Orange-Yellow Tongue and Palate: A Case Report - DentalCEToday
Orange-Yellow Tongue and Palate: A Case Report - DentalCEToday
Orange-Yellow Tongue and Palate: A Case Report - DentalCEToday

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Continuing EducationCourse Number: 147.2<strong>Orange</strong>-<strong>Yellow</strong> <strong>Tongue</strong><strong>and</strong> <strong>Palate</strong>:A <strong>Case</strong> <strong>Report</strong>Authored by Stephen A. Harden, DDS; Aamir Sheikh, DDS, MA; <strong>and</strong>Ronald S. Brown, DDS, MSUpon successful completion of this CE activity 1 CE credit hour may be awardedA Peer-Reviewed CE Activity byDentistry Today, Inc, is an ADA CERP Recognized Provider. ADA CERP isa service of the American Dental Association to assist dental professionalsin indentifying quality providers of continuing dental education. ADA CERPdoes not approve or endorse individual courses or instructors, nor does itimply acceptance of credit hours by boards of dentistry. Concerns orcomplaints about a CE provider may be directed to the provider or toADA CERP at ada.org/goto/cerp.Approved PACE Program ProviderFAGD/MAGD Credit Approvaldoes not imply acceptanceby a state or provincial board ofdentistry or AGD endorsement.June 1, 2009 to May 31, 2012AGD Pace approval number: 309062Opinions expressed by CE authors are their own <strong>and</strong> may not reflect those of Dentistry Today. Mention ofspecific product names does not infer endorsement by Dentistry Today. Information contained in CE articles <strong>and</strong>courses is not a substitute for sound clinical judgment <strong>and</strong> accepted st<strong>and</strong>ards of care. Participants are urged tocontact their state dental boards for continuing education requirements.
Continuing Education<strong>Orange</strong>-<strong>Yellow</strong> <strong>Tongue</strong> <strong>and</strong> <strong>Palate</strong>:A <strong>Case</strong> <strong>Report</strong>Effective Date: 03/1/2012 Expiration Date: 03/1/2015LEARNING OBJECTIVESAfter participating in this CE activity, the individual will learn:• Drugs, conditions, <strong>and</strong> diseases known to cause oralmucosal pigmentation.• Characteristics of carotenemia, xanthoderma, dermalpigmentation, <strong>and</strong> carotene <strong>and</strong> vitamin A analoguetoxicity issues.ABOUT THE AUTHORSDr. Harden is assistant professor,department of restorative dentistry,Howard University College of Dentistry,Washington, DC. He can be reached atsharden@howard.edu.Disclosure: Dr. Harden reports no disclosures.Dr. Sheikh is assistant professor,department of oral diagnostic services,Howard University College of Dentistry,Washington, DC. He can be reached atasheikh@howard.edu.Disclosure: Dr. Sheikh reports no disclosures.Dr. Brown is professor, department oforal diagnostic services, HowardUniversity College of Dentistry, <strong>and</strong>clinical associate professor, departmentof otolaryngology, Georgetown UniversityMedical Center, Washington, DC. Hecan be reached at rbrown@howard.edu.Disclosure: Dr. Brown reports no disclosures.INTRODUCTIONA number of drug therapies have a previously reportedassociation with drug-induced pigmentation of the oralmucosa. These drugs include antimalarials such asquinacrine, chloroquine, hydroxychloroquine, quinidine,zidovudine, tetracycline, minocycline, chlorpromazine, oralcontraceptives, clofazimine, ketoconazole, amiodarone,busulfan, doxorubicin, bleomycin, cylo phos phamide, <strong>and</strong>5-fluoroura cil. 1,2 Quinine antimalarial drugs are associatedwith blue-gray or blue-black coloring which is usually locatedonly within the palate. The reason for the palatal location ofthe discoloration is currently not un derstood. Mino cycline isknown to cause pigmentation of the alveolar bone, <strong>and</strong>the clinical appearance dem on strates a gray discolor ationof the oral mucosa. Mi nocycline has also been reportedto cause discoloration of the tongue. Further more,documentation of oral mucosa discolor ation in cludesdiffuse, bilateral, <strong>and</strong> focal presentations. These in cludephysiologic pigmentation, Peutz-Jeghers syndrome,Addison’s disease, heavy metal pigmentation, Ka posi’ssarcoma, postinflammatory pigmentation, smoker’s mela -nosis, <strong>and</strong> such focal presentations as hemangioma, varix,thrombus, hematoroma, amalgam tattoo, blue nevus,melanotic macule, pigmented nevus, melano-acanthoma,mel ano ma, black hairy tongue, <strong>and</strong> vitilago. 