2008 National Immunisation Schedule Health Provider booklet
2008 National Immunisation Schedule Health Provider booklet
2008 National Immunisation Schedule Health Provider booklet

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>2008</strong> <strong>National</strong><br />
<strong>Immunisation</strong> <strong>Schedule</strong><br />
<strong>Health</strong> <strong>Provider</strong> Booklet
Published in May <strong>2008</strong> by the<br />
Ministry of <strong>Health</strong><br />
PO Box 5013, Wellington, New Zealand<br />
ISBN 978-0-478-31748-0 (print)<br />
ISBN 978-0-478-31749 (online)<br />
HP 4575<br />
This document is available on the Ministry of <strong>Health</strong>’s website:<br />
http://www.moh.govt.nz
Contents<br />
Introduction 1<br />
Informed consent 1<br />
Eligibility for schedule vaccines 1<br />
1 <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong> 2<br />
1.1 <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong> 2<br />
1.2 Changes to the <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong> 2<br />
1.3 Other schedule vaccines – Td, Hepatitis B, BCG 3<br />
1.4 Ordering <strong>2008</strong> <strong>Schedule</strong> vaccines 4<br />
1.5 How to claim the immunisation benefit – <strong>Health</strong>PAC Information 4<br />
1.6 What to do with unused 2006 schedule vaccines 4<br />
1.7 <strong>Health</strong> education resources 5<br />
1.8 NIR forms 5<br />
1.9 Who to contact if you have questions 5<br />
2 Key Points 6<br />
2.1 dTap (Boostrix TM ) vaccine 6<br />
2.2 DTaP-IPV-HepB/Hib (Infanrix®-hexa) vaccine 7<br />
2.3 PCV7 (Prevenar®) vaccine 10<br />
2.4 MeNZB TM vaccine 13<br />
2.5 Expansion of the high risk pneumococcal programme for children under five years of<br />
age with a chronic condition 16<br />
2.6 HPV immunisation programme 18<br />
2.7 New schedule vaccine presentation and administration 21<br />
3 dTap (Boostrix) Vaccine and Pertussis Epidemiology 23<br />
3.1 dTap (Boostrix TM ) vaccine schedule 23<br />
3.2 Rationale for introducing the dTap vaccine 23<br />
3.3 Pertussis epidemiology 23<br />
3.4 dTap (Boostrix TM ) vaccine information 25<br />
3.5 Other recommendations 27<br />
3.6 <strong>National</strong> <strong>Immunisation</strong> Register and School Based Vaccination System 28<br />
4 DTaP-IPV-HepB/Hib (INFANRIX ® -hexa) 29<br />
4.1 Early introduction of DTaP-IPV-HepB/Hib from March <strong>2008</strong> 29<br />
4.2 DTaP-IPV-HepB/Hib vaccine schedule – from 1 June <strong>2008</strong> 29<br />
4.3 Change in type of Hib vaccine 29<br />
4.4 DTaP-IPV-HepB/Hib vaccine information 29<br />
4.5 DTaP-IPV-HepB/Hib vaccine and the <strong>National</strong> <strong>Immunisation</strong> Register 33<br />
4.6 DTaP-IPV-HepB/Hib vaccine and claiming the immunisation benefit 33<br />
5 Pneumococcal Conjugate Vaccine (PCV7, Prevenar ® ) and<br />
Pneumococcal Epidemiology 34<br />
<strong>2008</strong> <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong>: <strong>Health</strong> <strong>Provider</strong> Booklet iii
5.1 PCV7 vaccine schedule – from 1 June <strong>2008</strong> 34<br />
5.2 Pneumococcal disease 34<br />
5.3 Epidemiology 36<br />
5.4 Effects of introducing pneumococcal vaccine onto the infant immunisation programme 39<br />
5.5 Immunogenicity and efficacy of pneumococcal conjugate vaccine 45<br />
5.6 PCV7 vaccine information 46<br />
5.7 PCV7 vaccine and the <strong>National</strong> <strong>Immunisation</strong> Register – <strong>National</strong> <strong>Immunisation</strong><br />
<strong>Schedule</strong> only 48<br />
5.8 PCV7 vaccine and claiming the immunisation benefit – Childhood <strong>Immunisation</strong><br />
<strong>Schedule</strong> only 48<br />
6 Expansion of the High Risk Pneumococcal Programme for<br />
Children under Five Years of Age with a Chronic Condition 49<br />
6.1 Addition of new eligible groups 49<br />
6.2 High risk pneumococcal programme immunisation schedule 49<br />
6.3 Entering high-risk pneumococcal programme vaccines on the <strong>National</strong> <strong>Immunisation</strong><br />
Register 50<br />
6.4 Claiming for high-risk pneumococcal programme vaccines 51<br />
Appendix 1: <strong>Immunisation</strong> Catch-up <strong>Schedule</strong>s 52<br />
1.1 <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong> catch-up schedules 52<br />
1.2 High risk pneumococcal immunisation programme catch-up schedules 55<br />
Appendix 2: Pre/Post Splenectomy <strong>Immunisation</strong> Programme 56<br />
References 58<br />
List of Tables<br />
Table 1.1: <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong> from 1 June <strong>2008</strong> 2<br />
Table 2.1: PCV7 vaccine catch-up programme 10<br />
Table 2.2: Eligibility criteria for high-risk pneumococcal programme 16<br />
Table 5.1: PCV7 vaccine schedule 34<br />
Table 6.1: Eligibility criteria for high-risk pneumococcal programme 49<br />
Table 6.2:<br />
<strong>Schedule</strong> for pneumococcal vaccines for children at higher risk of pneumococcal<br />
disease with no prior history of pneumococcal vaccines 50<br />
List of Figures<br />
Figure 3.1: Notifications of pertussis in New Zealand (all ages), 2001–2007 24<br />
Figure 3.2: Age-specific rates of pertussis in New Zealand 2000–2006 24<br />
Figure 5.1: Pneumococcal disease spectrum (for use as a guide only) 35<br />
Figure 5.2: Hospitalisations from pneumococcal meningitis in children under two years of age,<br />
1999–2006 37<br />
Figure 5.3: Hospitalisations from pneumococcal septicaemia in children under two years of age,<br />
1999–2006 38<br />
Figure 5.4: Rate of vaccine-type (VT) invasive pneumococcal disease (IPD) before and after<br />
introduction of pneumococcal conjugate vaccine (PCV7), by age group and year;<br />
Active Bacterial Core surveillance, United States, 1998–2003 40<br />
iv<br />
<strong>2008</strong> <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong>: <strong>Health</strong> <strong>Provider</strong> Booklet
Introduction<br />
This <strong>booklet</strong> includes the following information about the <strong>2008</strong> <strong>National</strong> <strong>Immunisation</strong><br />
<strong>Schedule</strong> (<strong>Schedule</strong>):<br />
• changes to the <strong>Schedule</strong> in <strong>2008</strong><br />
• new vaccines (rationale for introduction, vaccine schedules, efficacy, safety)<br />
• information on stopping the MeNZB vaccine special programme (see Key Points)<br />
• children starting on or changing to the <strong>2008</strong> <strong>Schedule</strong> (Catch-up <strong>Schedule</strong>s)<br />
• key points information on the HPV (human papillomavirus) <strong>Immunisation</strong> Programme<br />
• vaccine ordering information<br />
• <strong>National</strong> <strong>Immunisation</strong> Register updates<br />
• immunisation benefit claims<br />
• what to do with unused 2006 schedule vaccines<br />
• an update on immunisation resources available for providers and parents<br />
• who to contact if you have questions.<br />
Informed consent<br />
The Ministry of <strong>Health</strong> recommends immunisation however it is a parent’s choice to<br />
immunise their child. For more information on informed consent refer to the<br />
<strong>Immunisation</strong> Handbook 2006.<br />
Eligibility for schedule vaccines<br />
Children under 16 years of age<br />
All children under 16 years of age are eligible for free <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong><br />
vaccines (http://www.moh.govt.nz/moh.nsf/indexmh/eligibility-healthservices-doctor).<br />
Unimmunised adults<br />
Unimmunised adults 16 years and over are eligible for free primary courses of the<br />
following vaccines:<br />
• Td (three doses)<br />
• MMR (two doses)<br />
• IPV (three doses)<br />
• Hepatitis B (three doses – household and sexual contacts of hepatitis B carriers<br />
only).<br />
The immunisation benefit may be claimed for these vaccines.<br />
<strong>2008</strong> <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong>: <strong>Health</strong> <strong>Provider</strong> Booklet 1
1 <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong><br />
1.1 <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong><br />
Table 1.1: <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong> from 1 June <strong>2008</strong><br />
<strong>Immunisation</strong> given<br />
Brand name<br />
DTaP-IPV-<br />
HepB/Hib<br />
Infanrix®-<br />
Hexa<br />
PCV7 Hib MMR DTaP-IPV dTap* HPV**<br />
Prevenar® Hiberix M-M-R® II Infanrix-IPV Boostrix Gardasil®<br />
Manufacturer GSK Wyeth GSK MSD GSK GSK CSL<br />
6 weeks • •<br />
3 months • •<br />
5 months • •<br />
15 months • • •<br />
4 years • •<br />
11 years •<br />
12 years<br />
girls only<br />
* From 1 January dTap is given to 11-year-old children.<br />
** From 2009<br />
Vaccine key<br />
D = diphtheria; T = tetanus; aP = acellular pertussis; HepB = hepatitis B; IPV = inactivated polio vaccine;<br />
Hib = Haemophilus influenzae type b; PCV7 = 7-valent pneumococcal conjugate vaccine;<br />
MMR = measles-mumps-rubella; d = adult dose diphtheria; ap = adult dose acellular pertussis, HPV =<br />
human papillomavirus.<br />
• 3 doses<br />
1.2 Changes to the <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong><br />
From January <strong>2008</strong><br />
• dTap (Boostrix TM ) vaccine is given at age 11 years instead of dTap-IPV.<br />
From March <strong>2008</strong><br />
• Introduction of DTaP-IPV-HepB/Hib (Infanrix®-hexa) vaccine instead of DTaP-IPV<br />
(Infanrix-IPV) and Hib-HepB (Comvax®) at age six weeks and three and five<br />
months.<br />
2 <strong>2008</strong> <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong>: <strong>Health</strong> <strong>Provider</strong> Booklet
From 1 June <strong>2008</strong><br />
• Introduction of pneumococcal conjugate (PCV7, Prevenar®) vaccine for all babies<br />
born from 1 January <strong>2008</strong>.<br />
• Introduction of DTaP-IPV-HepB/Hib (Infanrix®-hexa) vaccine for all babies.<br />
• Cessation of meningococcal B (MeNZB TM ) vaccine special programme.<br />
• Expansion of high-risk pneumococcal programme for children under five years of<br />
age.<br />
From 1 September <strong>2008</strong><br />
• Introduction of the human papillomavirus (HPV) vaccine for young women aged<br />
17 and 18 years (i.e. born in 1990 and 1991).<br />
From early 2009<br />
• Introduction of the HPV vaccine onto the <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong> for 12 year<br />
old girls (in primary care and health clinics) and girls in school Year 8.<br />
• HPV vaccine given to girls aged 13 to 18 years. Delivery of HPV vaccine to these<br />
cohorts will be phased over 2009 and 2010.<br />
For further information about the new vaccines refer to the section 2 Key Points and<br />
sections 3 to 6.<br />
1.3 Other schedule vaccines – Td, Hepatitis B, BCG<br />
There are no changes in the <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong> for the Td, Hepatitis B,<br />
and BCG vaccines.<br />
Practitioners are reminded that all pregnant women should be assessed for:<br />
• their hepatitis B status (HBsAg or HBeAg positive) in early pregnancy<br />
• the risk of tuberculosis for their baby.<br />
Neonatal BCG should be offered to newborns at increased risk for tuberculosis, see the<br />
<strong>Immunisation</strong> Handbook 2006, chapter 12, page 248 (Ministry of <strong>Health</strong> 2006).<br />
Please ensure that all babies of mothers who are HBsAg or HBeAg positive receive:<br />
• hepatitis B vaccine and hepatitis B immunoglobulin at birth; and<br />
• doses of hepatitis B vaccine at six weeks and three and five months.<br />
The baby’s serology must be checked at age five months, at the time of the fourth dose, to<br />
check for immunity/infection. See the <strong>Immunisation</strong> Handbook 2006, Figure 3.3,<br />
page 134 for details (Ministry of <strong>Health</strong> 2006).<br />
<strong>2008</strong> <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong>: <strong>Health</strong> <strong>Provider</strong> Booklet 3
1.4 Ordering <strong>2008</strong> <strong>Schedule</strong> vaccines<br />
All schedule vaccines can be ordered by fax through ProPharma:<br />
• dTap (Boostrix) is available to order<br />
• DTaP-IPV-HepB/Hib (Infanrix®-hexa) is available to order<br />
• PCV7 (Prevenar®) is available to order.<br />
• While no longer recommended for routine use, the MeNZB vaccine can continue to<br />
be accessed from ProPharma (See Sections 2 and 6 for more information on the use<br />
of the MeNZB vaccine) from 1 June <strong>2008</strong>.<br />
• HPV (GARDASIL®) can be ordered by primary care providers from August <strong>2008</strong> and<br />
will be available for school immunisation programmes to order in early 2009.<br />
Please ring ProPharma on 0800 400 101 if you:<br />
• do not have a ProPharma account<br />
• need a fax order form.<br />
1.5 How to claim the immunisation benefit – <strong>Health</strong>PAC Information<br />
See Section 2 Key Points and Sections 3-7 for more detailed information on claiming for<br />
specific vaccines.<br />
For information about claiming from <strong>Health</strong>PAC and error codes and their meanings,<br />
please refer to the Ministry’s Frequently Asked Questions webpage at:<br />
http://www.moh.govt.nz/moh.nsf/indexmh/healthpac-faq-immunisation<br />
For <strong>Health</strong>PAC claim forms, please phone Wickliffe Press on 0800 259 138 and quote<br />
your payee number.<br />
1.6 What to do with unused 2006 schedule vaccines<br />
Hib-HepB vaccine – COMVAX ®<br />
From 1 June <strong>2008</strong>, all unused stock of Hib-HepB vaccine (Comvax®) should be<br />
returned to ProPharma.<br />
Hepatitis B vaccine – HBvaxPRO ®<br />
The hepatitis B vaccine (HBvaxPRO) doses for children should be retained if the<br />
practice is likely to use these vaccines before the expiry date.<br />
Note that the birth dose of hepatitis B is given to those babies born to mothers who<br />
carry the hepatitis B virus (see section 8).<br />
DTaP-IPV – INFANRIX TM -IPV<br />
DTaP-IPV vaccine (Infanrix®-IPV) will continue to be used for the immunisation event at<br />
age four years.<br />
4 <strong>2008</strong> <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong>: <strong>Health</strong> <strong>Provider</strong> Booklet
1.7 <strong>Health</strong> education resources<br />
The Ministry of <strong>Health</strong> immunisation resources will be updated to include all the <strong>2008</strong><br />
changes to the <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong>. These updated resources can be<br />
ordered through the <strong>Health</strong>Ed website: http://www.healthed.govt.nz.<br />
A new resource has been developed to provide parents and caregivers with further<br />
information on the pneumococcal vaccine (PCV7, Prevenar®). This resource can be<br />
ordered through the <strong>Health</strong>Ed website: http://www.healthed.govt.nz.<br />
1.8 NIR forms<br />
NIR forms are being updated for the <strong>2008</strong> <strong>Schedule</strong> effective from 1 June <strong>2008</strong>.<br />
To reorder NIR forms:<br />
• Phone: (04) 496 2277<br />
• Email: moh@wickliffe.co.nz<br />
• Fax: 0800 802 126.<br />
Please quote the reference number printed on the form with any order made.<br />
1.9 Who to contact if you have questions<br />
Vaccine ordering<br />
<strong>Immunisation</strong> benefit claiming<br />
Reordering NIR forms<br />
Technical Advice<br />
<strong>National</strong> <strong>Immunisation</strong><br />
Programme<br />
Propharma<br />
0800 400 101<br />
<strong>Health</strong>PAC<br />
0800 458 448<br />
www.moh.govt.nz/moh.nsf/indexmh/healthpac-faq-immunisation<br />
moh@wickliffe.co.nz<br />
Fax 0800 802 126<br />
<strong>Immunisation</strong> Advisory Centre (IMAC)<br />
0800 IMMUNE or 0800 466 863<br />
www.immune.org.nz<br />
• <strong>National</strong> <strong>Immunisation</strong> Programme queries:<br />
immunisation@moh.govt.nz<br />
• General immunisation information/ <strong>Immunisation</strong> Handbook 2006:<br />
www.moh.govt.nz/immunisation<br />
<strong>2008</strong> <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong>: <strong>Health</strong> <strong>Provider</strong> Booklet 5
2 Key Points<br />
2.1 dTap (Boostrix TM ) vaccine<br />
For further detailed information about the adult diphtheria, tetanus, adult acellular<br />
pertussis (dTap, Boostrix TM ) vaccine, see section 3 and the Boostrix TM data sheet (refer<br />
to the Medsafe data sheets at:<br />
http://www.medsafe.govt.nz/profs/Datasheet/dsform.asp).<br />
Note: The dTap vaccine is delivered as a school-based (year 7) immunisation<br />
programme in the North Island and Nelson Marlborough DHBs and by primary health<br />
care services in the remainder of the South Island.<br />
Why was dTap introduced<br />
From 1 January <strong>2008</strong>, the dTap (Boostrix TM ) vaccine replaced the dTap-IPV (Boostrix®-<br />
IPV) vaccine on the <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong> at 11 years of age. From <strong>2008</strong>, all<br />
11-year-old children will have already received the recommended four doses of polio<br />
vaccine in childhood.<br />
Will dTap vaccine be recorded on the <strong>National</strong> <strong>Immunisation</strong> Register<br />
In primary health care situations, dTap vaccine will not be recorded on the <strong>National</strong><br />
<strong>Immunisation</strong> Register (NIR) as 11-year-old students are not in the NIR’s birth cohort.<br />
The School Based Vaccination System (SBVS) has been updated for the introduction of<br />
the dTap vaccine. The SBVS will not provide details of dTap vaccine events to the NIR.<br />
Why should dTap vaccine be delayed until two years after receipt of a tetanusdiphtheria<br />
vaccine (eg, Td vaccine after an injury)<br />
This delay in administering dTap aims to decrease the risk and severity of a local<br />
reaction at the injection site. This precaution may be waived if a pertussis epidemic is<br />
beginning and the student lives in a household with an unimmunised younger sibling or<br />
a pregnant woman.<br />
Students who have received Td vaccinations in the past two years should be referred to<br />
their general practitioner for follow-up and recall. The dTap vaccine should be offered<br />
to these students before they reach 16 years of age.<br />
If the child received a Td vaccine booster three to five years ago, dTap immunisation is<br />
recommended.<br />
6 <strong>2008</strong> <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong>: <strong>Health</strong> <strong>Provider</strong> Booklet
2.2 DTaP-IPV-HepB/Hib (Infanrix®-hexa) vaccine<br />
For further detailed information about Infanrix®-hexa, see section 4, and the Infanrix®hexa<br />
data sheet (refer to the Medsafe data sheets at:<br />
http://www.medsafe.govt.nz/profs/Datasheet/dsform.asp).<br />
Why was DTaP-IPV-HepB/Hib (Infanrix®-hexa) introduced in mid-March <strong>2008</strong><br />
Due to Hib-HepB (Comvax®) vaccine manufacturing problems, New Zealand was not<br />
able to secure further supplies of Comvax® vaccine beyond March <strong>2008</strong>. Stocks of<br />
Comvax® vaccine have run out, and DTaP-IPV-HepB/Hib (Infanrix®-hexa) vaccine is<br />
now available.<br />
Please continue to use your practice’s supply of Comvax® vaccine until it has run out.<br />
Who is eligible for the DTaP-IPV-HepB/Hib (Infanrix®-hexa) vaccine<br />
All babies due for their six-week, three-month or five-month immunisations are eligible<br />
for the Infanrix®-hexa vaccine.<br />
The Ministry of <strong>Health</strong> recommends Infanrix®-hexa also be given to children at five<br />
months of age, replacing DTaP-IPV and HepB (HBvaxPRO). However DTaP-IPV and<br />
HepB vaccines may still be given to five-month-old babies until 1 June <strong>2008</strong>.<br />
A change of vaccine within a primary series is safe and expected to be effective.<br />
The introduction of Infanrix®-hexa vaccine means there will be two injections given at<br />
six weeks and three and five months of age (Prevenar® and Infanrix®-hexa).<br />
How is DTaP-IPV-HepB/Hib (Infanrix®-hexa) administered<br />
Infanrix®-hexa vaccine is administered by intramuscular injection into the thigh.<br />
Note: The Infanrix®-hexa and Prevenar® vaccines should be given in separate limbs<br />
Infanrix®-hexa vaccine must be reconstituted prior to administration as follows.<br />
• Attach the 25-gauge needle to the pre-filled syringe.<br />
• Transfer the syringe’s liquid suspension to the vial containing the Hib pellet.<br />
• Shake the vial well to ensure the Hib pellet is completely dissolved.<br />
• Draw the reconstituted vaccine back into the syringe.<br />
• Attach the 23-gauge needle to the syringe for vaccine administration.<br />
• After reconstitution, the vaccine should be injected promptly.<br />
• However, the vaccine may be kept for up to eight hours at room temperature (21°C).<br />
<strong>2008</strong> <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong>: <strong>Health</strong> <strong>Provider</strong> Booklet 7
DTaP-IPV-HepB/Hib (Infanrix®-hexa) and PCV7 (Prevenar®) – fever management<br />
A higher incidence of fever (> 39.5°C) was reported in infants receiving Infanrix®-hexa<br />
and Prevenar® compared to infants receiving Infanrix®-hexa vaccine alone. (See<br />
section 4.4 for more information.)<br />
How to manage fever<br />
• Give the baby extra fluids to drink (more breastfeeds or water).<br />
• Do not overdress the baby if hot.<br />
• Paracetamol may be given for pain relief before immunisation.<br />
The Hib component of DTaP-IPV-HepB/Hib (Infanrix®-hexa) is different to that of<br />
the Hib-HepB (Comvax®) vaccine. What does this mean for disease protection<br />
The Haemophilus influenzae type b (Hib) component of the Hib-HepB vaccine was<br />
previously used as a schedule vaccine because it offers protection after a single dose –<br />
as early as six weeks of age. The Hib component of the Infanrix®-hexa vaccine does<br />
not offer this early protection.<br />
There is a small risk that Hib disease will re-emerge with this change. However, the<br />
incidence of Hib disease in New Zealand has significantly declined since Hib vaccine<br />
was introduced in 1994, with five to 10 cases occurring every year in unimmunised<br />
children.<br />
Following the vaccine change, Hib disease will be monitored using the existing<br />
surveillance systems.<br />
Can alternatives to DTaP-IPV-HepB/Hib (Infanrix®-hexa) vaccine be given<br />
When a child has a genuine contraindication to a component of the Infanrix®-hexa<br />
vaccine, alternative vaccines may be given (if available) and the immunisation benefit<br />
claimed.<br />
How do I enter DTaP-IPV-HepB/Hib (Infanrix®-hexa) onto the <strong>National</strong><br />
<strong>Immunisation</strong> Register<br />
PMS and NIR upgrades for Infanrix®-hexa are expected from 1 June <strong>2008</strong>.<br />
Before 1 June <strong>2008</strong>, enter Infanrix®-hexa into the Patient Management System (PMS)<br />
as two separate vaccines (two events). Therefore:<br />
• enter Hib-HepB (or HepB) and then enter DTaP-IPV as separate events (as you<br />
currently do with the 2006 <strong>National</strong> Childhood <strong>Immunisation</strong> <strong>Schedule</strong>)<br />
• enter the same Infanrix®-hexa batch number and expiry date into both events’ batch<br />
number and expiry field.<br />
Note: Prior to 1 June <strong>2008</strong>, this will be recorded in your PMS and the NIR as if two<br />
separate vaccinations were given.<br />
