May 2011 Dear Parents: It is hard to believe that this school year is ...
May 2011 Dear Parents: It is hard to believe that this school year is ...
May 2011 Dear Parents: It is hard to believe that this school year is ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
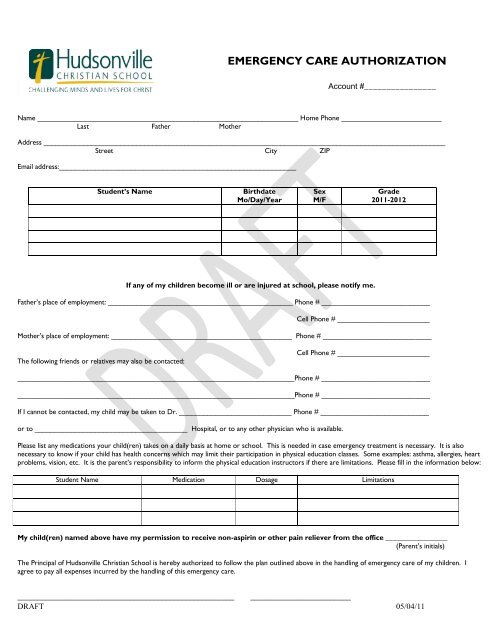
EMERGENCY CARE AUTHORIZATION<br />
Account #________________<br />
Name _________________________________________________________________ Home Phone _________________________<br />
Last Father Mother<br />
Address ____________________________________________________________________________________________________<br />
Street City ZIP<br />
Email address:___________________________________________________________<br />
Student’s Name<br />
Birthdate<br />
Mo/Day/Year<br />
Sex<br />
M/F<br />
Grade<br />
<strong>2011</strong>-2012<br />
If any of my children become ill or are injured at <strong>school</strong>, please notify me.<br />
Father‟s place of employment: ______________________________________________ Phone # ___________________________<br />
Cell Phone # _______________________<br />
Mother‟s place of employment: _____________________________________________ Phone # ___________________________<br />
The following friends or relatives may also be contacted:<br />
Cell Phone # _______________________<br />
_____________________________________________________________________Phone # ___________________________<br />
_____________________________________________________________________Phone # ___________________________<br />
If I cannot be contacted, my child may be taken <strong>to</strong> Dr. ____________________________ Phone # ___________________________<br />
or <strong>to</strong> ______________________________________ Hospital, or <strong>to</strong> any other physician who <strong>is</strong> available.<br />
Please l<strong>is</strong>t any medications your child(ren) takes on a daily bas<strong>is</strong> at home or <strong>school</strong>. Th<strong>is</strong> <strong>is</strong> needed in case emergency treatment <strong>is</strong> necessary. <strong>It</strong> <strong>is</strong> also<br />
necessary <strong>to</strong> know if your child has health concerns which may limit their participation in physical education classes. Some examples: asthma, allergies, heart<br />
problems, v<strong>is</strong>ion, etc. <strong>It</strong> <strong>is</strong> the parent‟s responsibility <strong>to</strong> inform the physical education instruc<strong>to</strong>rs if there are limitations. Please fill in the information below:<br />
Student Name Medication Dosage Limitations<br />
My child(ren) named above have my perm<strong>is</strong>sion <strong>to</strong> receive non-aspirin or other pain reliever from the office _________________<br />
(Parent‟s initials)<br />
The Principal of Hudsonville Chr<strong>is</strong>tian School <strong>is</strong> hereby authorized <strong>to</strong> follow the plan outlined above in the handling of emergency care of my children. I<br />
agree <strong>to</strong> pay all expenses incurred by the handling of th<strong>is</strong> emergency care.<br />
______________________________________________________ _________________________<br />
DRAFT 05/04/11