1,3,4Carotenemia, an increased level of serum carotene, isknown to cause discoloration of the skin, xanthoderma, <strong>and</strong>particularly the palms of the h<strong>and</strong>s <strong>and</strong> the soles of the feet.Boere <strong>and</strong> Hoskam 5 reported a case in which the individualwas noted for a striking yellow discoloration of the palms of theh<strong>and</strong>s <strong>and</strong> the plantar area of the feet. Furthermore, highperformanceliquid chromatography reported a value of serumbeta-carotene at 1.16 micromol when the normal values arebetween 0.07 <strong>and</strong> 0.88. Takita et al 6 reported a case ofcarotenemia secondary to beta-carotene supplementation.Their patient, a 66-year-old female, consumed 5.72 mg ofbeta-carotene daily for 3 months. The patient’s palms <strong>and</strong>soles were noted for orange-yellow coloration. Stack et al 7 alsoreported a case with yellow-orange coloration of the palms <strong>and</strong>soles. Their patient, a 29-year-old male from Liberia, had ahistory of regularly consuming red-palm oil which is rich inbeta-carotene. Arya et al 8 reported that carotenemia is a1
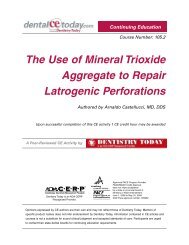
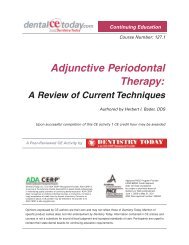
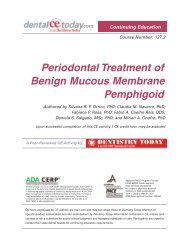
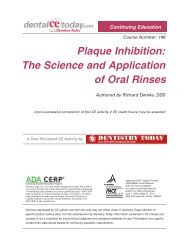
elatively common pediatric condition of yellowing ofthe skin <strong>and</strong> elevated serum beta-carotene values<strong>and</strong> is associated with metabolic disorders due toimmature liver function. All of the patients reportedabove were negative for scleral icterus <strong>and</strong> positive forelevated serum bilirubin values.This article presents a case report that representsthe first reported case of oral mucosal discoloration(of the dorsal tongue <strong>and</strong> palate) secondary to car ot -emia due to a topical retinoid pharmaco therapeutic.CASE REPORTA 59-year-old female was referred by herotolaryngologist to an oral medicine clinician with achief complaint of “orange tongue.” The patient notedthat other areas of the mouth were also orange, suchas the palate. The otolaryngologist previouslyperformed a fungal culture procedure of the area <strong>and</strong>the report was negative for fungal infectiveorganisms. The physician also suggested that thepatient use a tongue scraper, <strong>and</strong> prescribed magicmouthrinse. Magic mouthrinse is comprised ofnystatin, diphenhydramine, lidocaine, <strong>and</strong> sometimestriamcinolone. Neither the tongue scraping nor themouthrinse improved the condition. The patient utilized adilute vinegar solution, also without success. The patienthad been using one toothpaste with an antitartar(triclosan) agent <strong>and</strong> had recently switched to anothertoothpaste also containing an antitartar agent.The medical history noted that the patient had beenusing such skin cream medications as Tretinoin cream0.05%. The patient did not smoke cigarettes <strong>and</strong> drankalcohol only rarely. She was taking simvastatin forcholesterol lowering. She was taking such over-the-countermedications <strong>and</strong> supplements as fish oil, as pirin (81 mg),<strong>and</strong> calcium. She sometimes used such sleep aids aszaleplon <strong>and</strong> zolpidem. The patient reported a previousdrug allergy reaction to ciprofloxacin, but noted no otherknown drug allergies.Clinically, palpation for lympha den opathy was negative.The parotid <strong>and</strong> subm<strong>and</strong>ibular salivary gl<strong>and</strong>sdemonstrated limited function. The filiform papillae of thedorsal tongue <strong>and</strong> the midline portion of the soft palate hadContinuing Education<strong>Orange</strong>-<strong>Yellow</strong> <strong>Tongue</strong> <strong>and</strong> <strong>Palate</strong>: A <strong>Case</strong> <strong>Report</strong>Figure 1. Photograph illustrating an orange-yellow appearance of the dorsaltongue <strong>and</strong> soft palate.an orange-yellow tinge (Figure 1). The remaining oral tissuesappeared to be within normal limits. The skin color <strong>and</strong> theeye coloration also appeared to be within normal limits.As the patient was using a vitamin A/carotene analogue,the most likely (tentative/working) diagnosis was carotenemia,which is defined as an increased body burden of beta-car -otene <strong>and</strong> carotenosis/carotenoderma/xanthoderma, which isorange-yellow coloration secondary to caro tenemia. Thedifferential diagnosis for orange or yellow discoloration of theoral mucosa includes jaundice, fungal infection, <strong>and</strong>malakoplakia. As a trial therapy, the clinician advised thepatient to discontinue the antiwrinkle cream, which containeda vitamin A analogue. In one month, the color of the tonguefaded from orange-yellow back to a healthy pink. This wasreported by the patient <strong>and</strong> confirmed with photographstaken by the patient’s husb<strong>and</strong> (at a later date) (Figure 2).DISCUSSIONCarotenemia <strong>and</strong> secondary xanthoderma (discoloration ofthe epidermis) can be caused by a diet with excessiveamounts of carotene-rich foods such as carrots, <strong>and</strong> by2
Continuing Education<strong>Orange</strong>-<strong>Yellow</strong> <strong>Tongue</strong> <strong>and</strong> <strong>Palate</strong>: A <strong>Case</strong> <strong>Report</strong>supplements <strong>and</strong> medications which contain carotene orretinoids. Caroten oids are fat soluble <strong>and</strong> are deposited inthe intercellular lipids of the stratum corneum. 9 Qui nineantimalarial drugs are associated with discoloration of thepalate. Pos sibly, the stratum corneum of the palate is ananatomical location with an affinity for lipid-basedpharmacotherapeutics. Therefore, the route of drugadministration (oral versus topical) may have stronglyinfluenced the location of the epitheal discoloration.Lascari 10 reported that it is important for clinicians to beaware of the differences between jaundice <strong>and</strong>carotenemia. Ingestion of excessive amounts of carrots <strong>and</strong>also several other yellow as well as green vegetables is theusual cause of carotenemia. Fur thermore, there is thepotential of parents to un knowingly contribute tocarotenemia by providing commercial infant foodcombinations to newborns. How ever, carotenemia is atypically a be nign condition as poisoning due to vitamin A isslow <strong>and</strong> usually re versible.Serum carotene levels were not ordered for thepresented case because the condition improved with theelimination of the topical medication.Boere <strong>and</strong> Hoskam 5 reported that their patient’scondition was due to beta-carotene in the diet <strong>and</strong> waspossibly influenced by the patient’s type 2 diabeticcondition. According to Hoe rer et al, 11 there is anassociation be tween carotenemia <strong>and</strong> diabetes, al thoughin the case reported the pa tient did not have a diabetichistory. Possibly, the case reported demon stra ted thechange in normal color ation due to the proximity of thetopical application of the antiwrinkle car otene-containingcream to the oral tissues. The other noted cases ofcarotenemia/xanthoderma were all secondary to ingestionof particular vitamin A inclusive foods or vitamin Asupplements, rather than topical application.The negative culture assays by the otolaryngologisttended to rule out a diagnosis of fungal infection. Bor et al 12reported a case of an Aspergillus flavus infection in a childsecondary to acute lymphoblastic leukemia. The child had ayellow-white lesion of the lateral tongue which wassuccessfully treated with amphotericin B. Kitami et al 13reported a case of a 72-year-old male with a history ofsteroid <strong>and</strong> antibiotic utilization with a curdlike substance onFigure 2.Photograph illustratinga return to a morenormal oral colorationafter the discontinuationof the retinoid topicalcream.the surface of the tongue <strong>and</strong> lower lip. The diagnosis oforal sycosis c<strong>and</strong>idiasis was made with KOH-positivemicroscopic examination. Furthermore, the biopsy samplewas cultured <strong>and</strong> revealed C<strong>and</strong>ida albicans <strong>and</strong> C<strong>and</strong>idaparapsilos. The patient was successfully treated withamphotericin B syrup along with oral itraconazole <strong>and</strong> 2%miconzole gel. Rippon et al 14 reported a golden orangedorsal tongue lesion in a 54-year-old woman being treatedfor lymphocytic leukemia. The clinicians performed a biopsy<strong>and</strong> culture <strong>and</strong> determined the infective organism wasRamichloridium schulzeri (an un commonly encounteredsoil saprophyte). The clinicians treated the patient withnystatin, sulfamethoxazole, trimethoprim sulfate, <strong>and</strong>eventually amphotericin B therapy. How ever, the patientdied secondary to her leukemia condition compounded byneutropenia, <strong>and</strong> disseminated A flavus infection.The relative good health of the patient in the presentedcase, <strong>and</strong> the negative culture attained by the referringotolaryngologist, tended to rule out an oral fungal infectionas the etiology in the present case.Jaundice (icterus) is the yellowing skin color secondaryto increased bilirubin levels within the serum, known ashyperbilirubinemia. When the yellowish tinge becomesvisible, the concentration of bilirubin in plasma exceeds 1.5mg/dL, which is 3 times the normal value of 0.5 mg/dL.Typically, the skin in fair-skinned individuals takes on ayellowish tinge, <strong>and</strong> in jaundiced patients the sclera of theeyes have a yellowish appearance. 15,16 The condition of3
Continuing Education<strong>Orange</strong>-<strong>Yellow</strong> <strong>Tongue</strong> <strong>and</strong> <strong>Palate</strong>: A <strong>Case</strong> <strong>Report</strong>jaundice is secondary to obstruction of the biliary tract orsuch disease states as hepatitis <strong>and</strong> cancer of the liver.In the case reported, neither the patient’s skin nor eyesappeared to be yellow. Furthermore, there was no history ofliver disease or any history consistent with liver disease.There fore, blood studies to evaluate the patient’s bilirubinserum level were not undertaken.Several cases of jaundice have been reported in whichthe patient has a coated tongue secondary to c<strong>and</strong>idiasis,but the tongue or the palate is not involved in yellowingassociated with jaundice. 15-17Malakoplakia is a relatively un common chronicinflammatory reaction of unknown cause. Rarely, thiscondition may involve the tongue as a tongue mass withpossible discoloring. The most common lesion location sitesfor this condition are primarily the genitourinary tract <strong>and</strong>secondarily the gastrointestinal tract <strong>and</strong> retroperitoneum.Other less common sites include the tongue, lungs, bones,larynx, palatine tonsil, <strong>and</strong> parotid salivary gl<strong>and</strong>. Theprevalent etiological hypothesis is that a reaction oc curssecondary to an infectious agent within a patient with animmunologic deficiency. The diagnosis is confirmed with abiopsy <strong>and</strong> histopathologic evaluation determining thepresence of foamy histocytes with distinctive basophilicinclusions which are known as Michaelis-Gutmann bodies,which are due to partially ingested bacteria. Treatmentcombines antibiotic therapy such as quinolones <strong>and</strong>trimetoprim-sulpha meethoxazol with the surgical re moval ofthe lesion. 