New Good Standing Certificate Application Form - Dubai Health ...
New Good Standing Certificate Application Form - Dubai Health ...
New Good Standing Certificate Application Form - Dubai Health ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
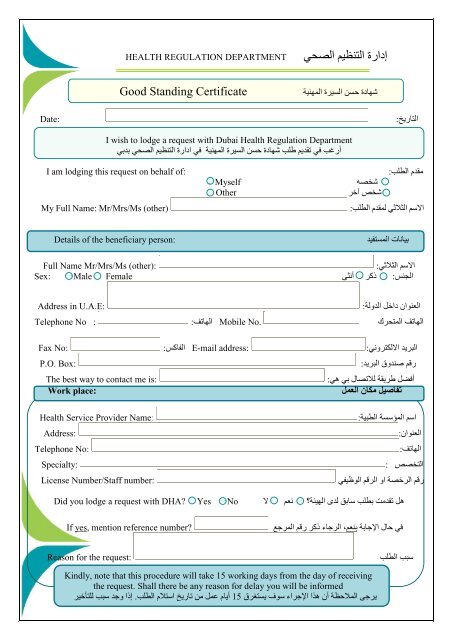
إدارة التنظيم الصح ي HEALTH REGULATION DEPARTMENT<br />
<strong>Good</strong> <strong>Standing</strong> <strong>Certificate</strong><br />
شهادة حسن السيرة المهنية<br />
Date:<br />
التاريخ :<br />
I wish to lodge a request with <strong>Dubai</strong> <strong>Health</strong> Regulation Department<br />
أرغب في تقديم طلب شهادة حسن السيرة المهنية<br />
في ادارة التنظيم الصحي بدبي<br />
I am lodging this request on behalf of:<br />
My Full Name: Mr/Mrs/Ms (other)<br />
Myself<br />
مقدم الطلب:<br />
الاسم الثلاثي لمقدم الطلب:<br />
شخصه<br />
Other<br />
شخص آخر Details of the beneficiary person:<br />
بيانات ال مستفيد<br />
Full Name Mr/Mrs/Ms (other):<br />
:<br />
الجنس : Female Sex: Male<br />
الاسم الثلاثي<br />
أنثى ذآر<br />
Address in U.A.E:<br />
Telephone No :<br />
Fax No:<br />
P.O. Box:<br />
The best way to contact me is:<br />
Work place:<br />
العنوان داخل الدولة :<br />
الهاتف المتحرك No. Mobile الهاتف :<br />
البريد الالكتروني : address: E-mail الفاآس :<br />
:<br />
رقم صندوق البريد :<br />
أفضل طريقة للاتصال بي هي<br />
تفاصيل مكان العمل<br />
<strong>Health</strong> Service Provider Name:<br />
Address:<br />
Telephone No:<br />
Specialty:<br />
License Number/Staff number:<br />
اسم المؤسسة الطبية:<br />
:<br />
العنوان :<br />
الهاتف :<br />
التخصص<br />
رقم الرخصة او الرقم الوظيفي<br />
هل تقدمت Did you lodge a request with DHA Yes No<br />
بطلب سابق لدى الهيئة؟<br />
لا نعم<br />
If yes, mention reference number<br />
في حال الإجابة بنعم، الرجاء ذآر رقم المرجع<br />
Reason for the request:<br />
سبب الطلب<br />
Kindly, note that this procedure will take 15 working days from the day of receiving<br />
the request. Shall there be any reason for delay you will be informed<br />
يرجى الملاحظة أن هذا الإجراء سوف يستغرق 15 أيام عمل من تاريخ استلام الطلب. إذا وجد سبب للتأخير
Declaration:<br />
إقرار وتصريح:<br />
For the Medical Director:*<br />
مدير المنشأة الطبية في *<br />
/<br />
أؤآد أن السيد /<br />
السيدة<br />
آان<br />
ما زال يعمل في المنشأة لدينا من<br />
حتى<br />
وأنه لم يتم وقفه أو منعه من مزاولة المهنة في إمارة دبي خلال الفترة المذآورة أعلاه. وأننا لسنا على علم بأي حدث قد يؤثر على حسن<br />
السيرة المهنية.<br />
التوقيع:----- --- -- ---- ---- --- -الختم:---- ---- --- ------ ---<br />
الاسم الثلاثي:<br />
التاريخ:<br />
The Medical Director of ,<br />
I affirm that Mr. / Ms. is / was working in our facility from Till<br />
And during this period he was not disqualified, suspended or prohibited from practicing his / her<br />
profession in Emirate of <strong>Dubai</strong>. And we are not aware of any matters that call into question of his / her<br />
good standing.<br />
Name:<br />
Signature: ___________Stamp: _____________ Date:<br />
For the Applicant:<br />
إنني أقر بأن البيانات المذآورة أعلاه صحيحة و آاملة<br />
يحق لإدارة التنظيم الصحي رفض الطلبات أو توجيهها للجهات المعنية حسب الشروط والأحكام<br />
التوقيع:----- --- - ---- ---- --- --- ---- --- --- -<br />
الاسم الثلاثي:<br />
التاريخ:<br />
I confirm that the information given in this form and in supporting documents is true to the best of my<br />
knowledge and belief.<br />
The health regulation department has the right to reject your request if the evidence is inadequate or not<br />
clear.<br />
Name:<br />
Signature: _______________Date:<br />
* Medical Director OR Equivalent who can sign on behalf of the Facility<br />
(e.g. CEO, Director of Nursing, or Director of HR)
لتقديم الطلب الرجاء التواصل معنا عن طريق<br />
قسم التسجيل و الاعتماد – إدارة التنظيم الصحي هيئه الصحة –دبي<br />
الهاتف:4298900<br />
الفاآس:043113133<br />
مكتب رقم 1017 الطابق الأول<br />
بناية الرازي مبنى رقم<br />
مدينة دبي الطبية<br />
الشبكة الالكترونية:<br />
البريد الالكتروني<br />
:<br />
-<br />
64<br />
04<br />
www.dha.gov.ae<br />
Regulation@dha.gov.ae<br />
If you need to contact us for any reason our contact details are:<br />
Registration and Accreditation Section- <strong>Health</strong> Regulation Department- <strong>Dubai</strong> <strong>Health</strong> Authority<br />
Telephone: (04) 4298900<br />
Fax Number:043113133<br />
<strong>Dubai</strong> <strong>Health</strong>care City<br />
Al-Razi Building, Building 64 Block C<br />
First Floor, Office Number 1017<br />
Website: www.dha.gov.ae<br />
E-mail: Regulation@dha.gov.ae<br />
: