Urology referral form - Nwlcn.nhs.uk
Urology referral form - Nwlcn.nhs.uk
Urology referral form - Nwlcn.nhs.uk

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
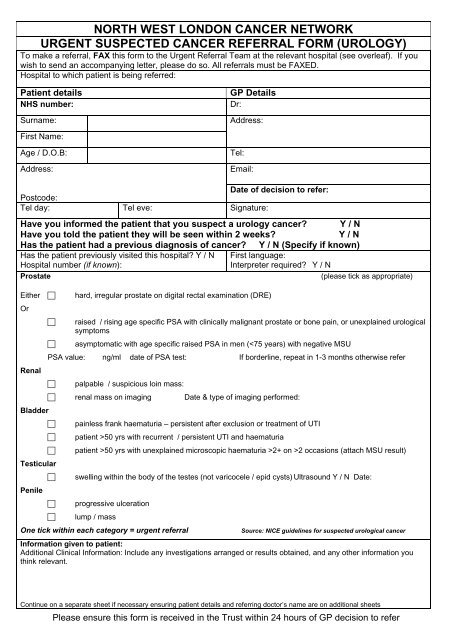
NORTH WEST LONDON CANCER NETWORK<br />
URGENT SUSPECTED CANCER REFERRAL FORM (UROLOGY)<br />
To make a <strong>referral</strong>, FAX this <strong>form</strong> to the Urgent Referral Team at the relevant hospital (see overleaf). If you<br />
wish to send an accompanying letter, please do so. All <strong>referral</strong>s must be FAXED.<br />
Hospital to which patient is being referred:<br />
Patient details<br />
NHS number:<br />
Surname:<br />
GP Details<br />
Dr:<br />
Address:<br />
First Name:<br />
Age / D.O.B:<br />
Address:<br />
Tel:<br />
Email:<br />
Date of decision to refer:<br />
Postcode:<br />
Tel day: Tel eve: Signature:<br />
Have you in<strong>form</strong>ed the patient that you suspect a urology cancer Y / N<br />
Have you told the patient they will be seen within 2 weeks<br />
Y / N<br />
Has the patient had a previous diagnosis of cancer Y / N (Specify if known)<br />
Has the patient previously visited this hospital Y / N<br />
Hospital number (if known):<br />
First language:<br />
Interpreter required Y / N<br />
Prostate<br />
(please tick as appropriate)<br />
Either <br />
Or<br />
Renal<br />
<br />
<br />
hard, irregular prostate on digital rectal examination (DRE)<br />
raised / rising age specific PSA with clinically malignant prostate or bone pain, or unexplained urological<br />
symptoms<br />
asymptomatic with age specific raised PSA in men (50 yrs with recurrent / persistent UTI and haematuria<br />
patient >50 yrs with unexplained microscopic haematuria >2+ on >2 occasions (attach MSU result)<br />
Testicular<br />
swelling within the body of the testes (not varicocele / epid cysts) Ultrasound Y / N Date:<br />
Penile<br />
progressive ulceration<br />
lump / mass<br />
One tick within each category = urgent <strong>referral</strong><br />
Source: NICE guidelines for suspected urological cancer<br />
In<strong>form</strong>ation given to patient:<br />
Additional Clinical In<strong>form</strong>ation: Include any investigations arranged or results obtained, and any other in<strong>form</strong>ation you<br />
think relevant.<br />
Continue on a separate sheet if necessary ensuring patient details and referring doctor’s name are on additional sheets<br />
Please ensure this <strong>form</strong> is received in the Trust within 24 hours of GP decision to refer
North West London<br />
Hospitals NHS Trust<br />
Fax: 020 8235 4188<br />
Tel: 020 8235 4293<br />
Ealing Hospital NHS<br />
Trust<br />
Fax: 020 8967 5005<br />
Tel: 020 8967 5000, x3921<br />
Imperial College Healthcare<br />
NHS Trust<br />
Charing Cross Hospital<br />
Fax: 020 8846 7564<br />
Tel: 020 8383 5000<br />
St Mary’s Hospital<br />
Fax: 020 7886 1580<br />
Tel: 020 7886 1527<br />
Hillingdon Hospital NHS Trust<br />
Fax: 01895 279890<br />
Tel: 01895 279698<br />
2WW dedicated fax line : 01895<br />
279807<br />
Chelsea and Westminster<br />
NHS Foundation Trust<br />
Fax: 020 8746 8814<br />
Tel: 020 8237 2679<br />
West Middlesex<br />
University Hospital NHS<br />
Trust<br />
Fax: 020 8321 5157<br />
Tel: 020 8321 6776<br />
Please ensure this <strong>form</strong> is received in the Trust within 24 hours of GP decision to refer