18The clinical findings in the presented case were notconsistent with a diagnosis of malakoplakia.Primary carotenoderma is that developing fromincreased oral ingestion of carotenoids, whereas secondarycarotenoderma is caused from underlying disease states(or metabolic dysfunction) that increase serum carotenoidswith normal oral intake of these compounds. Primary <strong>and</strong>secondary carotenoderma can coexist in the same patient.Although extensive amounts of vitamin A can manifest asan overdose with potential lethality, typically carotenemia isa benign condition. Carotenoderma is deliberately causedby beta-carotenoid treatment of certain photosensitivedermatitis diseases such as erythropoietic protoporphyria,where beta carotene is prescribed in quantities whichdiscolor the skin. These high doses of beta-carotene arebenign, although the orange appearance is displeasing tosome. In a recent meta-analysis of these therapies,however, the efficacy of the treatment is questionable. 19The patient in the presented case was informed that themost probable cause of the oral orange-yellow colorationwas the antiwrinkle skin cream containing beta-carotene.Fur thermore, the patient was informed that the efficacy ofthe skin cream formulation was controversial 20 <strong>and</strong> thatbeta-carotene supplements are associated with a numberof negative health consequences, including an increasedincidence of cancer <strong>and</strong> an increased mortality rate. 21-23The patient agreed to discontinue the use of the skincream, <strong>and</strong> her discoloration condition resolved within onemonth. As noted above, Lascari 10 reported that theabsence of yellow pigment in the sclera <strong>and</strong> oral cavitiesdistinguishes carotenemia from jaundice. However, the usualcauses of carotenemia/xanthoderma are through thedigestive system port of entry, while in this unusual case,the car otene was applied topically to the facial skin, whichwould tend to ac count for the oral location of thediscoloration. Further more, this case may serve to alerthealthcare pro viders to the possibility of discolorationsecondary to the administration of topical medications.CONCLUSIONA unique case has been presented in which an orangeyelloworal discolor ation was attributed to the use of acarotene-containing skin cream which was applied to thefacial skin. This case serves to alert clinicians that theadministration of certain topical medications may causediscoloration of the skin <strong>and</strong>/or oral mucosa.4
Continuing Education<strong>Orange</strong>-<strong>Yellow</strong> <strong>Tongue</strong> <strong>and</strong> <strong>Palate</strong>: A <strong>Case</strong> <strong>Report</strong>REFERENCES1. Kauzman A, Pavone M, Blanas N, et al. Pigmentedlesions of the oral cavity: review, differential diagnosis,<strong>and</strong> case presentations. J Can Dent Assoc.2004;70:682-683.2. Kleinegger CL, Hammond HL, Finkelstein MW. Oralmucosal hyperpigmentation secondary to antimalarialdrug therapy. Oral Surg Oral Med Oral Pathol OralRadiol Endod. 2000;90:189-194.3. Lawoyin D, Brown RS. Drug-induced black hairytongue: diagnosis <strong>and</strong> management challenges.Dent Today. 2008;27:60,62-63.4. Lawoyin DO, Brown RS, Reid E, et al. Concurrentpresentation of cutaneous <strong>and</strong> oral soft tissue vitiligo:a case report <strong>and</strong> literature review. ispub.com/journal/the-internet-journal-of-dental-science/volume-5-number-2/concurrent-presentation-of-cutaneous-<strong>and</strong>-oral-softtissue-vitiligo-a-case-report-<strong>and</strong>-literature-review.html.Accessed December 30, 2011.5. Boere IA, Hoskam JA. <strong>Yellow</strong> discolouration. NethJ Med. 2006;64:207.6. Takita Y, Ichimiya M, Hamamoto Y, et al. A case ofcarotenemia associated with ingestion of nutrientsupplements. J Dermatol. 2006;33:132-134.7. Stack KM, Churchwell MA, Skinner RB Jr.Xanthoderma: case report <strong>and</strong> differential diagnosis.Cutis. 1988;41:100-102.8. Arya V, Grzybowski J, Schwartz RA. Carotenemia.Cutis. 2003;71:441-442,448.9. Corrales Padilla H. Polymorphic light dermatitis.Photobiology <strong>and</strong> photoprotection [in Spanish].Med Cutan Ibero Lat Am. 1976;4:45-52.10. Lascari AD. Carotenemia. A review. Clin Pediatr(Phila). 1981;20:25-29.11. Hoerer E, Dreyfuss F, Herzberg M. Carotenemic, skincolour <strong>and</strong> diabetes mellitus. Acta Diabetol Lat.1975;12(3-4):202-207.12. Bor O, Cagri Dinleyici E, Kiraz N, et al. Successfultreatment of tongue aspergillosis caused byAspergillus flavus with liposomal amphotericin B in achild with acute lymphoblastic leukemia. Med Mycol.2006;44:767-770.13. Kitami Y, Kagawa S, Iijima M. <strong>Case</strong> of sycosisc<strong>and</strong>idiasis on the upper lip [in Japanese]. NihonIshinkin Gakkai Zasshi. 