TRAINING AND INFORMATION CAMPAIGN ON THE ... - Fokus
TRAINING AND INFORMATION CAMPAIGN ON THE ... - Fokus
TRAINING AND INFORMATION CAMPAIGN ON THE ... - Fokus

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Gambia Committee on Traditional Practices Affecting<br />
the Health of Women and Children (GAMCOTRAP)<br />
with support from FOKUS/NKTF<br />
External review of:<br />
<strong>TRAINING</strong> <strong>AND</strong> <strong>INFORMATI<strong>ON</strong></strong> <strong>CAMPAIGN</strong><br />
<strong>ON</strong> <strong>THE</strong> ERADICATI<strong>ON</strong> OF FGM,<br />
The Gambia<br />
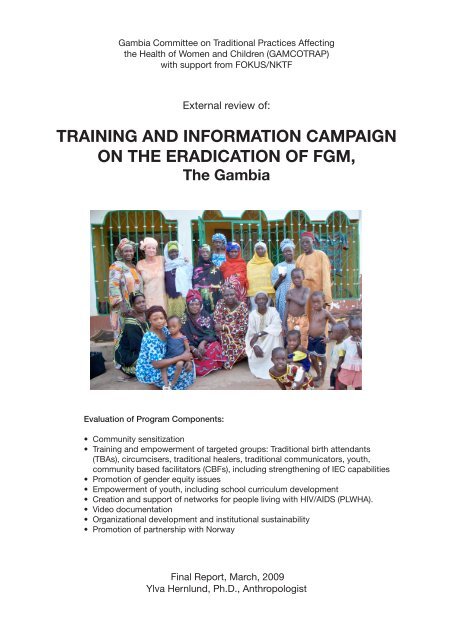
After the group meeting in Mannekunda, Basse (Amie and Ylva on the left, alkalo on far right). The elder <br />
man in white in the front row told me: “This may be a women’s affair, but it affects us men, as well. One <br />
of my wives took our daughter back to her mother’s house to be circumcised. The girl died. We didn’t <br />
use to know the bad effects.” <br />
Evaluation of Program Components:<br />
• Community sensitization<br />
Former circumciser (next to Ylva) was given seed money to start a soap business; she says people have <br />
• stopped even trying to bring girls to her to cut. <br />
Training and empowerment of targeted groups: Traditional birth attendants<br />
(TBAs), circumcisers, traditional healers, traditional communicators, youth,<br />
community based facilitators (CBFs), including strengthening of IEC capabilities<br />
• Promotion of gender equity issues<br />
• Empowerment of youth, including school curriculum development<br />
• Creation and support of networks for people living with HIV/AIDS (PLWHA).<br />
• Video documentation<br />
• Organizational development and institutional sustainability<br />
• Promotion of partnership with Norway<br />
<br />
Final Report, March, 2009<br />
Ylva Hernlund, Ph.D., Anthropologist
Table of Contents<br />
Executive Summary................................................................................................................................ 5<br />
Results........................................................................................................................................................5<br />
Conclusion and Recommendations..................................................................................................................6<br />
Background of Evaluation/Methodology.............................................................................................. 7<br />
Background to the project...................................................................................................................... 8<br />
Country Background.............................................................................................................................. 9<br />
Terminology........................................................................................................................................... 9<br />
The Practice of FGM in The Gambia................................................................................................... 9<br />
Prevalence............................................................................................................................................... 9<br />
Types........................................................................................................................................................11<br />
Background to Global anti-FGM Campaigns...................................................................................... 11<br />
Gambian anti-FGM Campaigns.......................................................................................................... 13<br />
Actors.......................................................................................................................................................13<br />
Strategies and Challenges............................................................................................................................13<br />
GAMCOTRAP.................................................................................................................................... 14<br />
Organization.............................................................................................................................................14<br />
Mission Statement......................................................................................................................................15<br />
Aims...................................................................................................................................................... 15<br />
Objectives..................................................................................................................................................15<br />
Approaches and Methods............................................................................................................................15<br />
Best Practices........................................................................................................................................ 17<br />
Results................................................................................................................................................... 19<br />
Discussion of objectives reached as proposed...................................................................................... 21<br />
General Observations..................................................................................................................................21<br />
Objectives Met as Proposed.........................................................................................................................22<br />
Unanticipated Outcomes.............................................................................................................................23<br />
Challenges and Adaptations........................................................................................................................23<br />
Monitoring and Reporting...........................................................................................................................24<br />
Cost Effectiveness.......................................................................................................................................24<br />
Partnership with Norway............................................................................................................................24<br />
Conclusions and Recommendations.................................................................................................... 25<br />
Sources Cited........................................................................................................................................ 26<br />
Appendix 1: Terms of Reference......................................................................................................... 27<br />
Appendix 2: Sources of Information Gathered in The Gambia......................................................... 31<br />
Appendix 3: Networks in which GAMCOTRAP participates............................................................. 51<br />
Appendix 4: Activities completed from Under the FOKUS funded Project from 2006 to 2008........ 52<br />
Appendix 5: Cluster Diagram.............................................................................................................. 53<br />
Appendix 6: Contributions from other donors..................................................................................... 54
Acronymes<br />
AEO<br />
AIDS<br />
CBF<br />
CBO<br />
CPA<br />
CRR<br />
FGM/C<br />
FLE<br />
FOKUS<br />
GAMCOTRAP<br />
GAMYAG<br />
HIV<br />
HTP<br />
IAC<br />
IEC<br />
IGA<br />
NGO<br />
NKTF<br />
PLWHA<br />
RH<br />
SHR<br />
SRH<br />
STI<br />
TBA<br />
TP<br />
UNCRC<br />
URR<br />
VAW<br />
VDC<br />
WR<br />
Alternative Employment Opportunity<br />
Aquired Immune Deficiency Syndrome<br />
Community Based Facilitators<br />
Community Based Organization<br />
Child Protection Alliance<br />
Central River Region<br />
Female Genital Mutilation/Cutting<br />
Family Life Education<br />
Forum for Kvinner og Utviklingsspørsmål (Forum for Women and Development)<br />
Gambia Committee on Traditional Practices Affecting the Health of Women<br />
and Children<br />
GAMCOTRAP Youth Advocacy Group<br />
Human Immunodeficiency Virus<br />
Harmful Traditional Practice<br />
Inter Africa Committee<br />
Information, Education, Communication<br />
Income Generating Activities<br />
Non Governmental Organization<br />
Norsk Kvinnelig Teologforening (Norway Women’s Theological Association)<br />
People Living with HIV and AIDS<br />
Reproductive Health<br />
Sexual and Human Rights<br />
Sexual and Reproductive Health<br />
Sexually Transmitted Infection<br />
Tradititional Birth Attendant<br />
Traditional Practice<br />
United Nations Convention on the Rights of the Child<br />
Upper River Region<br />
Violence against Women<br />
Village Development Committee<br />
Western Region
Executive Summary<br />
In The Gambia, a majority of women struggle with poverty, lack of education, and constraints on<br />
their decision-making power regarding their own reproductive and sexual health. The Gambian chapter<br />
of the Inter Africa Committee (IAC), the non-governmental organization (NGO) Gambia Committee<br />
on Traditional Practices Affecting the Health of Women and Children (GAMCOTRAP), has for over<br />
two decades been engaged in a campaign of education, sensitization, and activism aimed at eliminating<br />
harmful traditional practices, focusing in particular on abolishing Female Genital Mutilation (FGM) and<br />
early marriage, as well as promoting education and empowerment for women and girls.<br />
The main purpose of this external evaluation was to focus on the implementation and outcome of<br />
the three-year project “Training and Information Campaign on FGM,” funded by NKTF/FOKUS,<br />
Norway. This summative end-of-project evaluation seeks to provide information on the extent to which<br />
project objectives were achieved, on challenges, lessons learned from the experiences, use of resources,<br />
and organizational capacity and needs. Lessons learned about best practices are to be shared for others<br />
to replicate and, while it has been made explicit that no further funding is available from NKTF/<br />
FOKUS for the continuation of these project activities, it is hoped that the findings of the evaluation<br />
will form a basis for securing additional support for GAMCOTRAP’s ongoing efforts.<br />
The evaluation was participatory and designed in close collaboration with the funders and beneficiaries,<br />
and included document review, group meetings with beneficiaries from all the target groups in each<br />
of the project regions, as well as in-depth interviews with GAMCOTRAP staff, beneficiaries, board<br />
members, and partners.<br />
Results<br />
According to GAMCOTRAP’s reports, the information project was carried out in each of<br />
the proposed regions a total of 117 communities. The project directly reached an estimated 2,193<br />
beneficiaries. GAMCOTRAP estimates that an additional 10,965 indirect beneficiaries were reached<br />
(using a multiplier effect of 5; see Appendix 2).<br />
Representatives were trained from all the proposed target groups, which in the proposal were identified<br />
as (primary beneficiaries): women and girls, and (secondary beneficiaries): women group leaders, village<br />
heads, district chiefs, religious scholars, traditionalists, circumcisers, TBAs, traditional healers, and<br />
people living with HIV/AIDS.<br />
The broader aim of GAMCOTRAP is to sensitize communities with the ultimate goal being a<br />
reduction in FGM prevalence and increased empowerment of women and girls, while the specific focus<br />
of this project was to: train traditional birth attendants, circumcisers, and traditional healers in order<br />
to upgrade their skills and awareness regarding the harmful effects of FGM; establish networks of<br />
people living with HIV/AIDS; partner with traditional communicators and train youth drama groups;<br />
intensify Family Life Education and HIV counseling; enlist the support of traditional decision-makers;<br />
and enhance the IEC capacity of community health-providers and traditional healers.<br />
While all stakeholders realize that it is near impossible – especially in the short term – to apply<br />
objective metrics to assess actual reductions in prevalence rates of harmful traditional practices, this<br />
5
evaluation found that all the secondary sub-goals of the proposal appear to have been achieved to<br />
various degrees (at times exceeding them) and included: nine training workshops held, three videos<br />
produced, 15 drama groups trained, 16 schools reached for Family Life Education, 9 networks created<br />
for PLWHA, a Dropping of the Knives ceremony held with 18 participating former circumcisers and<br />
their communities, with an additional 60 circumcisers having declared their commitment to participate<br />
in the second such ceremony.<br />
One of the major strengths of GAMCOTRAP is its sustained efforts over time and the consistency of<br />
its approach and message. While methodology has been adapted over time (as well as from community<br />
to community, depending on need), the basic mandate has remained the same, and no effort is made<br />
to conceal the true agenda of the organization. While in the past GAMCOTRAP has often been the<br />
target of criticism, insults, and even threats, it appears that over time a major shift has taken place<br />
in public awareness and attitudes, and that the overall impression of the organization is positive.<br />
Although methodological trends in anti-FGM interventions come and go, the patient consistency of<br />
GAMCOTRAP’s approach appears to be paying off, as many beneficiaries explained that “change takes<br />
time,” but that they are now ready to consider GAMCOTRAP’s message.<br />
Conclusion and Recommendations<br />
It appears that at this time GAMCOTRAP stands at an important crossroads. After many years<br />
of sustained effort often involving extreme challenges, a shift appears to have taken place, as many<br />
Gambians are now ready to receive and consider GAMCOTRAP’s consistent message. This three-year<br />
project is seen by GAMCOTRAP staff as having been particularly crucial in effecting change, and there<br />
is a great sense of urgency in building on the current momentum.<br />
Major activities of the project have been consistent with proposed objectives, and all sub-goals have<br />
been achieved to various degrees, while important progress appears to have been made towards reaching<br />
the broader goal of gender empowerment and the abandonment of harmful traditional practices.<br />
GAMCOTRAP staff point to the need to expand geographically to areas of the country that remain<br />
unreached by campaigns and call for improved communication between various NGOs working on the<br />
issue of FGM in order to prevent overlapping in the same regions while ignoring others.<br />
Beneficiaries of the project agree with GAMCOTRAP staff that it is important to continue to focus<br />
on outreach and capacity building, while pursuing the continued commitment of traditional circumcisers<br />
to drop their knives. Community members unanimously stressed the need for consistent follow-up in the<br />
form of additional workshops, improved support for CBF’s, and expanded AEOs for former circumcisers<br />
(this was not originally proposed as part of the FOKUS funding). There is a perceived need to expand<br />
efforts with youth groups and to continue working on revising FLE curricula, as well as to strengthen<br />
and expand work with networks of PLWHA. In addition, it is crucial to continue the outreach efforts<br />
of improving IEC capacity of traditional health practitioners and to expand the important dialogue<br />
currently underway between Gambian emigrants (particularly in Spain and Norway) and their home<br />
communities.<br />
This evaluation recommends that GAMCOTRAP continue its community outreach while striving<br />
to strengthen its administrative capacity, particularly in the area of reporting, auditing, and effective<br />
communication with donors. This evaluation strongly urges for more sustained support from funders,<br />
while calling for improved dialogue between GAMCOTRAP and their supporters, as well as continued<br />
efforts to improve communication among Gambian organizations working on similar issues.<br />
6
Background of Evaluation/Methodology<br />
FOKUS/NKTF contacted Ylva Hernlund in 2008 to conduct an external, summative evaluation<br />
of GAMCOTRAP’s three-year project on education against FGM. The evaluator had previously<br />
encountered the organization during her year-long dissertation research in 1997-98. Its staff welcomed<br />
her with open arms in 1996, continuing to include her in their activities throughout the research, allowing<br />
access to a diverse range of research angles: archives in the GAMCOTRAP office library; individual<br />
interviews with staff and board members focusing on their personal histories of arriving at an anti-FGM<br />
position; observation of staff meetings (including budget discussions and planning sessions); preparations<br />
