br />
short implants demonstrate which characteristic<br />
a. Are very successful <strong>and</strong> that survival rates for short<br />
textured implants are comparable <strong>to</strong> longer implants.<br />
b. Are very successful <strong>and</strong> that survival rates for short<br />
smooth surfaced implants are comparable <strong>to</strong> longer<br />
implants.<br />
c. Are not very successful <strong>and</strong> that survival rates for<br />
short textured implants are not comparable <strong>to</strong> longer<br />
implants.<br />
d. Are not very successful.<br />
13. According <strong>to</strong> Bidez <strong>and</strong> Misch, when a crown height<br />
is increased from 10 <strong>to</strong> 20 mm, the increase <strong>of</strong> force<br />
on an implant is how large<br />
a. 25%.<br />
b. 50%.<br />
c. 75%.<br />
d. 100%.<br />
14. The European Association for Osseointegration<br />
reached which <strong>of</strong> the following conclusions<br />
a. Res<strong>to</strong>rations with a CIR up <strong>to</strong> 2 do not induce periimplant<br />
bone loss.<br />
b. FDP or single-<strong>to</strong>oth res<strong>to</strong>ration with a CIR up <strong>to</strong> 2 is<br />
an acceptable prosthetic option.<br />
c. Both A <strong>and</strong> B.<br />
d. Res<strong>to</strong>rations with a CIR up <strong>to</strong> 1 do not induce periimplant<br />
bone loss.<br />
15. Techniques <strong>to</strong> reduce forces on res<strong>to</strong>rations with an<br />
increased CIR include which <strong>of</strong> the following<br />
a. Res<strong>to</strong>re the posterior occlusal surfaces <strong>of</strong> teeth so<br />
canine guidance discludes the posterior teeth<br />
<strong>and</strong> minimizes lateral contact in m<strong>and</strong>ibular<br />
excursions.<br />
b. Increase the number <strong>of</strong> implants supporting the<br />
prosthesis.<br />
c. Increase the bone implant contact area with wider<br />
implants.<br />
d. All <strong>of</strong> the above.<br />
16. What is the precise crown <strong>to</strong> implant ratio that<br />
cannot be exceeded <strong>to</strong> avoid deosseointegration or<br />
fracture <strong>of</strong> an implant<br />
a. Unknown.<br />
b. 1.<br />
c. 1.5.<br />
d. 2.<br />
13
Continuing Education<br />
<strong>Importance</strong> <strong>of</strong> <strong>Crown</strong> <strong>to</strong> <strong>Root</strong> <strong>and</strong> <strong>Crown</strong> <strong>to</strong> <strong>Implant</strong> Ratios<br />
PROGRAM COMPLETION INFORMATION<br />
PERSONAL CERTIFICATION INFORMATION:<br />
If you wish <strong>to</strong> purchase <strong>and</strong> complete this activity<br />
traditionally (mail or fax) rather than online, you must<br />
provide the information requested below. Please be sure <strong>to</strong><br />
select your answers carefully <strong>and</strong> complete the evaluation<br />
information. To receive credit you must answer at least 12 <strong>of</strong><br />
the 16 questions correctly.<br />
Complete online at: dentalce<strong>to</strong>day.com<br />
TRADITIONAL COMPLETION INFORMATION:<br />
Last Name (PLEASE PRINT CLEARLY OR TYPE)<br />
First Name<br />
Pr<strong>of</strong>ession / Credentials<br />
Street Address<br />
Suite or Apartment Number<br />
License Number<br />
Mail or fax this completed form with payment <strong>to</strong>:<br />
Dentistry Today<br />
Department <strong>of</strong> Continuing Education<br />
100 Passaic Avenue<br />
Fairfield, NJ 07004<br />
Fax: 973-882-3622<br />
PAYMENT & CREDIT INFORMATION:<br />
Examination Fee: $40.00 Credit Hours: 2.0<br />
Note: There is a $10 surcharge <strong>to</strong> process a check drawn on<br />
any bank other than a US bank. Should you have additional<br />
questions, please contact us at (973) 882-4700.<br />
❏ I have enclosed a check or money order.<br />
❏ I am using a credit card.<br />
My Credit Card information is provided below.<br />
❏ American Express ❏ Visa ❏ MC ❏ Discover<br />
Please provide the following (please print clearly):<br />
City State Zip Code<br />
Daytime Telephone Number With Area Code<br />
Fax Number With Area Code<br />
E-mail Address<br />
ANSWER FORM: COURSE #: 135<br />
Please check the correct box for each question below.<br />
1. ❏ a ❏ b ❏ c ❏ d 9. ❏ a ❏ b ❏ c ❏ d<br />
2. ❏ a ❏ b ❏ c ❏ d 10. ❏ a ❏ b ❏ c ❏ d<br />
3. ❏ a ❏ b ❏ c ❏ d 11. ❏ a ❏ b ❏ c ❏ d<br />
4. ❏ a ❏ b ❏ c ❏ d 12. ❏ a ❏ b ❏ c ❏ d<br />
5. ❏ a ❏ b ❏ c ❏ d 13. ❏ a ❏ b ❏ c ❏ d<br />
6. ❏ a ❏ b ❏ c ❏ d 14. ❏ a ❏ b ❏ c ❏ d<br />
7. ❏ a ❏ b ❏ c ❏ d 15. ❏ a ❏ b ❏ c ❏ d<br />
8. ❏ a ❏ b ❏ c ❏ d 16. ❏ a ❏ b ❏ c ❏ d<br />
Exact Name on Credit Card<br />
Credit Card #<br />
Signature<br />
Approved PACE Program Provider<br />
FAGD/MAGD Credit Approval<br />
does not imply acceptance<br />
by a state or provincial board <strong>of</strong><br />
dentistry or AGD endorsement.<br />
June 1, 2009 <strong>to</strong> May 31, 2012<br />
AGD Pace approval number: 309062<br />
/<br />
Expiration Date<br />
Dentistry Today, Inc, is an ADA CERP Recognized<br />
Provider. ADA CERP is a service <strong>of</strong> the American<br />
Dental Association <strong>to</strong> assist dental pr<strong>of</strong>essionals in<br />
indentifying quality providers <strong>of</strong> continuing dental<br />
education. ADA CERP does not approve or endorse<br />
individual courses or instruc<strong>to</strong>rs, nor does it imply<br />
acceptance <strong>of</strong> credit hours by boards <strong>of</strong> dentistry.<br />
Concerns or complaints about a CE provider may be<br />
directed <strong>to</strong> the provider or <strong>to</strong> ADA CERP at<br />
ada.org/go<strong>to</strong>/cerp.<br />
14<br />
PROGRAM EVAUATION FORM<br />
Please complete the following activity evaluation questions.<br />
Rating Scale: Excellent = 5 <strong>and</strong> Poor = 0<br />
Course objectives were achieved.<br />
Content was useful <strong>and</strong> benefited your<br />
clinical practice.<br />
Review questions were clear <strong>and</strong> relevant<br />
<strong>to</strong> the edi<strong>to</strong>rial.<br />
Illustrations <strong>and</strong> pho<strong>to</strong>graphs were<br />
clear <strong>and</strong> relevant.<br />
Written presentation was informative<br />
<strong>and</strong> concise.<br />
How much time did you spend reading<br />
the activity <strong>and</strong> completing the test