2008;49:81-86.14. Rippon JW, Arnow PM, Larson RA, et al. ‘Goldentongue’ syndrome caused by Ramichloridiumschulzeri. Arch Dermatol. 1985;121:892-894.15. Maharshak N, Shapiro J, Trau H. Carotenoderma—a review of the current literature. Int J Dermatol.2003;42:178-181.16. Pelletier LL, Borel DM, Romig DA, et al. Disseminatedintravascular coagulation <strong>and</strong> hepatic necrosis.Complications of infectious mononucleosis. JAMA.1976;235:1144-1146.17. Mahmood BA. Typhoid hepatitis: two case reports.Bangladesh Med Res Counc Bull. 1989;15:12-14.18. Alvarez Gómez GJ, Marín Botero ML, Henao CalleCA, et al. Malacoplakia: case report in tongue <strong>and</strong>review of the literature. Med Oral Patol Oral Cir Bucal.2008;13:E352-E354.19. Minder EI, Schneider-Yin X, Steurer J, et al. Asystematic review of treatment options for dermalphotosensitivity in erythropoietic protoporphyria.Cell Mol Biol (Noisy-le-gr<strong>and</strong>). 2009;55:84-97.20. Bayerl CH. Beta-carotene in dermatology: Does ithelp? Acta Dermatovenerol Alp Panonica Adriat.2008;17:160-162, 164-166.21. Brown RS, Glascoe A, Feimster T, et al. Vitamins <strong>and</strong>the treatment of oral <strong>and</strong> dental diseases. Dent Today.2010;29:51-57.22. Touger-Decker R. Vitamin <strong>and</strong> mineral supplements:what is the dentist to do? J Am Dent Assoc.2007;138:1222-1226.23. Schwartz JL, Shklar G. Retinoid <strong>and</strong> carotenoidangiogenesis: a possible explanation for enhancedoral carcinogenesis. Nutr Cancer. 1997;27:192-199.5
Continuing Education<strong>Orange</strong>-<strong>Yellow</strong> <strong>Tongue</strong> <strong>and</strong> <strong>Palate</strong>: A <strong>Case</strong> <strong>Report</strong>POST EXAMINATION INFORMATIONTo receive continuing education credit for participation inthis educational activity you must complete the programpost examination <strong>and</strong> receive a score of 70% or better.Traditional Completion Option:You may fax or mail your answers with payment to DentistryToday (see Traditional Completion Information on followingpage). All information requested must be provided in orderto process the program for credit. Be sure to complete your“Payment,” “Personal Certification Information,” “Answers,”<strong>and</strong> “Evaluation” forms. Your exam will be graded within 72hours of receipt. Upon successful completion of the postexam(70% or higher), a letter of completion will be mailedto the address provided.Online Completion Option:Use this page to review the questions <strong>and</strong> mark youranswers. Return to dentalcetoday.com <strong>and</strong> sign in. If youhave not previously purchased the program, select it fromthe “Online Courses” listing <strong>and</strong> complete the onlinepurchase process. Once purchased the program will beadded to your User History page where a Take Exam linkwill be provided directly across from the program title.Select the Take Exam link, complete all the programquestions <strong>and</strong> Submit your answers. An immediate gradereport will be provided. Upon receiving a passing grade,complete the online evaluation form. Upon submittingthe form, your Letter Of Completion will be providedimmediately for printing.General Program Information:Online users may log in to dentalcetoday.com any time inthe future to access previously purchased programs <strong>and</strong>view or print letters of completion <strong>and</strong> results.POST EXAMINATION QUESTIONS1. Blue-gray <strong>and</strong> blue-black oral mucosal discolorationis associated with _______.a. Oral contraceptives.b. Zidovudine.c. Antimalarial drugs.d. Cyclophosphamide.2. Which of the antibiotics below is associated withpigmentation of the alveolar bone <strong>and</strong> a graydiscoloration of the oral mucosa?a. Penicillin.b. Clindamycin.c. Erythromycin.d. Minocycline.3. An example of physiologic oral pigmentationsecondary to a disease or condition