for workshops and campaign events; symposia and press conferences; and youth outreach activities.<br />
GAMCOTRAP staff invited her to travel with them on “trek” to rural areas, at one point even asking<br />
her to assist in leading small group projects by students carrying out Rapid Rural Assessment exercises.<br />
Through these travels she not only got to see firsthand how educational workshops are conducted, but<br />
also enjoyed the informal camaraderie of a group of women always enthusiastic about debating issues<br />
and reminiscing about their rich histories as gender activists.<br />
This report, although primarily based on a field visit in December 2008 and a dissemination exercise in<br />
February 2009, therefore also draws on this previous experience observing the work of GAMCOTRAP,<br />
and reflects comparisons drawn between the climate for such interventions in 1997-1998 versus today.<br />
In discussions with Amie Bojang-Sissoho and Dr. Isatou Touray, the reflection emerged that this time<br />
period in the late 90s, in retrospect, may have marked the most difficult moment of such campaigns; and<br />
this evaluation reflects the observation that a great deal of change has taken place over the last decade<br />
regarding public attitudes to and responses to GAMCOTRAP’s work.<br />
Data were gathered in The Gambia in December 2008 through interviews with GAMCOTRAP staff,<br />
volunteers, and Board members; archival research of reports and campaign materials including videos;<br />
interviews and group meetings with beneficiaries from all the targeted groups in a number of communities<br />
(26 total) in each of the regions included in the project; interviews with representatives from other NGOs<br />
involved in anti-FGM work as well as GAMCOTRAP partner organizations (the evaluator used an<br />
independent translator). In addition an electronic survey was conducted with five stakeholders in Norway.<br />
As the field visit was very brief, it was not possible for the evaluator to directly confirm the numbers<br />
of communities and beneficiaries reached; and this draft report additionally uses information from the<br />
nine project reports which were submitted to FOKUS/NKTF throughout the duration of the project,<br />
as well as a Data on Activities-file submitted by GAMCOTRAP staff to the evaluator at the conclusion<br />
of the data gathering.<br />
In February, 2009, a three-day workshop was held in The Gambia, attended by GAMCOTRAP<br />
staff, the evaluator, and Mette Bråthen Njie and Hanne Slåtten from NKTF (unfortunately the FOKUS<br />
representative was at the last minute unable to attend, due to illness). This meeting involved further<br />
document review, discussions about the experience of the partnership between Norway and The<br />
Gambia, an assessment of administrative and reporting procedures, and a thorough team-review of the<br />
first draft of this report, during which all stakeholders were given an opportunity to add comments and<br />
information and suggest further revisions to be included in the final report.<br />
In addition, a partner meeting was held on February 25 at the TANGO office in Kombo (see<br />
Appendix 2 for a list of attendees). Although the written draft report was not distributed, its major<br />
7
findings were discussed, along with presentations by NKTF, GAMCOTRAP staff, and the President<br />
of the Board; and there was a screening of one of GAMCOTRAP’s videos. The remainder of the day<br />
was spent on a group discussion during which beneficiaries spoke about their experiences with the TV<br />
project, and the NKTF representatives were able to ask follow-up questions (the evaluator was also able<br />
to interview TANGO’s Director, who had not been available during the December visit).<br />
Note: While the production of this report has been a truly collaborative effort, the evaluator naturally takes responsibility<br />
for any errors or shortcomings.<br />
Background to the project<br />
The Feminist Action Group from the 1980s pioneered work on information campaigns regarding<br />
FGM in hospitals, churches, and civil society in Norway. Anne Berit Stensaker (1930 - 2003), who was a<br />
priest and member of the Norwegian Female Theologian Committee, Norsk Kvinnelig Teologforening<br />
(NKTF), was engaged in work against female genital mutilation (FGM) from 1980. This commitment led<br />
to a lot of information about both the work and the team, but this information was never systematized.<br />
In 2004, some members of NKTF were involved in archiving this material. This work led to a contact<br />
with Mette Bråthen Njie, who had received a scholarship to work on the theme of FGM. She is a trained<br />
nurse with close relations to The Gambia, and had visited and brought back information about some<br />
of GAMCOTRAP’s work and methods. After meeting with Mary Small at GAMCOTRAP, she was<br />
impressed by the way they worked, but saw the lack of resources. NKTF also learned more through<br />
meeting with Torild Skard, feminist and former UNICEF Regional Director for West Africa (1994-<br />
1998), who knew of GAMCOTRAP’s work.<br />
After further visits to The Gambia, NKTF in 2005 decided to apply for funding from a project<br />
supported by the TV Action Campaign (through Norwegian TV) on ”Violence against Women,”<br />
where one of the sub-topics was FGM (along with Women in Conflicts, Trafficking, and Violence in<br />
Close Relationships). The TV project was that year dedicated to FOKUS (Forum for Women and<br />
Development), where one NKTF member had previously worked.<br />
Also in 2005, Dr. Isatou Touray was invited by FOKUS through NKTF, coordinated by Mildrid<br />
Mikkelsen, to attend a TV-Campaign meeting in Norway. FOKUS previously knew about her work<br />
through the Inter Africa Committee (IAC) and other NGOs. This visit made it possible for GAMCOTRAP<br />
to present its work to the donor community in Norway with the hope of gaining support for its work<br />
to eliminate FGM in The Gambia. It also created an opportunity for GAMCOTRAP to meet with its<br />
partner organization, NKTF, to get to know each other and discuss the proposal to end FGM, which was<br />
submitted to FOKUS. The Norwegian team consists of five women: Tone Marie Falch, Hanne Slåtten,<br />
Yvonne Anderson, Caroline Revling Erichsen, and Mette Bråthen Njie. During the visit, Isatou Touray<br />
presented the proposal to the team of women and it was discussed intensively and agreed upon.<br />
Dr. Touray was made to understand from this visit and the meetings held between FOKUS/NKTF<br />
and GAMCOTRAP that FOKUS gives support to countries by pairing local Norwegian organizations<br />
with other existing NGOs abroad. The partnership was mutual and accepted by both NKTF and<br />
GAMCOTRAP because their vision, mission, and objective resonate with each other. Having agreed to<br />
work together, GAMCOTRAP’s proposal was accepted and NKTF was made responsible for facilitating<br />
the project with support from FOKUS (FOKUS has no direct co-operation with GAMCOTRAP,<br />
8
ut supports the project co-operation that takes place through FOKUS between its member organizations<br />
and their local partner organizations). To that effect, a project agreement was made between NKTF and<br />
GAMCOTRAP with FOKUS funding to ensure the realization of the project, which operated from<br />
2006 – 2008.<br />
Country Background<br />
The Gambia is one of the poorest countries in the world, dependent from the moment of its<br />
independence to rely on foreign assistance for its survival. The population growth rate (1990-2006)<br />
is estimated at 3.4% per year, infant mortality rate (under 1) at 84 per 100,000 live births, maternal<br />
mortality 730; life expectancy at birth 59 years (UNICEF 2009). The overall literacy for women is<br />
26.9%, 55% for males (Government of The Gambia 1993; more recent UNICEF study does not provide<br />
these numbers). School enrollment is (2000-2006) 79% for males and 84% for females at the primary<br />
level, with 51% males and 42% females at the secondary level (UNICEF 2009). Agriculture provides<br />
60% of productive employment (Government of The Gambia 1993; more recent UNICEF study does<br />
not provide these numbers). There is also a limited impact of tourism, fisheries, “re-export” trade, light<br />
industries, and products from livestock. Continual economic decline has hit women especially hard.<br />
Many Gambians, especially young and middle-aged men, see the only way “out” as a literal escape to<br />
labor markets in the Global North, thus creating a massive movement out of the country with femaleheaded<br />
households left behind.<br />
Terminology<br />
While other terminology is used in other contexts (such as “female circumcision,” “female genital<br />
cutting,” FGC, or FGM/C), the preferred terminology of GAMCOTRAP is Female Genital Mutilation<br />
(FGM), which will be used throughout this report.<br />
The Practice of FGM in The Gambia<br />
Prevalence<br />
All existing studies agree that female genital mutilation is practiced by a substantial majority of<br />
Gambians. Earlier local studies report that 79% (Singateh 1985) to 83% 1 of all Gambian women have<br />
undergone some form of genital mutilation, while others use the Hosken report’s estimate of 60%<br />
(Touray 1993). A Gambian government study (Daffeh et al. 1999) puts the prevalence rate at 80%<br />
overall. More recently, the MICS (Multiple Indicator Cluster Survey) study for UNICEF, “Monitoring<br />
1. Estimated by a 1991 KAP (Knowledge-Attitude-Practice) study, carried out by the Monitoring and Evaluation Unit of<br />
the Women’s Bureau as part of the “Safe Motherhood” component of a Women in Development Project Report.<br />
9
the Situation of Women and Children” estimates that of all women aged 15-49, 78% have undergone<br />
FGM, while 64% of mothers in the same age-group have at least one daughter who has undergone the<br />
practice (UNICEF 2009), seemingly indicating a reduction in prevalence.<br />
These numbers, however, hide the complexity of who in The Gambia is actually practicing FGM and<br />
why. Daffeh et al. caution that previous literature on FGM in The Gambia has displayed “a gap between<br />
theory and practice, with regard to ethnicity” (Daffeh 1999). Daffeh et al. go on to assert that in the Gambian<br />
case, the “ethnic classifications with regard to FGM are much more complex than was hitherto apparent”<br />
(ibid). They are referring to general statements, such as “Wollofs don’t practice female circumcision,”<br />
which various Gambians commonly repeat without qualification. When Wollof girls do undergo FGM, it<br />
has usually been explained as due entirely to pressure from individuals of other ethnic backgrounds that<br />
causes co-wives or schoolmates to “join” their peers in circumcision. It appears, however, that the rate of<br />
circumcision for girls who identify as Wolof (but could have multi-ethnic heritage) is actually quite high.<br />
The Daffeh report presents more nuanced data on ethnicity, focusing on the variation in circumcision<br />
according to ethnic sub-group and ancestral geographic origin. Thus, they argue, for certain sub-groups of<br />
Wollofs FGM is as strong a tradition as it is for Mandinkas and Serahules, among whom the practice is said<br />
to be virtually universal. A total of 96% of Jolas circumcise females, again with variation across sub-goups<br />
(ibid). The authors of the 1999 report conclude that the only ethnic groups in The Gambia that do not at<br />
all practice FGM are the Creoles, the Lebanese, and the Manjagos (ibid).<br />
Although these numbers do throw light on a previously poorly understood area, ethnic and even<br />
sub-ethnic labels are not entirely reliable as indicators of whether a girl will undergo FGM or not. It is<br />
important to note that marriage across ethnic lines is very common and relatively unproblematic in The<br />
Gambia, and that it is typical to encounter Gambians whose relatives come from two or more ethnic<br />
groups. The age at which girls are circumcised is also somewhat tied to ethnicity, although not in any<br />
simple way. Serahule communities generally practice FGM in the first week of the girl’s life, coinciding<br />
with her naming ceremony. In other ethnic communities, the age of circumcision may vary widely.<br />
When initiations take place in a communal context, a group of girls may include infants, young children,<br />
and even teenagers, depending on how long the ritual cycle is until another big celebration rolls around.<br />
In general, however, there is clearly a trend in The Gambia, as elsewhere in Africa, to “circumcise” girls<br />
at a younger and younger age.<br />
Additionally, geographic location impacts prevalence rates. Project reports from The Gambia typically<br />
refer to urban versus rural areas, but it can be a bit difficult to define the two (according to the 2009<br />
UNICEF study, 72% of urban women have undergone FGM, 83% of rural). The Gambia has no true<br />
cities – the capital of Banjul is a sleepy town of a mere 50,000 or so. Most population growth is taking<br />
place in the nearby peri-urban areas of Bakau and Serrekunda – sprawling, densely populated towns<br />
predominantly populated by rural migrants. The 1993 Gambian census bases its definition of “urban”<br />
on: commercial and institutional importance, majority of population engaged in non-agricultural work, a<br />
population of 5,000 or more, high population density, and the presence of some infrastructure. In terms<br />
of FGM, however, prevalence rates in The Gambia do not correspond to facile assumptions of rural<br />
“traditionalism” and urban “progressiveness.” As evidenced in GAMCOTRAP’s reports on its campaign<br />
activities, community abandonment of harmful traditional practices can often be found clustered in very<br />
remote rural areas otherwise considered “traditional,” while the practice remains entrenched in “urban”<br />
centers such as Bakau and Brikama. Additionally, there is – despite the very small size of the country – a<br />
great deal of regional variation in the reach of anti-FGM interventions. Despite past attempts to coordinate<br />
the efforts of various NGOs involved in anti-FGM education and activism, in reality certain regions (such<br />
as the Basse area in URR) have been targeted by sensitization efforts of several different groups, while<br />
other areas (in particular on the North Bank) remain essentially unreached.<br />
10
Types<br />
WHO classifies FGM into the following types:<br />
I. Clitoridectomy (removal of part or all of the clitoris)<br />
II. Excision (removal of the clitoris and all or part of the labia majora)<br />
III. Infibulation (removal of and suturing together of the external genitalia)<br />
IV. Unclassified.<br />
For The Gambia, reports on the most common procedure vary (more recent WHO and UNICEF<br />
studies do not report types for The Gambia). According to one study, a majority of women (44.3%) had<br />
undergone Type II, with 21.4 Type I (Singateh 1985). Another one estimates 56% as having undergone<br />
Type I, 19% Type II (Daffeh et al. 1999). Both studies agree that 6-7% of Gambian women have<br />
undergone “sealing” (notoro), a non-suturing form of infibulation which falls under Type IV, but is unique<br />
to The Gambia (recent research with circumcisers by GAMCOTRAP suggests that this rate may be<br />
higher, but these data have not yet been analyzed). This practice is thought to be particularly prevalent in<br />
areas of the eastern part of the country, as was indeed evidenced by the frequency with which discussions<br />
about the health effects of sealing came up in the evaluation field visits to the Upper River Region.<br />
Background to Global anti-FGM Campaigns<br />
Identifying the most effective and appropriate methods for eliminating FGM is among the most<br />
contested issues surrounding the practice. Early colonial interventions alternately employed strategies<br />
based on the alleged adverse health effects of the practice and discourses framing the practice as<br />
uncivilized, barbaric, and unacceptable in the eyes of Christianity. Such campaigns have reappeared<br />
several times throughout the last century, each time with a slightly different focus. In the 1970s and 80s<br />
the practice was identified as “genital mutilation” and became targeted for “eradication” as a public<br />
health problem (see Hosken 1978). Some, particularly in the West, approached the practice as a human<br />
rights violation, often using extreme rhetoric which has caused a bitterness to still linger over the debates<br />
surrounding the practice and its elimination. Although often offended by the sensationalist manner in<br />
which the issue was discussed by outsiders, many African women have over time invited assistance from<br />
Western donors, and current efforts are largely supported by outside funding being channeled through<br />
indigenous women’s organizations.<br />
A series of conferences and international meetings have been held to address strategies for eliminating<br />
FGM, starting with the 1979 Khartoum seminar on Traditional Practices Affecting the Health of Women<br />
and Children. After an initial reluctance to address the issue, the World Health Organization organized<br />
