Continuation of Group Optional Life Coverage Form
Continuation of Group Optional Life Coverage Form
Continuation of Group Optional Life Coverage Form

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Dear Retiree:<br />
Congratulations on your Retirement! As a retiree <strong>of</strong> an employer participating in the State insurance<br />
benefits <strong>of</strong>fered through the South Carolina Public Employee Benefit Authority (PEBA), you are eligible<br />
to continue your optional group life insurance coverage. Your premium will not be deducted from your<br />
retirement annuity payment. You will be billed directly by Met<strong>Life</strong> for this insurance coverage.<br />
Your first quarterly billing statement will be sent under separate cover. Please pay special attention to the<br />
payment due date reflected on that statement.<br />
In order for you to take advantage <strong>of</strong> this option, Met<strong>Life</strong> must receive page 2 <strong>of</strong> this letter back within 31<br />
days from the date <strong>of</strong> your retirement. This will be your only chance to take advantage <strong>of</strong> this<br />
opportunity. If you are not yet age 70, your existing coverage will be reduced at age 70 to an amount<br />
equal to 65% <strong>of</strong> the original amount in force. In the future, if you decide that you are no longer interested<br />
in maintaining this life insurance coverage, you may cancel at any time by calling our Customer Service<br />
Center at the number below.<br />
Also enclosed is a Beneficiary Designation <strong>Form</strong>. Please take a moment to complete this beneficiary<br />
designation form to ensure your life insurance benefits are paid according to your wishes. Please complete<br />
the form and return it along with the election portion <strong>of</strong> this letter to Met<strong>Life</strong> at the following address.<br />
Met<strong>Life</strong> Recordkeeping Center<br />
P. O. Box 14401<br />
Lexington, KY 40512-4401<br />
Fax: 1-866-545-7517<br />
If you should have any questions regarding this letter or your options as a retiree, you may contact the<br />
Met<strong>Life</strong> Customer Service Center at 866-492-6983, Monday through Friday, between the hours <strong>of</strong> 8:00<br />
AM and 11:00 PM Eastern Time.<br />
Sincerely,<br />
Met<strong>Life</strong> Recordkeeping Services<br />
Encl. Beneficiary Designation <strong>Form</strong><br />
L0613329332 [exp1215][All States][DC,GU,MP,PR,VI]<br />
Metropolitan <strong>Life</strong> Insurance Company, New York, NY
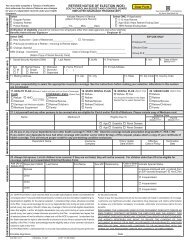
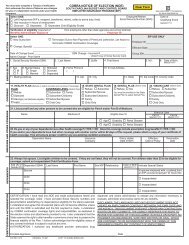
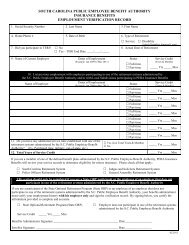
The State <strong>of</strong> South Carolina. Policy Number: 9143046<br />
Employee Information: Employee SSN _______________<br />
________________________________________ _____________<br />
Last Name First Name Middle Initial DOB (mm/dd/yy)<br />
________________________________________________________________<br />
Address City State Zip Code<br />
My current insurance coverage amount is $_______________ (To be completed by Benefits<br />
Administrator or Public Employee Benefit Authority staff), and I wish to continue my insurance coverage in the<br />
amount <strong>of</strong> $_______________ (Increments <strong>of</strong> $10,000).<br />
<strong>Optional</strong> <strong>Life</strong> Ins. Amt.<br />
If there has been a reduction in coverage due to age, please provide the amount <strong>of</strong> coverage prior to reduction<br />
$________________<br />
____________Last Day Worked<br />
__________________Active <strong>Group</strong> <strong>Coverage</strong> Termination Effective Date<br />
____________ Date <strong>of</strong> Retirement<br />
Retiree Signature_____________________________<br />
Date____________________<br />
I UNDERSTAND THAT THE INSURANCE I WISH TO CONTINUE WILL NOT BECOME EFFECTIVE UNLESS I HAVE<br />
FULLY COMPLETED THIS FORM. THIS FORM MUST BE COMPLETED IN ITS ENTIRETY OR IT WILL BE RETURNED<br />
TO ME.<br />
Benefits Administrator Name (Print): ______________________<br />
Employer <strong>Group</strong> #:_____________________________________<br />
Employer <strong>Group</strong> Name: _______________________________________<br />
Signature <strong>of</strong> verification by Benefits Administrator ______________________Date______________<br />
(Or Public Employee Benefit Authority staff).<br />
____________________________________________________________________________________<br />
I HAVE ALREADY RECEIVED A PORTION OF MY COVERAGE UNDER THE ACCELERATED BENEFITS OPTION (ABO)<br />
AND UNDERSTAND MY CONTINUED COVERAGE WILL EQUAL THE REMAINING COVERAGE IN EFFECT.<br />
Retiree Signature (If applicable) ________________________<br />
Date_____________________<br />
L0613329332 [exp1215][All States][DC,GU,MP,PR,VI]<br />
Metropolitan <strong>Life</strong> Insurance Company, New York, NY