Radiology Case Presentation - Henry Ford Health System
Radiology Case Presentation - Henry Ford Health System
Radiology Case Presentation - Henry Ford Health System

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Department of <strong>Radiology</strong><br />
<strong>Henry</strong> <strong>Ford</strong> <strong>Health</strong> <strong>System</strong><br />
Detroit, Michigan<br />
<strong>Radiology</strong> <strong>Case</strong><br />
<strong>Presentation</strong><br />
Erin Canale<br />
Wayne State University, MS4<br />
April 24, 2009
History<br />
• 20 yo F c/o pain & swelling in right heel & ankle<br />
for 2 months<br />
– Insidious onset<br />
– Pain exacerbated by weight-bearing<br />
– No history of recent trauma or injury; occasional<br />
“sprains” in past secondary to gymnastics<br />
• ROS<br />
– No fever, chills, malaise, weight loss, loss of appetite<br />
– MSK: RLE – swelling, mild redness; pain with weightbearing,<br />
normal ROM<br />
– All other systems negative
Rt ankle
Rt ankle
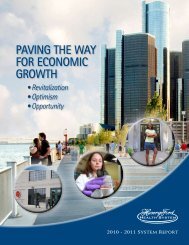
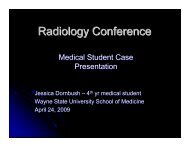
Right ankle,<br />
AP & lateral with os calcis view<br />
• FINDINGS:<br />
– lateral aspect of calcaneus is sclerotic<br />
– irregular cortical margin<br />
– calcifications in the soft tissue lateral to calcaneus<br />
• IMPRESSION:<br />
– Abnormal appearance of the calcaneus.<br />
– Possibility of tumor – location unusual<br />
– Also consider osteoid osteoma & healing stress<br />
fracture<br />
– Recommend further imaging studies
Bone Tumors: Workup<br />
• Imaging<br />
– X-ray<br />
• Best initial imaging<br />
• Suggest diagnosis & guide further work-up<br />
– CT<br />
• Bone destruction & soft tissue mass/calcification<br />
• Pathologic fractures<br />
• Helpful in flat bones – periosteal changes<br />
• Used in staging - pulmonary metastases<br />
– MRI<br />
• More sensitive than CT in local evaluation of tumor<br />
– Distribution of tumor within bone<br />
– Extent of soft tissue mass<br />
– Bone scan<br />
• Evaluate for metastases<br />
• Pathology<br />
– Biopsy<br />
• perform after baseline MRI studies
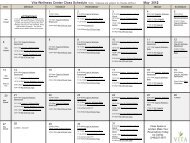
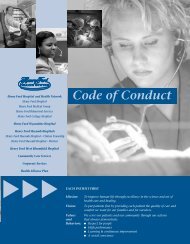
MRI, coronal
MRI, axial
MRI, sagittal
Rt ankle, MRI<br />
•FINDINGS:<br />
– Tumor extends into bone marrow<br />
– Involves soft tissue up to skin margin<br />
– Tumor enhances<br />
• IMPRESSION:<br />
– Large tumor extending into bone marrow<br />
cavity<br />
– Enhancing lesion demonstrates viable tumor<br />
tissue
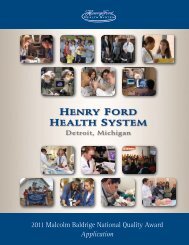
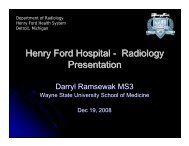
CT Rt ankle, axial
Rt ankle CT<br />
•FINDINGS:<br />
– Sclerotic lesion in the lateral calcaneus<br />
– Aggressive periosteal reaction<br />
– Associated soft tissue mass<br />
• Contains areas of enhancement & calcification<br />
• IMPRESSION:<br />
– Juxtacortical lesion in the lateral calcaneus<br />
– Most likely representing a periosteal<br />
osteosarcoma.
Bone Scan
Differential Diagnosis<br />
• Osteosarcoma<br />
• Osteoid osteoma<br />
• Chondrosarcoma<br />
• Ewing Sarcoma
Pathologic Diagnosis<br />
• Conventional osteosarcoma<br />
– Grade 2/3
Osteoid Osteoma<br />
• Small (< 1 cm) lucent<br />
lesion<br />
• Surrounded by<br />
marked reactive<br />
sclerosis<br />
• May have areas of<br />
radiodensity within<br />
the lucent lesion<br />
• M > F<br />
Source: Schwartz et al. Schwartz’s Principles of<br />
Surgery, 8th Edition: http://www.accessmedicine.com
Chondrosarcoma<br />
• Location: pelvis, ribs,<br />
scapula<br />
• Cortical destruction<br />
• Soft tissue calcification<br />
• Lobulated appearance<br />
• M > F<br />
• Age 20 – 80 (usually<br />
older patients)
Ewing’s Sarcoma<br />
• Location: diaphysis<br />
• Permeative pattern of<br />
bone lysis<br />
• Periosteal new bone<br />
formation<br />
– Onion-skinning<br />
• F > M<br />
• 10 – 20 yrs old<br />
Source: Schwartz et al. Schwartz’s Principles of Surgery, 8th<br />
Edition: http://www.accessmedicine.com
Osteosarcoma<br />
• Location: metaphysis<br />
• Mixed lytic & sclerotic lesion<br />
• Periosteal reactions common<br />
– Codman's triangle<br />
– Sunburst or hair-on-end<br />
appearance<br />
• Soft-tissue extension &<br />
calcification common<br />
• May see skip metastasis<br />
• M > F<br />
• 10 – 20 yrs old
Osteosarcoma<br />
• Location<br />
– Usually occurs in<br />
metaphysis of long<br />
bones<br />
• 42% femur<br />
• 19% tibia<br />
• 10% humerus<br />
–15% pelvis<br />
– 8% skull & jaw<br />
– 60% occur around<br />
knee (distal femur or<br />
proximal tibia)
Osteosarcoma<br />
• Malignant mesenchymal sarcoma<br />
– Tumor cells arise from primitive mesenchymal boneforming<br />
cells<br />
• Conventional osteosarcoma: 75%<br />
– Subclassification<br />
• Osteoblastic: Majority of tumor cells produce osteoid<br />
• Chrondroblastic: Majority of cells produce chondroid matrix<br />
• Fibroblastic: Spindle cells predominate; little matrix formed<br />
• Variants: 25%
Osteosarcoma<br />
• <strong>Presentation</strong><br />
– Pain, swelling around joint<br />
• Course<br />
– Relentless growth, early metastasis to lungs<br />
• Prognosis<br />
– 5-year survival rate = 15 – 20% when treated<br />
by resection of primary tumor (amputation)<br />
– 5-year survival rate = 60% with adjunctive<br />
chemotherapy following resection
References<br />
• Chen M.Y.M.; Pope T.L., Jr.; Ott D.J.:<br />
Basic <strong>Radiology</strong>. McGraw-Hill: 2004.<br />
• Doherty GM, Way LW: CURRENT<br />
Surgical Diagnosis and Treatment, 12th<br />
Edition.<br />
• Kantarjian, HM; Wolff, RA; Koller, CA: MD<br />
Anderson Manual of Medical Oncology<br />
• Schwartz et al. Schwartz’s Principles of<br />
Surgery, 8th Edition