a meeting at which representatives from a number of African countries began identifying strategies for<br />
eliminating the practice. In the late 1980s, WHO issued an elaborate plan for action, and other major<br />
agencies have since joined the global campaign with their own platforms.<br />
There are several, not mutually exclusive, ways in which to approach anti-FGM campaigns: as a<br />
human rights’ violation, as an infringement of the rights of the child, the right to sexual and bodily<br />
integrity, and/or as to the right to health. Many of those who organize against genital mutilation do so<br />
based on a broader concern for the human rights of women and children, while others also express a<br />
11
concern for women’s sexuality. A number of scholars and activists, however, have concluded that the<br />
most “sensitive” and least controversial angle from which to argue for the elimination of the practice is<br />
that of the right to health and bodily integrity.<br />
A number of African nations have passed legislation against FGM, although enforcement mechanisms<br />
vary. Many feel, however, that outright legislation against the practice, especially during the early stages<br />
of abandonment, is highly problematic as it pits community members against each other, penalizing<br />
individuals acting in good faith within their cultural framework, and potentially driving the practice<br />
underground and reducing the likelihood that those who need medical attention will receive it.<br />
The “development and modernization” approach suggests that overall improvements in socioeconomic<br />
status and education, especially for women, will have far-reaching social effects, including a reduced<br />
demand for FGM. The empirical data do not consistently support this conclusion, however, and many<br />
argue that changing social conditions will not automatically change strongly held beliefs and values<br />
regarding female “circumcision,” but that targeted intervention issues on the harmful effects of the<br />
practice are needed as well.<br />
The “convention theory” of abandonment argues that practices such as FGM are conventions locked<br />
in place by interdependent expectations in the marriage market and that once in place such conventions<br />
become deeply entrenched, since those who fail to comply also risk failing to reproduce (Mackie 2000).<br />
Therefore, education about adverse consequences does not suffice, but must be accompanied by a<br />
collective convention shift. This approach, which has been carried out in practice by the Senegalese<br />
NGO Tostan, uses basic education leading to public declarations in which communities who historically<br />
intermarry join in denouncing FGM.<br />
It is common for activists to argue that one of the reasons that FGM is so “entrenched” is that it<br />
constitutes an important source of income for those performing the procedure. Consequently, some<br />
eradication efforts have focused in part on schemes to compensate circumcisers for lost income. Critics<br />
(see Mackie 2000) argue that this is a misguided functionalism: although circumcisers immediately do<br />
cause circumcision of girls, they do not cause parents to want circumcision for their daughters and<br />
thus do not directly cause the continuation of the practice. Others point out that circumcisers may<br />
receive compensation for not practicing while continuing to do so in secrecy. However, in contexts in<br />
which circumcisers are prestigious community leaders, their genuine conversion is crucial and it may<br />
be an important strategy to provide at least symbolic, and perhaps limited material, support to those<br />
circumcisers who have already had a change of heart, thus motivating them to stick to their decision,<br />
which is distinct from “bribing” people to stop.<br />
Some groups and communities have experimented with alternative, non-circumcising rituals, for<br />
example in Kenya and The Gambia. The success of such an approach has not been documented,<br />
however, and there are reports from Kenya that girls who have undergone “ritual without cutting” have<br />
later been coerced into actual genital cutting.<br />
While these approaches have been discussed separately, in reality most campaigns combine a variety<br />
of strategies into an integrated approach.<br />
12
Gambian anti-FGM Campaigns<br />
Actors<br />
The Gambian campaign can be traced back to the early 1980’s when a small group of women,<br />
most of who are to this day involved in work against FGM, began an organized effort to abolish genital<br />
cutting. It started through the Women’s Bureau, which represented The Gambia at a general meeting<br />
in Dakar of the Inter Africa Committee (IAC) in February of 1984. Due to the perceived need to<br />
address FGM separately from the broader goals of the Women’s Bureau, the Gambia Committee of the<br />
IAC was then created and, in 1992, its name was changed to GAMCOTRAP (Gambia Committee on<br />
Traditional Practices Affecting Women and Children).<br />
In the early 1990’s the splinter group BAFROW (Foundation for Research on Women’s Health,<br />
Development and the Environment) was established, and GAMCOTRAP moved to its present location.<br />
By the late 1990s a newer group, APGWA (Association for Promoting Girls’ and Women’s Advancement<br />
in The Gambia), focused on alternative non-cutting ritual. In later years, a number of other organizations<br />
have in various ways been involved in anti-FGM work.<br />
Strategies and Challenges<br />
Those involved in efforts to abolish FGM have through the findings of several research studies<br />
been able to design more appropriate strategies. It has been found, for example, that in the Gambian<br />
context there is a great need to address the widespread but unfounded belief that female “circumcision”<br />
is a religious injunction in Islam. In her 1993 report, Isatou Touray argues that the practice can<br />
only be approached as a health issue after or simultaneously with approaching it from a sociocultural<br />
and religious angle. The vast majority of Gambians are Muslims (90%+) and FGM is often seen as<br />
somehow associated with Islamic identity. Activists stress, however, that the Qu’ran does not require<br />
female “circumcision,” that not all Islamic groups practice FGM, and that many non-Islamic ones<br />
do. In contexts in which Islam is to various degrees invoked as associated with the continuance of the<br />
practice it is often the focus of intense local theological debates, and a great deal of effort by scholars<br />
and activists has concentrated on demonstrating the lack of scriptural support for enforcing FGM,<br />
as is particularly evident in GAMCOTRAP’s close collaborations over time with religious leaders.<br />
In addition, this debate has benefitted from the recent Rabat Declaration (2007), in which Islamic<br />
scholars from many nations openly opposed FGM. The evaluation confirmed that many Gambians<br />
bring up the issue of religion and have come to see the practice of FGM as separate from religious<br />
requirements.<br />
Currently a number of African countries, including neighboring Senegal, have passed laws against<br />
FGM, while The Gambia has not done so. Interviewees pointed to the difficulties that ensued when<br />
the law was passed in Senegal and there was an increase in demand for cross-border circumcision<br />
in The Gambia – a situation that is still encountered by some circumcisers in URR who live close to<br />
the Casamance border. Although far from all respondents expressed support for national anti-FGM<br />
legislation as a strategy at the present time, GAMCOTRAP has through the duration of the FOKUS<br />
project identified increasing calls from communities for such legislation, which the organization now<br />
supports.<br />
13
In the absence of anti-FGM legislation, up to the present, attempts have been made to bring charges<br />
under existing assault laws when girls have been circumcised against their wishes and those of their<br />
families, so far unsuccessfully. GAMCOTRAP submitted a draft of areas for inclusion in law reform on<br />
women’s rights, including FGM, in 2008, after a request by the Law Reform Commission, and became<br />
involved as advocates in the Awa Nget case (Asemota, 2002a, 2002b) with the help of funds raised<br />
through the Urgent Action Fund through Equality Now’s Africa Region.<br />
Anti-FGM work has at times been considered highly controversial in The Gambia. In 1997, the thennewly<br />
elected Gambian government issued a decree which banned the broadcasting on state radio and<br />
TV (the only TV station in the country was controlled by the government) of any programs “which either<br />
seemingly oppose female genital mutilation or tend to portray medical hazards about the practice.” This<br />
information came to the public in 1997 when Dr. Isatou Touray was conducting a gender class for media<br />
practitioners and issues of traditional practices were discussed in order to create awareness amongst<br />
media practitioners.<br />
It was during this class that a media directive dated 17 th May 1997 banning any form of advocacy<br />
against female genital mutilation on national radio or television was accessed. GAMCOTRAP responded<br />
to the directive by making a clarion call to the President of the Republic in an open letter dated 27 th<br />
May 1997. After massive protests – from in particular GAMCOTRAP, aided by an international letterwriting<br />
campaign organized by New York-based Equality Now – the decree was lifted, although with so<br />
little publicity that many people are still unclear on what is and is not legal to broadcast.<br />
Vice President Isatou Njie-Saidy, herself a women’s rights activist who has previously been involved in<br />
the campaign against FGM, was later quoted as stating that the government’s policy will be to “discourage<br />
such harmful practices,” and that NGOs will not be prevented from working against the practice (Forward<br />
with The Gambia newsletter July 7, 1997). Head of State President Colonel (Retired) Yaya Jammeh, in his<br />
annual address marking the 1994 July 22 military take-over, clarified the government’s position as being<br />
opposed to FGM, but stressed that any campaign must be conducted in a culturally sensitive manner.<br />
Yet, later he issued a statement that activists “cannot be guaranteed that after delivering their speeches,<br />
they will return to their homes” (Observer newspaper, January 25, 1999).<br />
GAMCOTRAP<br />
Organization<br />
GAMCOTRAP was established in 1984 as the Gambian chapter of the Inter Africa Committee.<br />
It is an NGO, with non-profit status, registered with the NGO Affairs Agency and The Association<br />
for Non-Governmental Organizations (TANGO), an umbrella organization that registers, monitors,<br />
and supports Gambian NGOs . GAMCOTRAP has a General Assembly, Board of Directors, and<br />
Executive Committee. The General Assembly is the supreme organ of GAMCOTRAP and is composed<br />
of the representatives of communities and all other affiliates. The elected Board of Directors includes<br />
a President, Vice President, and Treasurer, as well as other individuals with varied expertise relevant<br />
to GAMCOTRAP’s work. Like all NGOs registered by TANGO, GAMCOTRAP has a Constitution,<br />
Action Plan, and Guiding Principles, and has been registered under the Company Act as a Charity with<br />
the Attorney General’s Chambers.<br />
14
GAMCOTRAP collaborates with the Women’s Bureau, which advises the government on all policy<br />
matters affecting Gambian women. In addition, GAMCOTRAP participates in an ongoing manner in<br />
a number of networks on the international, national, and grassroots level (see Appendix 3).<br />
Mission Statement<br />
“GAMCOTRAP’s mission is to create awareness about traditional practices in The Gambia. We aim<br />
for the preservation of beneficial practices (such as breastfeeding) as well as the elimination of harmful<br />
traditional practices.<br />
GAMCOTRAP is committed to the promotion and protection of women and girl children’s political,<br />
social, educational, and sexual and reproductive health rights.<br />
We support any national and international declarations protecting these rights, in particular the<br />
Convention on the Elimination of All Forms of Discrimination against Women, The Convention on the<br />
Rights of the Child, and the Protocol of the African Charter on Human and People’s Rights and on the<br />
Rights of Women.”<br />
Aims<br />
“To create and raise the consciousness of men and women about traditional practices that negatively<br />
affect the health of children and women, whilst encouraging positive practices. In addition, we aim to<br />
protect the rights of children and women by involving them to participate in decision-making processes.”<br />
Objectives<br />
1. To carry out research into traditional practices that affect the sexual and reproductive health<br />
of women and girl children in The Gambia.<br />
2. To identify and promote traditional practices that improve the status of girl-children and women.<br />
3. To create awareness of the effects of harmful traditional practices on the health of girlchildren<br />
and women, in particular FGM, nutritional taboos, child/early marriage, and wife<br />
inheritance.<br />
4. To promote and encourage the education of girls at all levels.<br />
5. To sensitize and lobby decision- and policy-makers about sociocultural practices that are<br />
harmful to the health of girl-children and women.<br />
6. To promote and protect the human rights of girl-children and women.<br />
7. To create awareness of international and national instruments that address discrimination<br />
and violence against girl-children and women.<br />
8. To influence policies in promoting and protecting women’s and children’s rights.<br />
9. To highlight a rights-based approach to activities.<br />
10. To solicit funds locally and externally for the purpose of carrying out the above objectives.<br />
Approaches and Methods<br />
GAMCOTRAP believes that the elimination of harmful traditional practices has to be approached<br />
through research, training, and advocacy. It employs a multi-pronged approach that seeks to match the<br />
15
appropriate strategy to specific community characteristics, with its work consisting primarily of carrying<br />
out educational and “sensitization” campaigns, as well as lobbying. Its staff members visit schools<br />
(including organizing essay and poster competitions), hold press conferences and symposia, produce<br />
videos, and organize workshop for health workers, traditional healers, TBAs, circumcisers, and youth.<br />
GAMCOTRAP has remained adamantly opposed to alternative rituals, and subscribes to a philosophy<br />
of ultimate total abandonment of FGM, “zero tolerance” and advocates for the passing of national anti-<br />
FGM legislation. Recently the organization has intensified its efforts to build dialogue with emigrant<br />
Gambians in the diaspora, spreading awareness of the legal consequences of sending foreign-born girls<br />
“home” for “holiday circumcisions.”<br />
GAMCOTRAP sees the main factors influencing the practice of FGM in The Gambia as being:<br />
1. Sociocultural.<br />
2. Religious<br />
3. Other factors (including ignorance/poverty of practitioners).<br />
Its methods, therefore, are grounded in varied approaches, including: awareness-raising, grassrootssensitization<br />
regarding HTPs, collaboration with respected religious leaders able to address scriptural<br />
issues, community education about the harmful effects of FGM, and support for circumcisers committed<br />
to ending the practice.<br />
Training workshops are organized by first dividing participants by village, then into groups (such<br />
as young or old women or men, TBAs, circumcisers, traditional healers), then having all participants<br />
come together into a “plenary” discussion. This way, “everyone has to face everyone.” This is especially<br />
important when men and women each claim that it is the other group that requires that FGM be<br />
practiced. Participants are asked to first list the traditional practices they are aware of in their community<br />
and later to rank them as “positive,” “negative” or under “lack of consensus.”<br />
An important component of awareness-raising is the use of visual aids, including anatomical<br />
models and a slide show that presents adverse health effects of genital cutting, but GAMCOTRAP<br />
hopes to develop its own materials based on Gambian cases). While some activists from other groups<br />
expressed disagreement with the method of “shocking” trainees with graphic images of health effects,<br />
GAMCOTRAP staff sees this “awakening” as central to the process of attitude change (and point out<br />
that the goal is not to “shock,” although this is sometimes the effect). The evaluation, as well, found that<br />
most beneficiaries, when asked what had most affected their attitudes to FGM, responded that they<br />
had become aware of the adverse health consequences. When probed to explain more about what<br />
specifically affected their change in attitudes, a majority of beneficiaries interviewed mentioned the<br />
visual aids and pointed out that “health is the most important thing for human beings.” They stressed<br />
that “seeing is believing” and that although many of them had previously been told that FGM is harmful,<br />
they did not believe this to be true until they saw the photos of actual women and girls suffering adverse<br />
consequences (such as retention of urine and/or menstrual blood, and severe keloid scarring). This led<br />
to realizations that the beneficiary herself and/or someone close to her had also suffered these health<br />
effects, while perhaps having attributed them to other causes.<br />
GAMCOTRAP activists argue that there is little resistance to showing these visual materials to groups,<br />
including those of mixed age and gender, although they always preface such viewings with a warning<br />
and make it clear that anyone is free to leave (which religious elders occasionally do), and the images are<br />
only presented at the end of the training session when group discussion and general sensitization have<br />
already been concluded. The evaluator was struck by the nearly universal mention by respondents that<br />
16
it was the images that had made them see the truth in the anti-FGM message. In addition, videos are<br />
shown during the training workshops to reinforce the message on the harmful effects of FGM, as well as<br />
the spread awareness of HIV/AIDS.<br />
GAMCOTRAP tailors its educational approach to the target group and each community’s discussions<br />
take on their own character according to local needs and concerns. When a major tumbling block during a<br />
community discussion appears to be religion, clarification is provided by a resource person. In workshops<br />
with traditional healers, information on HIV transmission is disseminated as these practitioners are<br />
often the first point of contact and need training in how to recognize signs and encourage patients to<br />
seek testing. Traditional birth attendants ask for kits and more training and are encouraged to use ICE<br />
on FGM after the birth of any girl. In the Wuli workshop there was a discussion on the definition of<br />
“early” marriage and what sharia has to say about a girl’s preferred age at marriage.<br />
In several communities, women expressed their fear to seek family planning for fear of being accused<br />
of infidelity, while men said they approved of married women spacing births but would not agree to<br />
contraceptives being made available to unmarried young women. In Foni, there was an expressed<br />
concern with domestic violence, which women stated is often justified by religion, which was refuted by<br />
a religious scholar, who argued that men and women need to be partners in marriage.<br />
Youth were engaged in discussions on reproductive health, and health threats such as poverty, drugs,<br />
alcohol, and early pregnancy. Brochures were handed out, as were condoms, and they were encouraged<br />
to, anonymously put their questions about sex in a box, the “Secret Clinic,” to be answered in front<br />
of the group. Youth asked for drama groups, video, and sometimes made statements such as that they<br />
will burn the jujuyo (traditional circumcision hut), conduct Peace Marches, and report the names of<br />
any circumcisers still practicing (GAMCOTRAP clarified that they will only sensitize, not bring legal<br />
action).<br />
One particularly crucial target group consists of the ngangsingbas, traditional circumcisers. As opposed<br />
to elsewhere in Africa, FGM is never performed by male practitioners or by female health professionals.<br />
GAMCOTRAP has taken particular care to reach these women, who retain their important role in<br />
society after abandoning the practice. Eighteen former circumcisers participated in the Dropping the<br />
Knife celebration of May, 2007 (see Results), and GAMCOTRAP states that currently more than sixty<br />
others are committed to abandoning the practice and participate in the next Dropping of the Knife.<br />
Best Practices<br />
GAMCOTRAP’s self-assessment identifies its major strength as lying in its staff of committed<br />
activists. Dr. Touray and Ms. Bojang-Sissoho are both circumcised Mandinka women with a deep<br />
understanding of both the cultural and religious context and Gambian political realities. While acutely<br />
attuned to the need to follow local etiquette, they are resilient and courageous, and consistently display<br />
remarkable flexibility and insight (as well as compassion and humor) when dealing with often rapidly<br />
changing circumstances in the field. They are extremely well-versed in not only international human<br />
rights protocols but also Islamic theology, and can engage in culturally and religiously sensitive dialogue<br />
with a wide range of individuals and groups, always ”taking the pulse” of which approach is most<br />
appropriate with a particular person or community. This ability is something that can not be learned<br />
through formal training, but can only be found in a true ”insider.” Additionally, they are both extremely<br />
17
effective public speakers with fluency in several local languages. The TV-project has been especilly<br />
instrumental in freeing up Dr. Touray to work full-time on coordinating the project.<br />
GAMCOTRAP does not employ an approach of stressing charismatic personalities. Although both<br />
Amie and Isatou are indeed well known and respected in the communities in which they work (and their<br />
names at times show up in praise-songs) they stress that ”GAMCOTRAP is not Amie or Isatou.” The<br />
groundwork that they have done over so many years could be continued by other dedicated activists,<br />
and there is evidence of training of junior staff and volunteers and the transfer of competency, as was<br />
particularly demonstrated by the active participation in the dissemination exercise of Musa Jallow and<br />
Omar Dibbah. This philosophy was also evident during the field visit (as was also the case during the<br />
evaluator’s travels with the group in 1997-98) – GAMCOTRAP staff behave in an extremely humble<br />
way when ”on trek.” They use very modest accomodations, eat simple food, and work long hours without<br />
ever complaining about discomfort or fatigue. GAMCOTRAP staff meet community members on their<br />
own terms, joining them in their work and domestic responsibilities. They are acutely aware of farming<br />
cycles and women’s domestic labor burdens and make a genuine and concerted effort to empathize with<br />
the realities of the people they are trying to reach. GAMCOTRAP also has a firm policy of not handing<br />
out cash to praise-singers, kanyelengs, and others. Instead, they budget for a collective contribution to be<br />
given at the end of the visit to a designated group of women.<br />
GAMCOTRAP are veterans in the field of anti-FGM activism and are anchored in long-term<br />
relationships with the communities they serve, and their approach is characterized by frankness and<br />
transparency. While remaining attuned to the need to show respect (especially for elders, dignitaries, and<br />
individuals with particular prestige) the activists never conceal their agenda nor make excuses for their<br />
convictions. Because there has been no attempt throughout the sustained campaign to veil the message<br />
or hide it within other agendas, GAMCOTRAP appears to have ultimately gained the respect of the<br />
populations they have worked so long to sensitize.<br />
While never straying from the agenda that was set out at the inception of the Gambian IAC chapter,<br />
it is evident that GAMCOTRAP staff display flexibility and adaptability in tailoring their message to<br />
specific community realities and are open to making adjustements in campaign approaches over time.<br />
Thus, there has in some communities been a greater emphasis than in others on refuting the allegation<br />
that FGM is a religious injunction and breaking the taboo of men as sole custodians of religion; and<br />
GAMCOTRAP shows great skill in utilizing collaborations with religious scholars. They also display a<br />
great deal of insight into geographic and ethnic variations in the practice of FGM; and presentations<br />
are angled to best resonate with community realities. During the field visit, this was particularly evident<br />
in the advice offered regarding reproductive health care surrounding consummation of marriage in<br />
communities practicing ”sealing,” (an important component of the strengthening of IEC capacity of<br />
the traditional healers who are usually the first to treat these cases), as well as in discussions about Spain’s<br />
anti-FGM law in villages that have seen many of its young people emigrate there.<br />
When asked what changes have emerged in their campaign strategies over time, they pointed to<br />
the increasing use over the last few years of traditional communicators and drawing on the cultural<br />
centrality of dance, song, and music. Also, in the past, there was more of a strategy of training a few<br />
representatives from each of many communities, while they have now realized that this places too much<br />
of a burden on a few people to return to their communities and try to recount all that they learned<br />
in training and alone attempt to effect collective change (this was also expressed in some of the field<br />
interviews as extremely challenging by attendees who pleaded for the support of workshops to be held<br />
in their communities). Now they focus instead on mass meetings and collective change through targeting<br />
a ”cluster” of villages centered around a major community (see Appendix 5 for adiagram) aimed at<br />
18
consensus building and values clarification, with the ultimate goal being participation of additional<br />
communities in the next Dropping of the Knives ceremony.<br />
Outside observers noted that GAMCOTRAP activists have ”toned down” their rhetoric over time.<br />
They felt that earlier presentations were often overly emotional and passionate and, while they could<br />
sympathize with this (given the activists’ own personal experiences with the practice), they welcomed<br />
a”cooler” and less emotional manner of delivery. In general, when chatting with ”regular” Gambians,<br />
the evaluator found that the impression of GAMCOTRAP was very positive (”those people are really<br />
working hard to help people”), which differs from often-heard comments in the late 1990s that ”these<br />
people don’t know what they are talking about.<br />
In addition, GAMCOTRAP staff seems particularly savvy when intuiting prevailing trends and<br />
adapting their ongoing message. This was made explicit in their use, at the right moment, of the<br />
visual illustrations of adverse health effects. They have also picked up on the current dialogue between<br />
Gambians at home and those who have emigrated to European countries that have passed strict anti-FGM<br />
legislation that includes clauses on extraterritoriality which makes it a crime to have a girl circumcised<br />
abroad. During the field visit, Amie Bojang consistently discussed (often in a casual manner before<br />
formal meetings commenced) the legal and social consequences were a local circumciser to agree to<br />
circumcise a European-born Gambian girl sent back to her ”home” villlage for holidays (especially those<br />
from Spain, where Isatou and Amie visisted the Gambian community in November 2008, altough this<br />
trip was not funded by the TV Project). As one circumciser in URR responded: ”We tell them we would<br />
have to be insane to take that risk.” It is likely that such a dialogue will be furthered with Gambians in<br />
Norway, where Dr. Touray conducted a workshop in December 2008.<br />
Results<br />
According to GAMCOTRAP’s reporting, the information project was carried out in each of the five<br />
proposed regions (training was held in The Central River Region, Upper River Region, and Western<br />
Region, with networking and organizational headquarters in Kanifing Municipal Area and Banjul Area),<br />
reaching a total of 117 communities. 2 The project directly reached an estimated 2,193 beneficiaries.<br />
GAMCOTRAP estimates that an additional 10,965 indirect beneficiaries were reached (using a multiplier<br />
effect of 5; see Appendix 2).<br />
Representatives were trained from all the proposed target groups, which in the proposal were identified<br />
as (primary beneficiaries): women and girls, and (secondary beneficiaries): women group leaders, village<br />
heads, district chiefs, religious scholars, traditionalists, circumcisers, TBAs, traditional healers, and<br />
people living with HIV/AIDS.<br />
The broader aim of GAMCOTRAP is to sensitize communities with the ultimate goal being a<br />
reduction in FGM prevalence and increased empowerment of women and girls, while the specific focus<br />
of this project was to: train traditional birth attendants, circumcisers, and traditional healers in order<br />
2. What are now called Regions used to be called Divisions. Thus, there was a change from: Lower River Division, Upper<br />
River Division, Central River Division, North Bank Division, Western Division, and Kombo/St.Mary Division and Banjul,<br />
to: Lower River Region, Upper River Region, Central River Region, North Bank Region, Western Region, Kanifing<br />
Municipal Area Council, and Banjul Area Council.<br />
19
to upgrade their skills and awareness regarding the harmful effects of FGM; establish networks of<br />
people living with HIV/AIDS; partner with traditional communicators and train youth drama groups;<br />
intensify Family Life Education and HIV counseling; enlist the support of traditional decision-makers;<br />
and enhance the IEC capacity of community health-providers and traditional healers.<br />
While all stakeholders must realize that it is near impossible – especially in the short term – to apply<br />
objective metrics to assess actual reductions in prevalence rates of harmful traditional practices, this<br />
evaluation found that nearly all the secondary sub-goals of the proposal appear to have been achieved to<br />
various degrees, in some cases exceeding them (for a break-down of proposed versus reached objectives,<br />
see section below. See also Appendix 4):<br />
Training sessions were held in the following communities (data from reports):<br />
• (Report, April 2006) Training Workshop for TBAs, Traditional Healers, and Herbalists on<br />
Women’s Sexual and Reproductive Health Rights, in Bansang (250 participants).<br />
• (Report, June 2006) Training Workshop for TBAs, Circumcisers, Traditional Healers (attended by<br />
Norway team), inSuduwol, with participation from 12 cluster villages (113 participants).<br />
• (Report, December 2006) Training Workshop for TBAs, Circumcisers, Parents. Sutukoba, in<br />
Wuli (100 participants).<br />
• (Report, May 2007) Training Workshop for Decisionmakers, in Sangajor, Foni, including 4<br />
villages (162 participants).<br />
• (Report, May 2007) Training Workshop for Youth (ages 16-25), in Basse (99 participants).<br />
• (Report, July 2007) Training Workshop for Senior Secondary School students from CRR, LRR,<br />
NBR, (total reached through peer educators: 841).<br />
• (Report, May 2008), Training Workshop for Traditional Communicators, Women of<br />
Reproductive Age, Circumcisers, Women’s Leaders, and TBAs, in Tambasangsang, URR,<br />
including 13 cluster villages (115 participants).<br />
• (Report 8, May 2008), Training Workshop for Traditional Decision-makers, Imams, in Kulari/<br />
Garawol, URR, including 3 communities (328 participants).<br />
• (Report 9, June 2008) Workshop for Traditional Communicators, in Bantanto CRR, including 6<br />
villages (107 participants).<br />
Network was established of nine groups of PLWHA.<br />
15 youth drama groups were trained.<br />
16 schools were reached for Family Life Education including training on FGM and HIV/<br />
AIDS.<br />
3 videos were produced:<br />
Dropping the Knives Initiative 2006 (3 minutes)<br />
Rhythms against Harmful Traditional Practices 2008 (34 minutes)<br />
Winning the Campaign against FGM 2008 (9 minutes)<br />
Dropping of the Knives celebration by 18 Circumcisers and their Communities planned<br />
and implemented on May 5, 2007, at Independence Stadium, Bakau.<br />
As a result of advocacy and training activities, 18 circumcisers and their communities were motivated<br />
to publicly declare what they have learned about FGM and that they have decided to stop the practice.<br />
These women still maintain their position as leaders in their communities and are a point of reference<br />
on women’s issues. This landmark celebration, in which seven districts took part, was the first of its kind<br />
in The Gambia and has served as an opening for other communities to follow suit.<br />
20
Knives and other instruments were dropped and circumcisers, carrying signs saying “I have stopped<br />
FGM,” recited an oath: “We the circumcisers of The Gambia, representing the cluster villages we cover<br />
have solemnly declared to the world and in particular The Gambia that we have stopped the practice<br />
of FGM in our various communities. Over the years we have received information on women’s health<br />
and have acquired knowledge about the effects of FGM on sexual and reproductive rights and the rights<br />
