SCCO Medical History Form
SCCO Medical History Form
SCCO Medical History Form

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Protocol: hcunliffe10-032<br />
PRIVILEGED COMMUNICATION FOR INVESTIGATIONAL USE ONLY<br />
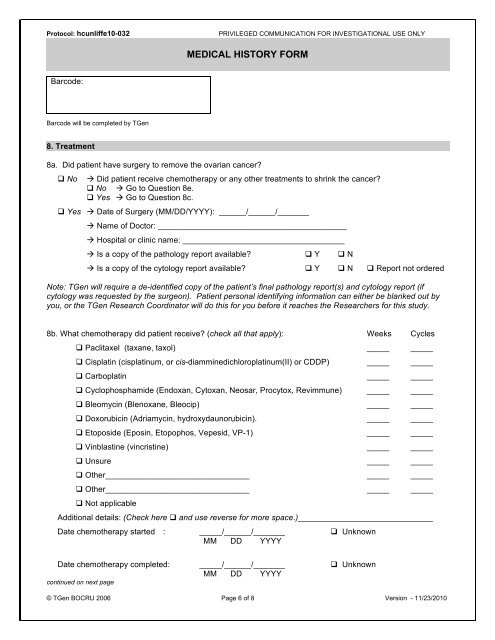
MEDICAL HISTORY FORM<br />
Barcode:<br />
Barcode will be completed by TGen<br />
8. Treatment<br />
8a. Did patient have surgery to remove the ovarian cancer<br />
No<br />
Did patient receive chemotherapy or any other treatments to shrink the cancer<br />
No Go to Question 8e.<br />
Yes Go to Question 8c.<br />
Yes Date of Surgery (MM/DD/YYYY): ______/______/_______<br />
Name of Doctor: __________________________________________<br />
Hospital or clinic name: ____________________________________<br />
Is a copy of the pathology report available Y N<br />
Is a copy of the cytology report available Y N Report not ordered<br />
Note: TGen will require a de-identified copy of the patient’s final pathology report(s) and cytology report (if<br />
cytology was requested by the surgeon). Patient personal identifying information can either be blanked out by<br />
you, or the TGen Research Coordinator will do this for you before it reaches the Researchers for this study.<br />
8b. What chemotherapy did patient receive (check all that apply): Weeks Cycles<br />
Paclitaxel (taxane, taxol) _____ _____<br />
Cisplatin (cisplatinum, or cis-diamminedichloroplatinum(II) or CDDP) _____ _____<br />
Carboplatin _____ _____<br />
Cyclophosphamide (Endoxan, Cytoxan, Neosar, Procytox, Revimmune) _____ _____<br />
Bleomycin (Blenoxane, Bleocip) _____ _____<br />
Doxorubicin (Adriamycin, hydroxydaunorubicin). _____ _____<br />
Etoposide (Eposin, Etopophos, Vepesid, VP-1) _____ _____<br />
Vinblastine (vincristine) _____ _____<br />
Unsure _____ _____<br />
Other________________________________ _____ _____<br />
Other________________________________ _____ _____<br />
Not applicable<br />
Additional details: (Check here and use reverse for more space.)______________________________<br />
Date chemotherapy started : _____/______/_______ Unknown<br />
MM DD YYYY<br />
Date chemotherapy completed: _____/______/_______ Unknown<br />
MM DD YYYY<br />
continued on next page<br />
© TGen BOCRU 2006 Page 6 of 8 Version - 11/23/2010