would be _______.a. Pneumonia.b. Peutz-Jeghers syndrome.c. Papillon-Lefèvre syndrome.d. Osteogenesis Imperfecta.4. Taking high doses of carotene <strong>and</strong>/or vitamin Aanalogues may result in _______.a. Carotenemia.b. Vitalago.c. Pigmented nevus.d. Melanotic macule.5. Xanthoderma is associated with orange-yellowpigmentation of the _______.a. Face.b. Palms <strong>and</strong> soles.c. Trunk.d. Eyes.6. Jaundice is known for yellowing of the skin <strong>and</strong> eyes<strong>and</strong> is associated with increased serum _______.a. Albumin.b. Glucose.c. Bilirubin.d. Melanin.7. Malakoplakia is diagnosed with a biopsy <strong>and</strong> thesignificant histopathological finding of partiallyingested bacteria is known as _______.a. Acid fast staining.b. Michaelis-Gutmann bodies.c. Lipshutz bodies.d. Donovan bodies.8. Which of the statements below is the most correct?a. Beta-carotene has no known toxicity.b. Beta-carotene is extremely toxic.c. Beta-carotene has demonstrated success in thetreatment of oral cancer.d. Increased beta-carotene supplementation is associatedwith decreased life span <strong>and</strong> increased cancer.6
Continuing Education<strong>Orange</strong>-<strong>Yellow</strong> <strong>Tongue</strong> <strong>and</strong> <strong>Palate</strong>: A <strong>Case</strong> <strong>Report</strong>PROGRAM COMPLETION INFORMATIONPERSONAL CERTIFICATION INFORMATION:If you wish to purchase <strong>and</strong> complete this activitytraditionally (mail or fax) rather than online, you mustprovide the information requested below. Please be sure toselect your answers carefully <strong>and</strong> complete the evaluationinformation. To receive credit you must answer at least 6 ofthe 8 questions correctly.Complete online at: dentalcetoday.comTRADITIONAL COMPLETION INFORMATION:Last Name (PLEASE PRINT CLEARLY OR TYPE)First NameProfession / CredentialsStreet AddressSuite or Apartment NumberLicense NumberMail or fax this completed form with payment to:Dentistry TodayDepartment of Continuing Education100 Passaic AvenueFairfield, NJ 07004Fax: 973-882-3622City State Zip CodeDaytime Telephone Number With Area CodeFax Number With Area CodeE-mail AddressPAYMENT & CREDIT INFORMATION:Examination Fee: $20.00 Credit Hours: 1.0Note: There is a $10 surcharge to process a check drawn onany bank other than a US bank. Should you have additionalquestions, please contact us at (973) 882-4700.❏ I have enclosed a check or money order.❏ I am using a credit card.My Credit Card information is provided below.❏ American Express ❏ Visa ❏ MC ❏ DiscoverANSWER FORM: COURSE #: 147.2Please check the correct box for each question below.1. ❏ a ❏ b ❏ c ❏ d 5. ❏ a ❏ b ❏ c ❏ d2. ❏ a ❏ b ❏ c ❏ d 6. ❏ a ❏ b ❏ c ❏ d3. ❏ a ❏ b ❏ c ❏ d 7. ❏ a ❏ b ❏ c ❏ d4. ❏ a ❏ b ❏ c ❏ d 8. ❏ a ❏ b ❏ c ❏ dPlease provide the following (please print clearly):Exact Name on Credit CardCredit Card #SignatureApproved PACE Program ProviderFAGD/MAGD Credit Approvaldoes not imply acceptanceby a state or provincial board ofdentistry or AGD endorsement.June 1, 2009 to May 31, 2012AGD Pace approval number: 309062/Expiration DateDentistry Today, Inc, is an ADA CERP RecognizedProvider. ADA CERP is a service of the AmericanDental Association to assist dental professionals inindentifying quality providers of continuing dentaleducation. ADA CERP does not approve or endorseindividual courses or instructors, nor does it implyacceptance of credit hours by boards of dentistry.Concerns or complaints about a CE provider may bedirected to the provider or to ADA CERP atada.org/goto/cerp.PROGRAM EVAUATION FORMPlease complete the following activity evaluation questions.Rating Scale: Excellent = 5 <strong>and</strong> Poor = 0Course objectives were achieved.Content was useful <strong>and</strong> benefited yourclinical practice.Review questions were clear <strong>and</strong> relevantto the editorial.Illustrations <strong>and</strong> photographs wereclear <strong>and</strong> relevant.Written presentation was informative<strong>and</strong> concise.How much time did you spend readingthe activity <strong>and</strong> completing the test?7