of the child. Having been empowered with the right information, we hereby publicly declare that we<br />
shall never involve ourselves in the practice of FGM. We take leadership responsibility in protecting and<br />
promoting the best interest of the girl child.”<br />
Each one presented with a Certificate of Honor. Alkalos were also given certificates for their support,<br />
and all clusters for their participation. Cultural performances were presented from several ethnic groups<br />
and remarks were made by: Dr. Isatou Touray, Mrs. Amé Atsu David, from Save the Children, Dr. Nestor<br />
Shivute, Resident representative to The Gambia of the WHO, and Dr. Tamsir Mbowe, Secretary of<br />
State for Health and Social Welfare.<br />
An additional 60 circumcisers have declared their intention to participate in the next<br />
Dropping of the Knives ceremony.<br />
Discussion of objectives reached as proposed<br />
General Observations<br />
A major strength of GAMCOTRAP is its sustained efforts over time and the consistency of its approach<br />
and message. While methodology has been adapted over time (as well as from community to community,<br />
depending on need), the basic mandate has remained the same, and no effort is made to conceal the true<br />
agenda of the organization. While in the past GAMCOTRAP has often been the target of criticism,<br />
insults, and even threats, it appears that over time a major shift has taken place in public awareness and<br />
attitudes, and that overall impressions of the organization are positive. Although methodological trends<br />
in anti-FGM interventions come and go, the patient consistency of GAMCOTRAP’s approach appears<br />
to be paying off, as many beneficiaries explained that “change takes time,” but that they are now ready<br />
to consider GAMCOTRAP’s message.<br />
In general, the evaluator sees the the field visit as having provided ample evidence that the targeted<br />
groups have been reached in the communities visited (and it is important to note that GAMCOTRAP<br />
did not restrict these visits, but offered the evaluator the opportunity to choose any community for a<br />
visit). Observations showed very open community discussions, even in groups including mixed age,<br />
gender, and class. One male elder in URR said: ”This may be a women’s issue, but it affects us men as<br />
well. I had one daughter who died after circumcision.”<br />
There was a sense that change was embraced without looking back, and that no blame was cast<br />
on actions past. As one woman in Basse said: ”What is past is past. Now it is the future.” Circumcisers<br />
remain respected members of their communities and continue to advice women (and many of them<br />
still practice as TBAs). People who used to engage in domestic violence are not castigated, although it is<br />
made clear that such behavior is no longer accepted. In one URR village, a man confessed that he used<br />
to beat his wife because he had simply never questioned it. After the training, he said, he realized that<br />
21
he could instead sit down and discuss with her. ”It is like I have a new wife now,” he said; and when we<br />
drove away from the village, he was standing at the side of the road, his arm around his wife, smiling.<br />
When asked about enforcement, responses varied. In one community in URR, respondents said that ”If<br />
people insist on practicing [FGM] we cannot stop them, but it seems that they aren’t.” In other communities<br />
(in URR and CRR), the councils of elders insisted that ”we are policing around” and that no one in the<br />
community could get away with either FGM , domestic violence, or giving their underage daughter away in<br />
forced marriage. Clearly, the concrete reductions in such practices remain to be seen, but the evaluator still<br />
perceives the sentiments expressed during the field visit as radically different from what was said ten years ago.<br />
A number of circumcisers professed that they were relieved to no longer have to practice FGM. One<br />
circumciser’s assistant in Wuli exclaimed: ”This is one burden I no longer have to carry!” Many mentioned<br />
that they were ready to participate in a Dropping of the Knife ceremony, and there was some indication that<br />
if this does not come to pass they may not start practicing again but will feel that they have been marginalized<br />
vis-a-vis their colleagues who participated in the first such event. Likewise, there was a lot of discussion about<br />
the equitable distribution of AEOs (again, not one of the activities funded by this project), which ranges<br />
from seed money (D10,000) for small businesses (such as soap making, tie and dye, or having a freezer to sell<br />
ice blocks and cold drinks) to raising cattle (in communities where it is not seen as appropriate for women to<br />
engage in trade). GAMCOTRAP make it very clear that such support is limited and not ongoing over time,<br />
but it seems to have significant symbolic importance, especially as ngangsingbgas are aware of others who<br />
have ”received something.” All former circumcisers were trained and supported by TANGO staff in planning<br />
and implementing their AEO. Also, male circumcisers were an important target group reached, as they tend<br />
to be the husbands of female circumcisers and it is crucial to gain their support of abandonment.<br />
Objectives Met as Proposed<br />
As is evident from the Data on Activities document (Appendix 4), all sub-goals (with one exception<br />
mentioned below) have been met or exceeded. As the expectation was stated in the original proposal,<br />
there were also of spill-over effects from the training activities. For example, in Damphakunda, on the<br />
evening of the first training day, a council of elders who were not part of the training but had heard<br />
about it, convened on their own and decided to join the project. Also, in several communities (Sutukoba,<br />
Garawol, Suduwol, Arrangel) chiefs took it upon themselves to advocate for the project in their own<br />
networks of chiefs from communities that have not been directly targeted by training. In Garawol, the<br />
council of elders planned their own follow-up meeting after the training and set up a ”community law”<br />
against FGM and early marriage and implemented ”policing” enforcement mechanisms.<br />
Video materials were reviewed during the evaluation and were found to have exceeded what was planned<br />
in the proposal, which was merely documentation for the purposes of institutional memory rather than the<br />
production of actual films. The one sub-goal that was found not to have been met (as funding ended up not<br />
being available after budget revisions) was the video screenings in 12 community halls.<br />
Interviews with staff at Mutapola revealed successful collaboration with the advocay group for women<br />
living with HIV/AIDS, having established nine networks (exceeding the proposed goal of 7). This work<br />
has particularly strengthened a gender-sensitive approach to HIV/AIDS awareness, as Mutapola is an<br />
advocacy organization specifically targeting the unique challenges and needs of women living with the<br />
virus. It was also pointed out by the CBF from Foni during the dissemination partner meeting that this<br />
project has lent a gender perspective to all development projects in the area – ”if anyone comes with a<br />
project, the women will ask how it affects them.”<br />
22
A group interview with a members of a youth group in south Kombo indicated that these youth<br />
are actively engaged and feel that they are receiving adequate support from GAMCOTRAP. All 15<br />
proposed drama groups were trained, although GAMCOTRAP points out that it is difficult to know<br />
how many are still operating.<br />
TANGO representatives spoke of GAMCOTRAP as a model NGO.<br />
Unanticipated Outcomes<br />
GAMCOTRAP staff and many interviewed beneficiaries expressed that the most surprising<br />
development of this project is how quickly change seems to recently have taken on its own momentum,<br />
and that they had honestly not expected this change to take place during their own lifetimes.<br />
The three videos that ended up being produced were not planned.<br />
When training traditional communicators, there was the unexpected result of original songs and<br />
dances spontaneously being created by women for the campaign.<br />
Many more ngangsingbas than anticipated committed to dropping their knives.<br />
An indirect outcome during the project period was the successful efforts to save foreign-born,<br />
Gambian girls from FGM and other harmful traditional practices when sent home for holidays. From<br />
2006 to 2008, GAMCOTRAP received requests related to cases from the following countries:<br />
Spain 3<br />
Germany 1<br />
United States 3<br />
United Kingdom 3<br />
Norway 2<br />
Netherlands 2<br />
Total 14<br />
Some of the potential victims were brought to The Gambia and others were in Europe and the<br />
United States at the time the request was received. Meanwhile, during the same period, 2006 – 2008,<br />
nine local cases were also reported to GAMCOTRAP, relating to FGM, early and forced marriages,<br />
rights to inheritance, and gender based violence. Women are counselled by GAMCOTRAP staff and<br />
given moral support to stand and say no to violence and any form of abuse. Their stories are used as<br />
case studies and testimonies on violence against women.<br />
In one instance during the training workshop in Damphakunda, there was the unanticipated outcome<br />
of a battered woman reporting the case to GAMCOTRAP staff and then the police, and the community<br />
holding an open discussion about domestic violence.<br />
Challenges and Adaptations<br />
While important gains were being made with former circumcisers abandoning the practice, there<br />
is an emergent threat of foreign circumcisers from the sub-region increasingly taking on the role<br />
23
of practising FGM, especially in the Western Region and the Greater Banjul Area. Clusters and<br />
communities who have decided to stop FGM have formed a strong network against roving circumcisers<br />
in the border areas of URR, LRR, CRR; and GAMCOTRAP is informed of any such attempts in<br />
these communities.<br />
The continued lack of access to state radio and TV are seen as an impediment to effective dissemination<br />
of information. The long-term goal is to address this limitation by creating community radio stations, if<br />
funding becomes available.<br />
Monitoring and Reporting<br />
Project monitoring is done on a regular basis, including surprise visits to target communities.<br />
The area of the timeliness and quality of reporting to the funders was one in which it was difficult<br />
to reach consensus during the collaborative evaluation. FOKUS requires only a yearly program report.<br />
In the view of GAMCOTRAP these were complete and submitted in a timely manner, while FOKUS/<br />
NKTF expressed that reports were late and some information was missing.<br />
In addition to these yearly reports, GAMCOTRAP produced nine narrative reports on training<br />
workshops, which were not required by FOKUS, but are seen by GAMCOTRAP and the evaluator as<br />
useful to share with community members, visitors, and potential funders.<br />
Cost Effectiveness<br />
The evaluation mandate explicitly excluded a financial audit and the evaluator did not examine<br />
financial records (independent audits were conducted for each year of project implementation, and<br />
these reports are available to interested parties). In a general sense, however, this evaluation finds that the<br />
project expenditure was cost-effective, in that all proposed sub-goals were met or exceeded (again, with<br />
the exception of community video screenings) and that, in addition, the project benefited from resources<br />
coming from elsewhere.<br />
Thus, GAMCOTRAP made effective use of previously trained CBF’s, who were not directly funded<br />
by the TV project (with the exception of receiving the same allowances for training sessions as any<br />
other participant), but do continue, without receiving a salary, to monitor and document FGM-related<br />
activities and sensitize their communities.<br />
In addition, GAMCOTRAP was able to obtain other sources of funding (see Appendix 6) for the<br />
staging of the first Dropping the Knives ceremony. Nonetheless, GAMCOTRAP stresses that the<br />
ongoing funding from FOKUS/NKTF for community training and sensitization is what prepared the<br />
ground for this event.<br />
Partnership with Norway<br />
Representatives from both NKTF/FOKUS and GAMCOTRAP reported that a lot has been learned<br />
from the partnership. On the other hand, stakeholders on both sides, as well as the evaluator, experienced<br />
difficulties and delays in communication, and identified this as an area in need of improvement.<br />
24
Conclusions and Recommendations<br />
It appears that at this time GAMCOTRAP stands at an important crossroads. After many years of<br />
sustained effort often involving extreme challenges, a shift appears to have taken place, as many Gambians<br />
are now ready to receive and consider GAMCOTRAP’s consistent message. There is currently a great<br />
sense of urgency in building on the current momentum.<br />
This recently completed three-year project is seen by GAMCOTRAP staff as having been crucial in<br />
effecting change by providing the needed funding and support. Particularly beneficial was allowing Dr.<br />
Touray to devote her time fully to coordinating the project. It also gave GAMCOTRAP the opportunity<br />
to map out large sections of the country and plan clusters to be targeted, especially in planning and<br />
organizing a second, larger Dropping of the Knives ceremony.<br />
Major activities of the project have been consistent with proposed objectives, and almost all sub-goals<br />
have been achieved to various degrees (in some cases having exceeded them), while progress appears to<br />
have been made towards reaching the broader goal of gender empowerment and the abandonment of<br />
harmful traditional practices.<br />
Beneficiaries of the project agree with GAMCOTRAP staff that it is important to continue to focus<br />
on outreach and capacity building, while pursuing the continued commitment of traditional circumcisers<br />
to drop their knives. Community members unanimously stressed the need for consistent follow-up in the<br />
form of additional workshops, improved support for CBF’s, and expanded AEOs for former circumcisers<br />
(this was not originally proposed as part of the FOKUS funding). There is a perceived need to expand<br />
efforts with youth groups, as well as to strengthen and expand work with networks of PLWHA. In<br />
addition, it is crucial to continue the outreach efforts of improving IEC capacity of traditional health<br />
practitioners and to expand the important dialogue currently underway between Gambian emigrants<br />
(particularly in Spain and Norway) and their home communities.<br />
This evaluation recommends that GAMCOTRAP continue its community outreach while<br />
striving to strengthen its administrative capacity, particularly in the area of reporting, auditing, and<br />
effective communication with donors. Specifically, it is recommended that particular care is taken in<br />
proposal writing to set realistic objectives that will be easy to document at the conclusion of a project<br />
implementation. In the current project, the proposal listed a break-down of intended beneficiaries by<br />
sub-group (such as circumcisers, TBAs, traditional healers) with separate projected numbers for each<br />
one. In the final reporting, however, these sub-groups were often combined (having attended the same<br />
workshops), making it difficult to assess the exact numbers reached in each sub-category (the situation is<br />
further complicated by the fact that one individual can have several identities, such as: ngangsingba and<br />
TBA and woman of reproductive age). Likewise, individuals living with disabilities were reached in all<br />
community workshops, rather than as a separate sub-group.<br />
GAMCOTRAP has gained organizational and administrative strength over the years, and staff members<br />
are engaged in an ongoing process of education and skills development. At this time there appears to be<br />
an acceptable level of institutional support in terms of office space, equipment, and vehicles. A major<br />
threat to GAMCOTRAP’s project sustainability is, however, the uncertainty of funding. Staff described<br />
the stress of managing from grant to grant and never knowing whether funding would be available for the<br />
next important step in project implementation (as exemplified by the current need for resources to plan a<br />
second “Dropping the Knife” ceremony). This evaluation urges for more sustained support from funders,<br />
25
while calling for improved dialogue between GAMCOTRAP and their supporters, as well as continued<br />
efforts to improve communication among Gambian organizations working on similar issues.<br />
Sources Cited<br />
Asemota, S. (2002a) “Women on Rampage over FGM Case At Magistrate Court.”<br />
Daily Observer, posted to the Web October 18. http://allafrica.com/stories/200210180124.html<br />
• (2002b) “Court Discharges Alleged Female Genital Mutilators.” Daily Observer, November 3.<br />
Daffeh, Jarai, Sheriff Dumbuya, Adelaide Sosseh-Gaye (1999) Listening to the Voice of the People:<br />
A Situational Analysis of Female Genital Mutilation in The Gambia. Banjul, The Gambia: A Study<br />
Commissioned by WHO, UNFPA, UNICEF.<br />
Forward with the Gambia, newsletter July 7, 1997.<br />
Gambian Department of State for Education. Policy Documents, Vol 1.<br />
GAMCOTRAP (April, 2006) Report on Bansang Training Workshop.<br />
• (June, 2006) Report on Suduwol Training Workshop.<br />
• (December, 2006) Report on Sutukoba Training Workshop.<br />
• (May, 2007) Report on Sangajor Training Workshop.<br />
• (May, 2007) Report on Basse Training Workshop.<br />
• (July, 2007) Report on Secondary School Training Workshop.<br />
• (July, 2007) Report on Tamasangsang Training Workshop.<br />
• (May, 2008) Report on Kulari Training Workshop.<br />
• (June, 2008) Report on Bantanto Training Workshop.<br />
Government of The Gambia/UNICEF (1998) Situational Analysis for Women and Children in The Gambia. Banjul.<br />
Government of The Gambia (1993) Housing and Household Characteristics: Population and Housing Census.<br />
Banjul: Central Statistics Department, Dept of State for Finance and Economic Affairs.<br />
Hosken, Fran (1978) “The Epidemiology of Female Genital Mutilations.” Tropical Doctor 8:150-156.<br />
Mackie, Gerry (2000) “Female Genital Cutting: The Beginning of the End.” In Shell-Duncan, Bettina<br />
and Ylva Hernlund, (eds.) Female ‘Circumcision’ in Africa: Culture, Controversy, and Change. Boulder, CO:<br />
Lynn Rienner Publishers.<br />
Singateh, Saffiatou (1985) Female Circumcision: The Gambian Experience. Banjul, The Gambia: Gambia<br />
Women’s Bureau.<br />
Touray, Isatou (1993) “Reconceptualising Traditional Practices in the Gambia: The Case of Female<br />
Genital Mutilation.” The Hague, Netherlands: Unpublished Master’s Thesis.<br />
UNICEF (2009) Monitoring the Situation of Women and Children.<br />
http://.childinfo.org/misc3.surveys.html<br />
www.gamcotrap.gm<br />
26
Appendix 1:<br />
EVALUATI<strong>ON</strong> OF GAMCOTRAP<br />
(The Gambia Committee on Traditional Practices<br />
Affecting the Health of Women and Children)<br />
“Training and Information campaign on the Eradication of FGM.”<br />
The Gambia, 2006-2008<br />
Terms of Reference<br />
Background and Problem Analysis:<br />
In Gambian society, a majority of women are poor, relatively powerless, and lack decisionmaking<br />
power over their sexuality and reproductive health. As a result, women are subjected to<br />
various forms of physical, sexual, and psychological violence. The non-governmental organization<br />
(NGO) GAMCOTRAP, the Gambian chapter of the Inter Africa Committee (IAC), has for several<br />
decades been engaged in campaigns to promote positive traditional practices, while discouraging<br />
those that negatively affect the well-being of women and the girl child, focusing in particular<br />
on abolishing Female Genital Mutilation (FGM) and early marriage, as well as on promoting<br />
education and empowerment for women and girls. GAMCOTRAP has identified FGM as a form<br />
of sexual violence against women that is often erroneously justified as a religious injunction.<br />
The broader aims of the organization include working towards a situation in which Gambian<br />
women’s voices and decisions are not taken for granted in development plans, but are considered<br />
as central issues.<br />
Objectives:<br />
The current project, funded for three years by NKTF/FOKUS Norway, is based on empowering<br />
people with the information to make informed decision and choices, with the underlying principle of<br />
citizens’ participation in their own development.<br />
The project comprised three stages, with Years 1 and 2 having consisted of campaign programs<br />
directed at various target groups. Year 3 is intended to work towards sustainability where the participants<br />
who have been identified as Community Based Facilitators will be allowed to engage in training under the<br />
supervision of GAMCOTRAP and its partners. There is an additional goal of building and sustaining<br />
collaborations with Norwegian scholars and practitioners.<br />
Geographically the project is being carried out in The Central River Region, Upper River Region,<br />
and Western Region.<br />
The overall development goal stated by GAMCOTRAP is: to reach a wide audience of all age<br />
groups to realize the belief that all individuals have the right and responsibility to promote and protect<br />
their human rights and to develop and implement relevant and effective gender-related activities that<br />
promote and protect the human rights of not only Gambian women and children, but also people living<br />
with HIV/AIDS and those living with disabilities.<br />
27
The specific goal of this project was to: upgrade the skills and knowledge of participants on the<br />
effects of FGM (including HIV/AIDS) and other harmful traditional practices.<br />
The primary beneficiaries were identified as women and girls. For the purposes of advocacy, secondary<br />
project beneficiaries included women group leaders, village heads, district chiefs, and religious scholars<br />
as influencers of decisions. The proposal states that traditionalists, circumcisers, traditional healers, and<br />
people living with HIV/AIDS will also be targeted.<br />
Specifically the project aimed to: train traditional birth attendants, circumciser s, and traditional<br />
healers; establish networks of people living with HIV/AIDS; partner with traditional communicators<br />
and train youth drama groups; intensify Family Life Education and HIV counselling; enlist the support<br />
of traditional decision-makers; enhance IEC capacity of community health providers and traditional<br />
healers; and sensitize the targeted communities, with the ultimate goal being a reduction in FGM<br />
prevalence and increased empowerment of women and girls.<br />
Purpose of the Review:<br />
After three years of funding, the project is up for evaluation. 3 This is a summative evaluation. The<br />
review will look at the impact of GAMCOTRAP’s project to educate and effect change in the area of<br />
harmful traditional practices in The Gambia. It will examine the extent that project objectives were<br />
achieved, challenges, lessons learned from the experiences, use of resources, and organization. Lessons<br />
learned about best practices will be shared for others to replicate.<br />
The evaluation will look at the process by which GAMCOTRAP staff implemented the programs<br />
and the involvement of youth, survivors, and other stakeholders, insights from the implementation, and<br />
opportunities opened up by the project.<br />
Specifically, the evaluation will focus on and assess the following aspects:<br />
Background<br />
The evaluation will describe the project as such, its background, how it came into being, how it is<br />
organized and managed, what input there has been in the form of funding and personnel and activities,<br />
and what the funding from FOKUS/NKTF has been used for. 4<br />
• What other donors have been involved, and in what networks do GAMCOTRAP and the project<br />
take part nationally<br />
Achievement of objectives and results and implementation of the project<br />
• To what extent have the project’s objectives been achieved or are expected to be achieved<br />
• What are the results of the project, and has the project generated unexpected results<br />
3. After 2008 FOKUS will not have any funding available to secure further funding of the project.<br />
4. Evaluator is not responsible for auditing or detailed financial information.<br />
28
In order to discuss the achievement of objectives and results, the evaluation will analyze and discuss<br />
these achievements vis-à-vis how the project has been planned, organized, implemented, monitored,<br />
and reported on.<br />
• How have difficulties and problems been identified, and how have they been met What<br />
adaptations and adjustments have taken place<br />
• How is the reporting on results and achievements of objectives done and what is the quality of<br />
this reporting<br />
• Which factors have promoted or impeded the implementation of the project<br />
• How have youth, survivors, and other stakeholder been involved in the project<br />
• Has the use of resources been cost-effective<br />
Relevance of the project<br />
• Which best practices can be identified and documented from GAMCOTRAP’s work in the<br />
project<br />
• Is the project relevant when it comes to successfully addressing the combating of FGM in The<br />
Gambia<br />
• Are the work methods relevant<br />
• What does the international literature say about best practices compared with the intervention<br />
and work methods used in this project (The evaluator should get a critical outsider’s perspective<br />
through consulting other stakeholders in The Gambia such as other organizations working within<br />
this field, authorities, and others).<br />
Lessons learned<br />
• What are the lessons learned in the project, and to what extent are these lessons relevant to<br />
projects that work within other contexts<br />
Extended effects of the project<br />
• Which extended effects of the project can be identified<br />
Methodology and Scope:<br />
The goals of the evaluation that have previously been identified by the organization are: to assess<br />
the training and information campaigns at the community level, and to review the organizational<br />
absorptive capacity and resources available for sustainability, as well as the overall impact of the<br />
project on the target groups. In addition, GAMCOTRAP staff prioritizes communication between<br />
the partners, and seek to answer the question: Has it been a mutual exchange of experience in working<br />
for women’s rights<br />
The evaluator will review organizational documents and program/project outputs, including video<br />
documentation, as one basis for evaluation and as a source of data on the project. Media coverage of<br />
the project will also be part of information source.<br />
29
Participatory observation of project activities and related GAMCOTRAP activities will be<br />
conducted as far as is possible during the country visit (and will complement the evaluator’s previous<br />
participant observation with GAMCOTRAP). Interviews will be conducted (using a Gambian translator<br />
independently engaged by the evaluator) among key informants - GAMCOTRAP staff and volunteers;<br />
leading decision-makers in targeted communities; Community Based Facilitators; Traditional Birth<br />
Attendants, traditional healers, and circumcisers trained by GAMCOTRAP; members of established<br />
networks of people living with HIV/AIDS; traditional communicators and representatives of youth<br />
drama groups; and students in Family Life Education classes.<br />
The review will include conceptualization of the project, planning processes, implementation,<br />
monitoring, and evaluation mechanisms. The aspects of project content, organization, sustainability,<br />
communication with partners, and administration will all be reviewed.<br />
Outputs:<br />
1. The evaluator will interview GAMCOTRAP staff and volunteers, representatives of the<br />
primary and secondary beneficiaries in a participatory manner with the assistance of<br />
GAMCOTRAP staff, and independently representatives of other agencies and organizations.<br />
2. A report of approximately 30 pages, exclusive of annexes showing the raw data from the<br />
project, will be the final output.<br />
The report is to contain:<br />
• Executive Summary with main conclusions on findings, lessons learned, and recommendations.<br />
• Background, description of project and its activities.<br />
• Answers to the questions in the ToR.<br />
• Recommendations.<br />
• Attachments.<br />
Timetable:<br />
The evaluator will spend two weeks in The Gambia during the first half of December, 2008, gathering<br />
data, and will then spend one week (in Seattle, U.S.) preparing the report. The evaluator in collaboration<br />
with the various stakeholders will then plan a dissemination workshop to be hosted by GAMCOTRAP<br />
in The Gambia during the last week of February, which will be attended by GAMCOTRAP staff,<br />
beneficiaries and local partners, the evaluator, and representatives from NKTF/FOKUS.<br />
A proposal for the evaluation report with associated guiding principles should be completed by<br />
January 1, 2009. FOKUS, NKTF, and GAMCOTRAP should give input to the report by January 15,<br />
2009. An updated version of the report, where the input from the organizations previously mentioned is<br />
taken into consideration, will be submitted to FOKUS before the seminar to be held in February 2009<br />
where input to the final version of the report will be given. The final report will be submitted to FOKUS<br />
by March 15, 2009.<br />
30
Appendix 2<br />
Sources of Information Gathered in The Gambia,<br />
November 30-December 11, 2008<br />
1. [November 30] Interview with Chair of the Board, Sidia Jatta, Bakau.<br />
2. [December 1] Introductory meeting at GamcoTRAP office, Bakau New Town, with:<br />
Amie Bojang-Cissoko, Programme Coordinator<br />
Musa Jallow, Finance Officer<br />
Haddy Saidy, Field Coordinator for Women<br />
Omar Dibba, Youth Coordinator<br />
Discussion of background of project, itinerary for trek, review of campaign videos and project reports.<br />
3. [December 2] Interview with Isatou Touray, GamcoTRAP office, Bakau New Town.<br />
4. [December 2] Interview with Amie Bojang-Cissoko, in vehicle from Bakau to Basse.<br />
5. [December 2] Meeting in Mannekunda, Basse, URR (a primarily Mandinka community in<br />
original settlement of the town), with 15 beneficiaries, including the alkalo, leaders of the men’s<br />
and women’s societies, and two former circumcisers.<br />
6. [December 2] Interview with religious leader Oustass Fayinke in his compound in Basse.<br />
7. [December 2] Meeting in Kaba Kama, URR, with a dozen beneficiaries, including Community<br />
Based Facilitator, female alkalo, leaders of women’s society, and two former circumcisers (one<br />
Mandinka, one Fula).<br />
8. [December 2] Interview with Amie-Bojang and Malick Baldeh, the CBF, at Basse guesthouse.<br />
9. [December 3] Interview with Amie Bojang-Cissoko and Malick Baldeh, in the vehicle going to<br />
Wuli.<br />
10. [December 3] Meeting in Boro Kanda Kasse (with participants also coming from Boro Manjang<br />
Kunda), Wuli. Discussion held in Serahule with about twenty beneficiaries, including CBF, alkalo,<br />
leaders of men’s and women’s societies, religious leaders, two former circumcisers.<br />
11. [December 3] Interview with alkalo of Sutukoba, Wuli.<br />
12. [December 3] Meeting in Sutukoba, Wuli with around ten beneficiaries, including TBA, leaders<br />
of men’s and women’s societies, youth leader.<br />
13. [December 3] Interviews in Makka Masireh, Wuli, with alkalo, former circumciser and her<br />
husband, and one youth leader.<br />
31
14. [December 3] Meeting in Mansayangkunda (a Fula compound) in Basse with Omar Baldeh<br />
(VDC Chair and GamcoTRAP mobilize), three women’s leaders, one men’s leader, and a group<br />
of young girls.<br />
15. [December 3] Interview with still practicing Mandinka circumciser and her two adult sons in<br />
their compound in Basse.<br />
16. [December 3] Meeting in Giroba, Fula compound of Maleck Baldeh in Basse, with around<br />
twenty women in their 20s and 30s.<br />
17. [December 4] Meeting with Governor at his office in Basse.<br />
18. [December 4] Meeting at alkalos compound in Garawol (a large, predominantly Serahule<br />
community), URR, including men’s leaders, Chief of Police, three former circumcisers, and two<br />
youth leaders.<br />
19. [December 4] Meeting in alkalo’s compound in Suduwol (a mostly Serahule community) URR,<br />
with alkalo and his (co-alkalo) brother, senior men’s council leader, a male youth leader, three<br />
women’s leaders, and a young former circumciser.<br />
20. [December 4] Meeting in Kulari (a large village, mostly Serahule and Bambara), URR, in<br />
compound of women’s council president, with one men’s leader and five women, including one<br />
former circumciser.<br />
21. [December 4] Meeting in Tambasangsang (a community of Jahankas, who are ethnically<br />
Mandinka but culturally Serahule), URR, with over a hundred community members, dominated<br />
by the local kanyeleng society, including several former circumcisers, male and female traditional<br />
leaders, and youth leaders.<br />
22. [December 4] Meeting in Damphakunda (large Jahanka community near Tambasangsang),<br />
URR, in compound of women’s leader, with kanyelengs, CBFs, TBA/ former circumciser, and a<br />
number of individuals who have participated in GamcoTRAP training.<br />
23. [December 4] Interview in vehicle with Amie Bojang-Cissoko, Malick Baldeh, and Wandefa<br />
Saidhykhan.<br />
24. [December 4] Meeting in Tinkinjo (Mandinka village), URR, with alkalo and his brother, former<br />
circumciser and her assistant, young man previously unaware of the issue.<br />
25. [December 4] Interview with Amie Bojang-Cissoko and Malick Baldeh at guesthouse in Basse.<br />
26. [December 5] Interview in Bansang, CRR, with CBF, Fatou Tarawally.<br />
27. [December 5] Meeting in Bantanto (a Mandinka community near Bansang), CRR, at bantaba<br />
with male elders (including alkalo and his two older brothers who make decisions alongside him)<br />
and former circumciser.<br />
28. [December 5] Meeting in Sareh Gideh (a Fula community near Bansang), CRR, with first the<br />
alkalo and elder men, then a group of young married women.<br />
32
29. [December 5] Meeting in Mabally Kuta (Mandinka/Jahanka community), CRR, in alkalo’s compound,<br />
with alkalo and his brother, male elders (including former circumciser’s husband), a male youth leader.<br />
30. [December 5] Meeting in Mabally Kuta in blacksmith/circumcisers’compound with members of<br />
former circumciser’s family.<br />
31. [December 5] Interview with Mabally Kuta’s former circumciser on the road as she was returning<br />
from rice fields and we passed in vehicle on the way back to Bansang.<br />
32. [December 5] Meeting in alkalo’s compound in Bansang, with alkalo (son of former circumciser)<br />
and former alkalo and other male leaders, women’s leaders, including former circumciser, and a<br />
group of young men and women.<br />
33. [December 5] Interview with TBA/former circumciser in Dobong Kunda, CRR (the planned<br />
meeting could not be held as someone just died and the entire community was in mourning).<br />
34. [December 5] Meeting in Sabally Koto, CRR, in alkalo’s compound, with male and female<br />
leaders, including former circumciser, and group of young women.<br />
35. [December 5] Interview with Amie Bojang-Cissoko in vehicle.<br />
36. [December 5] Interview in Kerewan Samba Sireh, CRR, with former circumciser in her house<br />
(also present was alkalo’s wife).<br />
37. [December 5] Interview in Kerewan Samba Sireh with religious leader in his compound.<br />
38. [December 5] Interview with Amie Bojang-Cissoko in vehicle on the way to Soma.<br />
39. [December 6] Interview in Bwiam, Foni, with Wolof religious leader who had attended workshop<br />
(planned meeting not possible as many people had left for Tabaski shopping).<br />
40. [December 6] Meeting in Arrangel, Foni, in alkalo’s compound with male and female members<br />
of his family who had attended Sibanor workshop.<br />
41. [December 6] Meeting in Batabutu Kantora, Foni, with two women (including a TBA) who had<br />
attended Sibanor workshop.<br />
42. [December 6] Meeting in Sibanor, Foni, in women’s leader’s compound, with five women.<br />
43. [December 7] Meeting in Brikama with more than twenty young women members of the Jabbi<br />
Sisters society.<br />
44. [December 7] Interview with Amie Bojang-Cissoko in Isatou Touray’s compound, Brikama.<br />
(Planned meeting in Ebo Town with traditional communicators cancelled as everyone had gone shopping<br />
for Tabaski).<br />
45. [December 7] Interview at community center in Jambanjelly with five youth activists trained as<br />
community based facilitators (representing a group of 50 youths).<br />
33
46. [December 7] Interview with Amie Bojang-Cissoko and Isatou Touray at Dr. Touray’s compound<br />
in Brikama.<br />
47. [December 7] Interview with European activist working on another anti-FGM campaign, Bakau.<br />
48. [December 7] Meeting at GamcoTRAP office, Bakau New Town, with Amie Bojang-Cissoko and<br />
Isatou Touray. Viewed additional videos and slide show on medical consequences of FGM.<br />
49. [December 10] Interview in Barra with Chair of the Board, Sidia Jatta.<br />
50. [December 10] Interview with activist from Norway, Bakau.<br />
51. [December 11] Meeting at office of Mutapola, Talinding, with four staff members/ Persons<br />
Living with HIV/AIDS.<br />
52. [December 11] Interview at GamcoTRAP office with Bakary Badjie from the Child Protection<br />
Alliance.<br />
(Interviews had to be canceled at other agencies, as people had traveled for Tabaski).<br />
53. [December 11] Concluding meeting at GamcoTRAP office with Amie Bojang-Cissoko, Isatou<br />
Touray, and Omar Dibbah, gathering of materials.<br />
54. [December 13] Interview with Isatou Touray at Yundum airport and on flight to Dakar.<br />
55. [December 13] Interview with Amie Joof-Cole, co-founder and former President of<br />
GamcoTRAP at her home in Dakar.<br />
Additional sources of information:<br />
E-mail interviews in November with representatives of Tostan and UNICEF.<br />
E-mail survey in January with stakeholders in Norway.<br />
34
GAMCOTRAP Evaluation December 2008<br />
Photos by Ylva Hernlund<br />
Bulletin board in GAMCOTRAP’s New Town<br />
office showing photos from past programs.<br />
The “Secret Clinic” (see box on upper right) is used<br />
during workshops on reproductive health with<br />
youth – any young person can submit a candid<br />
question about sex in the box and later have it<br />
answered anonymously in front of the group.<br />
Poster in GAMCOTRAP office.<br />
Dr. Isatou Touray in the GAMCOTRAP office, having just returned<br />
from a meeting in Bamako and before that a visit to Spain, a week<br />
before going to the First Ladies’ meeting in Cairo.<br />
35
After the group meeting in Mannekunda, Basse<br />
(Amie and Ylva on the left, alkalo on far right).<br />
The elder man in white in the front row told me:<br />
“This may be a women’s affair, but it affects us<br />
men, as well. One of my wives took our daughter<br />
back to her mother’s house to be circumcised. The<br />
girl died. We didn’t use to know the bad effects.”<br />
Former circumciser (next to Ylva) was given seed<br />
money to start a soap business; she says people have<br />
stopped even trying to bring girls to her to cut.<br />
Amie Bojang-Sissoho and Oustass Fayinke in his<br />
compound in Basse.<br />
Amie explained about the unique support Fayinke<br />
has been giving them: “He is not only knowledgeable<br />
in the Qu’ran, but has a deep understanding about<br />
social psychology.”<br />
Oustass Fayinke, Basse.<br />
“Things have changed a lot in the last ten years. When the real truth<br />
is revealed, there can be no argument. There is no religious scholar<br />
in the URR who will sit down and argue this issue with me.”<br />
Oustass Fayinke, Basse.<br />
“Things have changed a lot in the last ten years. When the real truth<br />
is revealed, there can be no argument. There is no religious scholar<br />
in the URR who will sit down and argue this issue with me.”<br />
Trekk lodging (a government guesthouse in Basse).<br />
36
Breakfast of canned chicken <strong>AND</strong> sardines with<br />
mayonnaise on bread...<br />
Road conditions in Wuli (bush-fires in the background),<br />
temperature 42 degrees Celsius.<br />
Ylva’s translator Wandefa Saidykhan and Amie<br />
Bojang-Sissoho debating issues over breakfast at<br />
the guesthouse in Basse.<br />
Waiting to cross the river from Basse to Wuli (the<br />
ferry operators were having their breakfast...).<br />
37
The Gambia River between Basse and Wuli.<br />
Boro Kanda Kasse (URR) group that participated<br />
in a large meeting held in Serahule. Chief Juwara,<br />
before he passed away, was a GAMCOTRAP Board<br />
member and his legacy lives on in the strong support<br />
GAMCOTRAP enjoys in this community.<br />
Amie talked a lot in this community about the Spanish<br />
anti-FGM law, as many villagers have emigrated there.<br />
One of the women said: “Human beings will follow<br />
that which there is benefit in.”<br />
Former circumciser (in white in front row) said that she was given cattle as an AEO but the animals died. “Still,”<br />
she said, “I am not going to start circumcising again.”<br />
She added: “For me, a heavy load has been lifted. One so heavy that not even a vehicle could carry it.”<br />
Boro Kanda Kasse males. Translator Wandefa<br />
Saidykhan on far right, third from right is Malick<br />
Baldeh, the CBF from Basse, who traveled with us<br />
for a few days.<br />
There was a very frank discussion between Amie<br />
and the community members about to what extent<br />
circumcisers should continue to receive alternative<br />
support.<br />
When I asked what other issues have changed,<br />
other than FGM, I was told: “We have observed that between husbands and wives there is better<br />
communication now. Love is important.”<br />
Sutukoba alkalo showing the certificate he received<br />
in GAMCOTRAP training. He got one for himself<br />
and one for the community. He has been doing<br />
outreach to ten villages; he wishes the nearby Fula<br />
communities would also get training.<br />
“We are behind Amie and Isatou. We would<br />
mobilize 10,000 people if we had to. People have<br />
stopped here. I can let you talk to 100 people here<br />
and they will all tell you they have stopped.”<br />
“Sutukoba has been given the gift from God to be<br />
able to spread the message to other places. When I was younger I was youth leader, now I am a leader<br />
of elders. People listen to me, and in any community where they will listen, I talk to them.”<br />
38
Sutukoba meeting in alkalo’s compound.<br />
When asked what changes they have seen: “Kids<br />
used to collapse because of loss of blood.”<br />
What if someone in this community disagrees and<br />
wants to circumcise their daughter<br />
“No, we have community law, a community court.<br />
We will win as a majority.”<br />
But, what if they disobey…what would be the<br />
consequences<br />
“They would be isolated by the community.”<br />
Woman is a circumciser’s daughter and was supposed to take over, but her mother told her she had<br />
stopped and she is relieved she does not have to take over.<br />
Sutukoba meeting.<br />
Young man on far right said: “When you don’t<br />
understand something, it is so difficult. It has<br />
stopped now.” He had renamed FGM: Females<br />
Gently Moving. “Also it was nice to go to Kombo<br />
[for the training] to see the electricity.”<br />
Woman 1: “There was bad communication before.<br />
Now husband and wife can sit together and discuss<br />
FGM.”<br />
Woman 2: “If someone says ‘Let me better your<br />
life’—then that’s it! The benefit will even carry to the next generation. Every human being wants a<br />
benefit. We know they [Amie and Isatou] love us and that they love our future.”<br />
Former circumciser ‘s assistant [left]: “I am the one who is now free. I don’t have to go around collecting<br />
these girl. It was a great burden.”<br />
Young man: “The man in Norway who was arrested for circumcising his daughter is from this village,<br />
but had been gone for 25 years. He should have communicated with us at home and he would have<br />
realized that we have stopped.”<br />
Amie pounding with women before a meeting.<br />
39
Makka Masireh meeting in alkalo’s compound.<br />
Kumba, the former circumciser, is wearing a GAMCO-<br />
TRAP headscarf. “Women can start something, but<br />
men have to support them.”<br />
Alkalo: “I have sympathy for the women. See how<br />
hard they work! So anything that can be done to help<br />
them, you have to support it.”<br />
Have there been other changes than FGM stopping<br />
“Yes, wife beating has stopped. The mentality has<br />
changed. It has been over a year since anyone tried to beat his wife.”<br />
But it used to happen<br />
“Yes, there would be fighting. And then you would not be friends with your wife for a week.”<br />
Elder woman: “Yes, it has changed. Quarreling has reduced.”<br />
Makka Masireh compound.<br />
There was a lot of talk about wanting a milling<br />
machine in order to reduce the workload of the<br />
women. Amie was very clear about how this is not<br />
part of their funding, but said she will try to help<br />
them write a small grant to the German Embassy,<br />
although it probably won’t be until next year<br />
because the money has already been given out for<br />
this year.<br />
Makka Masireh well. It is 55 meters deep and it takes<br />
two or three women to pull up a bucket of water.<br />
Garawol former circumcisers.<br />
“When you first hear something, if you don’t know<br />
it, then you think about it.”<br />
“We decided to stop after we learned that our<br />
relatives in Basse have also stopped.”<br />
“We received help with cattle, since women here<br />
don’t do business.”<br />
40
Garawol elders. Man in white: “I am the community<br />
police here. I make sure no one is circumcising.”<br />
Garawol meeting in alkalo’s compound.<br />
“Religious leaders made it clear to us that health is<br />
more important than anything else.”<br />
There are 16,000 Gambian Serahules in Spain.<br />
“They used to send their daughters home here to be<br />
circumcised, but now they know they can go to jail.”<br />
Amie discussed how two weeks before a girl is<br />
married she needs to go to a health professional to<br />
be safely unsealed.<br />
Garawol alkalo.<br />
“It used to be that men were in charge of boys, women of girls. No<br />
one circumcises here anymore. This community is like a family. The<br />
heads of household have all agreed and any guest that comes to stay<br />
with them has to follow the law of the village.”<br />
Amie and alkalo in Suduwol.<br />
“Wa have learned a lot. The practice is useless and it<br />
causes harm. When someone is used to something,<br />
when you tell them to stop, it won’t happen right away.<br />
But knowledge can bring change. You can’t just force<br />
people, then they accuse you of just eating money.”<br />
“There has to be dialogue rather than a law. But it will<br />
take a lot of work and resources. Look at Kantora!<br />
47 villages…. But no more than 3 or so have had<br />
a training workshop. So it is up to those people to<br />
spread the word. The CBFs need motorcycles...”<br />
41
Suduwol meeting, young former circumciser on the<br />
right. She had just been trained, had only circumcised<br />
one girl when GAMCOTRAP came.<br />
“Thank God. We were lost before.”<br />
Other issues<br />
“There is a lot of awareness now about HIV<br />
transmission. Gum tattooing is dying out, people<br />
never share the same razors, or even nail cutters.”<br />
Suduwol men.<br />
Reminded Amie of how it took days of discussion<br />
before everyone finally agreed after Oustass Fayinke<br />
spoke to them: “You have to respect those who know<br />
the religion.”<br />
“The workshop brought awareness. When you bring<br />
a lot of people together at the same time, you get it.”<br />
“The pictures [of health consequences] were<br />
important, they impress a human being. You<br />
understand the harm.”<br />
Kulari women’s leader, Isatou who was the first one<br />
to mobilize this community (she broke her leg in a<br />
road accident and it has just been set by a traditional<br />
healer).<br />
We waited in her house while a group of women,<br />
including the former circumciser, walked very far<br />
from their rice fields to come talk to us.<br />
Ngangsingba said that her first reaction was: “I hear<br />
you. But it’s my source of income.” She explained: “It<br />
is just like with a child. If you take something away<br />
from her you have to give her something else.”<br />
Then the women had training at the hospital and they stopped bringing their daughters to be cut.<br />
“I can’t say much. If the women don’t want this, there is nothing I can do. So, I put my knife down. Now I<br />
won’t even unseal brides, I tell them to go to the hospital.”<br />
Amie reinforced the message that it is very important to plan weddings in such a way that the new bride has<br />
several weeks to heal before consummation after being opened by health care professionals; this message<br />
really seemed to resonate with the women. They expressed that they are really concerned about the interim<br />
generation of young women who have already been sealed.<br />
The circumciser now raises cattle for a living, but she is still an important advisor to the women.<br />
They also see that early marriage is ending, which is positive because it reduces the harm during childbirth<br />
that happens when “a child is having a child.”<br />
42
Tambasangsang mass meeting. This is a village of<br />
Jahankas, who are ethnically Mandinka but whose<br />
cultural practices are closer to Serahule.<br />
Tambasangsang kanyeleng kaafo. These women<br />
play an important role in traditional circumcision,<br />
so are crucial to have on board for abandonment.<br />
Fanta in Tambasangsang. Amie described her as one of the<br />
most astonishing women they have ever encountered in their<br />
campaign. She heard ant-FGM messages on the radio and from<br />
talking to people in other communities who had participated<br />
in training. She paid her own transport to go all the way to<br />
Brikama, where she walked around asking people for directions<br />
to Dr. Touray’s compound. She told Isatou she wants to stop<br />
FGM in her community. GAMCOTRAP happened to be doing<br />
an education workshop that day and they invited her to come<br />
and listen, although she speaks no English. Later, she again paid<br />
for herself and three other Tambasangsang women to attend the<br />
Handing over the Knives ceremony – they didn’t tell anyone<br />
they were coming, but just showed up.<br />
She told me her own story of early forced marriage – she was married<br />
at age 13 to a man she hated. They tied her up and beat her until she<br />
submitted and “I lived like that until he died.”<br />
She is now remarried and a respected leader in her community.<br />
43
Tambasangsang kanyelengs.<br />
Fanta went to the alkalo and the circumciser and<br />
convinced GAMCOTRAP to come do training.<br />
After several preliminary meetings, the community<br />
decided at a village-wide meeting (at which they saw<br />
the visual materials on health effects) to stop FGM.<br />
Now they try to talk about it in other communities.<br />
Alkalo said: “It was Fanta who brought this. She<br />
understood something and did not keep it for herself.<br />
She was not looking for anything for herself [she has<br />
never received any payment from GAMCOTRAP].<br />
Now everyone is part of the decision and we welcome you back.”<br />
Woman: “If you identify a problem, then you have to act.”<br />
“Fanta is very effective in this community, she is the one who can enter with the women and talk about<br />
what used to be a secret between them and the circumciser.”<br />
Fatou Tarawally (on the right), a school teacher from<br />
Bansang, one of the first CBFs trained in 1997 (I<br />
met her during her training in Basse). She has been<br />
consistently involved with GAMCOTRAP since then<br />
although she does not receive any salary from them.<br />
Man and child in Bantanto. We waited as an old man<br />
on a bicycle zoomed around the village collecting<br />
people for a meeting. Then everyone spoke, from<br />
elders, down to the youngest. They told of Amie<br />
coming to hold a meeting, and how they felt when<br />
they saw the videos about health effects.<br />
“We can’t say about other places, but here we are not<br />
practicing.”<br />
“Kids are the future leaders. Anything that harms<br />
them, development will not accept. The elders do<br />
not want there to be darkness over the next generation.”<br />
There was an elder circumciser here who had just passed away and her daughter had not yet taken over<br />
because she was sick in the hospital. GAMCOTRAP happened to arrive during that time for training, so the<br />
new circumciser never did start practicing.<br />
“There have been big changes in this community. Today and yesterday, they are not the same.”<br />
An older man confessed that he used to beat his wife, but that he has gained understanding and has stopped.<br />
On the way driving out, we passed him, with his arm around her, smiling.<br />
“She is free now,” Amie said.<br />
44
Amie pounding with the women in Sareh Gideh, a<br />
Fula community.<br />
While we waited for people to walk from their farms,<br />
Amie explained to me more about site selection.<br />
Larger towns are easy to identify; then smaller villages<br />
surrounding them are selected based on size, ethnic<br />
make-up, and how they intermarry and share a<br />
circumciser.<br />
I asked if they ever approach communities that do<br />
not practice FGM and she said that yes, they did<br />
workshops in Wollof communities in northern CRR, talking about domestic violence, early marriage, family<br />
planning, and HIV prevention. In one of those villages, the issue of post-menopausal sexuality (traditionally seen<br />
as inappropriate) came up. The alkalo was pondering out loud why it is that middle-aged women suddenly stop<br />
taking care of their appearance. His wife exclaimed: “Eh! You don’t even give us soap to wash with – how are<br />
we supposed to take care of ourselves!” At a later meeting, Amie said villagers were openly laughing about how<br />
men have started having sex with their postmenopausal wives again and how happy everyone was about it.<br />
In another one of these villages, during the discussion on family planning, an older man accused young women<br />
of “just wanting to be married but not wanting to have kids.” A young woman spoke up and said that it is not<br />
that they don’t want children, but “We can’t even afford a naming ceremony for the first one, so how can we<br />
keep having one every year”<br />
Sareh Gideh, “the children’s bantaba.”<br />
Sareh Gideh. A group of young married women<br />
gathered to speak with us. They are against FGM,<br />
but the main issue they wanted to talk about was<br />
early and forced marriage and the lack of educational<br />
opportunities for women. They began sharing with<br />
us their tragic stories of sub-fertility. Most of them<br />
have been unable to get pregnant, or have suffered<br />
multiple miscarriages and/or losing their infants.<br />
When asked if they know what could improve their<br />
reproductive health, they said they don’t know, all<br />
they can do is pray. The woman in the striped top cried and said: “Everyday, I just pray to God to give me a<br />
child that will live.”<br />
I asked about the ages at which each one of them had married, and the answers were: 17,16, 15, 16, 16, 18,<br />
16, 18, and 17.<br />
I asked, when they think about the next generation of girls, what would they hope for them They gave very<br />
animated answers: They should have schooling. And stay in school until they finish and not drop out to get<br />
married. They should prosper and have children to help them in old age. They should marry for love, but not<br />
until they are at least 19 or 20. And never should they go to circumcision.<br />
45
Mabally Kuta (a Mandinka/Jahanka community).<br />
This is the kind of milling machine that so many<br />
communities are requesting.<br />
We interviewed the husband of the former<br />
circumciser (she was out in her rice field) and he<br />
said that she has stopped and that he supports her<br />
100% in her decision. “She did listen. Since last year<br />
it is like this: when people [from other communities,<br />
primarily from across the border in Senegal where<br />
the practice is illegal] she sends them away.” Or, if<br />
she is on the farm, he himself sends them away.<br />
I asked if he knows what they do next but he said he neither knows nor cares.<br />
I asked him if he is surprised that this change has come so rapidly and he exclaimed: “Actually, I am!”<br />
He did not think he would see the end of FGM in this community in his lifetime. What exactly, I asked, was<br />
it that convinced people, and he replied: “Seeing the images of health effects.”<br />
Mabally Kuta, kids using the milling machine to make groundnut butter.<br />
Amie and Fatou Tarawally.<br />
46
Jainaba, the circumciser from Mabally Kuta.<br />
After we left the meeting with her husband we ran into<br />
her on the road where she was walking from her rice<br />
field. She reiterated that she has stopped practicing<br />
and that she sends people away if they ask.<br />
But she also very strongly expressed that she felt<br />
that, like other circumcisers, she should be allowed to<br />
participate in a Handing over the Knives ceremony,<br />
and that she wants access to AEOs. Amie spoke with<br />
her very frankly about how the current funding is<br />
finished and there won’t be another ceremony unless<br />
they find more support, and how the AEO money was not part of this project budget but drawn from other<br />
sources here and there. She was very careful not to make big promises, but asked Jainaba to be patient.<br />
Jainaba listened and stressed that, no matter what, she is not going to start cuttign again because the decision<br />
has been made. But she wants to be part of the next ceremony.<br />
Bansang, meeting in the compound of the alkalo<br />
(whose mother used to be the circumciser). He said:<br />
“All is quiet here. We are keeping an ear out [for<br />
people practicing FGM].”<br />
Woman’s leader said: “What we are looking for is<br />
health. Especially for the children. That is why we<br />
are behind GAMCOTRAP.”<br />
Former alkalo (on the left) explained that this has<br />
been going on for three years and that “there has<br />
been more of a benefit than I expected.”<br />
One woman looked at Amie and said: “Amie, they used to insult you when you were talking on the radio. But<br />
now they are fully stopping. This practice is dying a natural death.”<br />
One very old woman jumped up from her seat and said “I can’t sit down when I talk about this!” She<br />
expressed how happy she is about the program. “Everyone is happy about this, but I am the most happy. Just<br />
like a driver has an apprentice, we have learned from GAMCOTRAP.”<br />
Bansang, meeting with women’s leaders. There<br />
were some tense moments here which Amie and I<br />
discussed later in the car. One of the women said<br />
that she had also been approached by BAFROW<br />
who had promised to give cell phones to all<br />
community outreach people. Amie said: “We don’t<br />
have a program that gives out mobiles.”<br />
She was very direct in saying that “this is not a<br />
competition between groups. If you want to work<br />
with BAFROW, please do so. Ultimately we are all<br />
working for the same thing.”<br />
47
Kerewan Samba Sirreh in the house of former circumciser Sunkangba Damba, one of the original 18 <br />
Kerewan Samba Sirreh in the house of former<br />
circumciser Sunkangba Damba, one of the<br />
original 18 “Sheroines” (posters on the wall and<br />
sign in the corner).<br />
Even though she is very old, she is still working in<br />
her rice fields. “I would rather farm for myself than<br />
sit in the compound all day, babysitting, screaming<br />
myself hoarse at these kids and then at the end of<br />
the day their mothers barely give me a handful of<br />
rice,” she laughed.<br />
She “Sheroines” (posters on the wall and sign in the corner). <br />
said: “Ever since our great-grandmothers we used to practice, even though there was harm in it. Life<br />
Even though she is very old, she is still working in her rice fields. “I would rather farm for myself than sit <br />
has a yesterday, a today, and a tomorrow.”<br />
in the compound all day, babysitting, screaming myself hoarse at these kids and then at the end of the <br />
day their mothers barely give me a handful of rice,” she laughed. <br />
She said: “Ever since our great‐grandmothers we used to practice, even though there was harm in it. Life <br />
has a yesterday, a today, and a tomorrow.” <br />
<br />
Interview.<br />
Jabbi Sisters in Brikama. This is a voluntary women’s<br />
organization of about 30 women, 20 or so of whom<br />
showed up for a meeting.<br />
They started leadership training with GAMCO-<br />
TRAP in 2006 and participated in Zero Tolerance<br />
celebrations.<br />
“Before, we didn’t know much about FGM. But the<br />
harm is more than the benefit.”<br />
“Even in Islam it says that if you have to circumcise,<br />
only take very little.”<br />
They told of a set of women twins, one a friend of theirs. This sister was always complaining that she did not<br />
enjoy sex and only submitted to it because it was her marital duty. She thought this was because of FGM,<br />
because her twin sister who was not circumcised professed to enjoy sex a lot. I was a bit confused about why<br />
one twin would be circumcised and not the other, but they explained that one had been fostered out and was<br />
raised in Senegal.<br />
48
Bansang, meeting in the compound of the alkalo<br />
(whose mother used to be the circumciser). He<br />
said: “All is quiet here. We are keeping an ear out<br />
[for people practicing FGM].”<br />
Woman’s leader said: “What we are looking for is<br />
health. Especially for the children. That is why we<br />
are behind GAMCOTRAP.”<br />
Former alkalo (on the left) explained that this has<br />
been going on for three years and that “there has<br />
been more of a benefit than I expected.”<br />
One woman looked at Amie and said: “Amie, they used to insult you when you were talking on the radio.<br />
But now they are fully stopping. This practice is dying a natural death.”<br />
One very old woman jumped up from her seat and said “I can’t sit down when I talk about this!” She<br />
expressed how happy she is about the program. “Everyone is happy about this, but I am the most happy.<br />
Just like a driver has an apprentice, we have learned from GAMCOTRAP.”<br />
Jabbi Sisters. “We pray for GAMCOTRAP.”<br />
49
February 24-26, 2009:<br />
Dissemination exercise, working meetings with:<br />
GAMCOTRAP:<br />
Dr. Isatou Touray - Executive Director<br />
Amie Bojang-Sissoho - Programme Coordinator<br />
Omar Dibba - Assistant Youth Coordinator<br />
Musa Jallow - Finance Officer<br />
Muhammed Singhateh - Intern<br />
NKTF:<br />
Mette Bråthen Njie<br />
Hanne Slatten<br />
February 25, Partner Meeting with:<br />
Sidia Jatta - Chairperson of the Board<br />
Olimatou Jarju - Coordinator of Mutapola<br />
Aja Nano Touray - CBF from Sibanor<br />
Yaya Jallow - Community Health Nurse from Foni<br />
Kumba Kora - CBF from Basse<br />
Fatou Bojang - CBF and former circumciser from Brikama<br />
Imam Baba Leigh - Religious Adviser, GAMCOTRAP<br />
Alh. Malick Nyang - Islamic Teacher<br />
Kebba Barrow - TANGO<br />
Interview with Ousman Jabbo, Director of TANGO<br />
50
Appendix 3<br />
Networks in which GAMCOTRAP participates<br />
International Level:<br />
Inter African Committee<br />
AMANITARE<br />
Women Living Under Muslim Laws<br />
MUSAWAH for Equality and Justice in the Muslim Family<br />
African Feminist Forum<br />
National Level:<br />
Gender Action Team<br />
Women’s Bureau<br />
GAMNASS (Gambia Network of AIDS Support Societies<br />
Mutapola (adopted from Uganda, this means Network of Positive Women Living with HIV/AIDS)<br />
Child Protection Alliance<br />
Grassroots Level:<br />
Allatentu Kafo of Ebo Town<br />
Kartong Women’s Kafo<br />
51
Appendix 4<br />
Activities completed from Under the FOKUS funded Project from 2006 to 2008<br />
Activities<br />
Training with TBAs, Circumcisers,<br />
Community Health Providers,<br />
Traditional healers, and herbalist<br />
Training with TBAs, Circumcisers,<br />
and Parents<br />
Training with Traditional Birth<br />
Attendant, Circumcisers, traditional<br />
healers and herbalists<br />
Year<br />
2006<br />
2006<br />
2006<br />
Host Community<br />
and Region<br />
Suduwol, Upper River<br />
Region<br />
Sutukoba, Upper River<br />
Region<br />
Bansang, Central River<br />
Region<br />
Number<br />
of Communities<br />
Number<br />
of Beneficiaries<br />
Male<br />
12 Communities 113 55 58<br />
6 Communities 100 30 70<br />
40 Communities 250 50 200<br />
Networking 2006 Sibanor, Western Region 2 communities 50 - 50<br />
Total trained 2006 513 135 378<br />
Female<br />
Training with Traditional<br />
Communicators, women of<br />
reproductive age, Circumcisers,<br />
women leaders and TBAs<br />
2007<br />
Tambasangang, Upper<br />
River Region<br />
11 Communities 115 26 89<br />
Training with Decision Makers 2007 Sangajor, Western Region 4 Communities 162 54 108<br />
Training information campaign with<br />
youths Drama Group<br />
Training with Schools on FLE,<br />
Reproductive Health and Traditional<br />
Practices<br />
2007 URR 20 Communities 99 42 57<br />
2007 5 Schools<br />
Central River Region<br />
Kaur Senior Secondary<br />
School<br />
200 100 100<br />
Central River Region<br />
North Bank Region<br />
Bansang Senior<br />
Secondary School<br />
Farafenni Senior<br />
Secondary School<br />
169 93 76<br />
145 64 81<br />
Lower River Region<br />
Tahir Ahmadiyya Senior<br />
Secondary School<br />
161 58 103<br />
North Bank Region<br />
Kerewan Upper Basic<br />
and Senior Secondary 166 77 89<br />
School<br />
Total trained 2007 1,217 514 703<br />
Training with Local decision Makers 2008<br />
Kulari,Garawol, Tinkinjo-<br />
URR<br />
4 communities 328 88 240<br />
Training with Traditional<br />
Communicators<br />
Training on FGM, HIV and other<br />
Traditional Practices with Women<br />
Living with HIV/AIDS<br />
2008 Bantanto – CRR 4 communities 107 35 72<br />
2008<br />
Mutapola,<br />
URR,CRR,NBR, WR &<br />
GBA<br />
9 Support Groups 28 - 28<br />
Total trained 2008 463 123 340<br />
Total trained in 3 years<br />
Estimated Indirect Beneficiaries<br />
(Total multiplied by 5)<br />
Based on the Average Family size<br />
in the Gambia 6.5<br />
2006<br />
-2008<br />
117 2,193 772 1,421<br />
10,965 3,860 7,105<br />
52
New Circumcisers for the Dropping of the Knife<br />
Number of Circumciser<br />
Regions<br />
60 Circumcisers URR, CRR and LRR<br />
Appendix 5<br />
Cluster Diagram<br />
Bansang Cluster<br />
53
Appendix 6: Contributions from other donors.<br />
D<strong>ON</strong>OR NAME<br />
C<strong>ON</strong>TRIBUTI<strong>ON</strong>S FROM O<strong>THE</strong>R D<strong>ON</strong>ORS<br />
Donor Activity / Area of Operations<br />
Equality Now<br />
Community Out Reach Activities<br />
Institutional Support to GAMCOTRAP<br />
Global Fund for Women Community Out Reach Activities / Training<br />
-<br />
Inter African Committee (IAC) Youths Programmes<br />
Operational Research<br />
P.O.Salaries<br />
AEO Materials and Feasibility Study of AEO<br />
Media Training<br />
Save the Children Fund Dakar Dropping of the Knife Celebration<br />
Community Training Activities<br />
Institutional Support to Gamcotrap<br />
Training Activities / Out Reach Activities<br />
NIYO Sweden Training Activities / Out Reach Activities<br />
Future in Our Hands (FIOH)<br />
Support to Dropping of the Knife Celebration<br />
54
International Womens committee in NKTF together with Isatou Touray<br />
at a seminar with MKBK, Oslo November 2008.<br />
Photographer: Trine Bråthen<br />
from left: Mette Bråthen Njie, Isatou Touray, Caroline Revling Erichsen,<br />
Tone Marie Falch, Hanne Slåtten.