Health & Wellness - Emerson Hospital
Health & Wellness - Emerson Hospital
Health & Wellness - Emerson Hospital

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
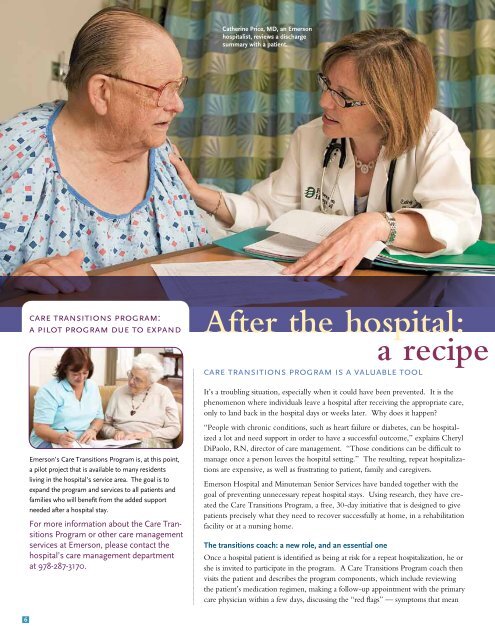
Catherine Price, MD, an <strong>Emerson</strong><br />
hospitalist, reviews a discharge<br />
summary with a patient.<br />
care transitions program:<br />
a pilot program due to expand<br />
<strong>Emerson</strong>’s Care Transitions Program is, at this point,<br />
a pilot project that is available to many residents<br />
living in the hospital’s service area. The goal is to<br />
expand the program and services to all patients and<br />
families who will benefit from the added support<br />
needed after a hospital stay.<br />
For more information about the Care Transitions<br />
Program or other care management<br />
services at <strong>Emerson</strong>, please contact the<br />
hospital’s care management department<br />
at 978-287-3170.<br />
After the hospital:<br />
a recipe<br />
care transitions program is a valuable tool<br />
It’s a troubling situation, especially when it could have been prevented. It is the<br />
phenomenon where individuals leave a hospital after receiving the appropriate care,<br />
only to land back in the hospital days or weeks later. Why does it happen<br />
“People with chronic conditions, such as heart failure or diabetes, can be hospitalized<br />
a lot and need support in order to have a successful outcome,” explains Cheryl<br />
DiPaolo, RN, director of care management. “Those conditions can be difficult to<br />
manage once a person leaves the hospital setting.” The resulting, repeat hospitalizations<br />
are expensive, as well as frustrating to patient, family and caregivers.<br />
<strong>Emerson</strong> <strong>Hospital</strong> and Minuteman Senior Services have banded together with the<br />
goal of preventing unnecessary repeat hospital stays. Using research, they have created<br />
the Care Transitions Program, a free, 30-day initiative that is designed to give<br />
patients precisely what they need to recover successfully at home, in a rehabilitation<br />
facility or at a nursing home.<br />
The transitions coach: a new role, and an essential one<br />
Once a hospital patient is identified as being at risk for a repeat hospitalization, he or<br />
she is invited to participate in the program. A Care Transitions Program coach then<br />
visits the patient and describes the program components, which include reviewing<br />
the patient’s medication regimen, making a follow-up appointment with the primary<br />
care physician within a few days, discussing the “red flags” — symptoms that mean<br />
6