8 <strong>2008</strong> <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong>: <strong>Health</strong> <strong>Provider</strong> Booklet
From 1 June <strong>2008</strong>, the NIR will record the Infanrix®-hexa vaccine events as part of the<br />
<strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong>.<br />
How do I claim the immunisation benefit for Infanrix®-hexa vaccinations given<br />
<strong>Health</strong>PAC payment systems will not be updated for Infanrix®-hexa until 1 June <strong>2008</strong>.<br />
Before 1 June <strong>2008</strong>, for the six-week, three and five-months events claim as though<br />
DTaP-IPV and Hib-HepB or HepB vaccines were given, that is, record the DTaP-IPV-<br />
HepB/Hib (Infanrix®-hexa) vaccination event as if two separate vaccinations were<br />
given.<br />
From 1 June <strong>2008</strong>, <strong>Health</strong>PAC payment systems will accept claims for the DTaP-IPV-<br />
HepB/Hib (Infanrix®-hexa) vaccine.<br />
<strong>2008</strong> <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong>: <strong>Health</strong> <strong>Provider</strong> Booklet 9
2.3 PCV7 (Prevenar®) vaccine<br />
For further detailed information about PCV7 (Prevenar®) and pneumococcal disease,<br />
see section 5 and the Prevenar® data sheet (refer to the Medsafe data sheets at:<br />
http://www.medsafe.govt.nz/profs/Datasheet/dsform.asp).<br />
Why is the PCV7 vaccine being added to the <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong><br />
from 1 June <strong>2008</strong><br />
PCV7 vaccine protects young children against the seven most common strains of the<br />
Streptococcus pneumoniae bacteria that cause severe pneumococcal disease. Severe<br />
pneumococcal disease can cause meningitis, blood poisoning and pneumonia. All<br />
babies are at risk of severe pneumococcal disease.<br />
The pneumococcus is the most common bacterial cause of otitis media in children and<br />
a frequent cause of sinusitis and pneumonia in all age groups.<br />
Who is eligible for the PCV7 vaccine<br />
All babies born from 1 January <strong>2008</strong> will be eligible to receive PCV7 vaccine from<br />
1 June <strong>2008</strong>.<br />
What is the PCV7 vaccine schedule<br />
From 1 June <strong>2008</strong>, all new babies beginning their childhood immunisations will be<br />
offered the PCV7 vaccine. These babies will receive four doses of the PCV7 vaccine at<br />
the same time as other <strong>Schedule</strong> vaccines at age six weeks and three, five and<br />
15 months of age (see the <strong>2008</strong> <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong> table in section 1).<br />
Babies born from 1 January <strong>2008</strong> will receive a catch-up schedule for PCV7 vaccine.<br />
What is the catch-up programme for PCV7 vaccine<br />
A catch-up programme is available for babies born from 1 January <strong>2008</strong>. These<br />
children can receive PCV7 vaccine from 1 June <strong>2008</strong>. (See the PCV7 vaccine schedule<br />
below for the number of doses required for the age of the baby at catch up.)<br />
Table 2.1: PCV7 vaccine catch-up programme<br />
Age of baby at PCV7 dose 1<br />
PCV7 vaccine schedule<br />
6 weeks to 6 months 6 weeks, 3 months, 5 months, 15 months of age OR<br />
3 doses 6 to 8 weeks apart + 1 dose at age 15 months<br />
7 months to 11 months of age* 2 doses 6 weeks apart + 1 dose at age 15 months<br />
12 to 23 months* 2 doses of PCV7 given 6 to 8 weeks apart<br />
* Applies only to babies born from 1 January <strong>2008</strong>.<br />
This catch-up programme is in place because children aged under one year are at<br />
greatest risk of severe pneumococcal disease.<br />
10 <strong>2008</strong> <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong>: <strong>Health</strong> <strong>Provider</strong> Booklet
PCV7 (Prevenar®) and DTaP-IPV-HepB/Hib (Infanrix®-hexa) – fever management<br />
A higher incidence of fever (> 39.5°C) was reported in infants receiving Infanrix®-hexa<br />
and Prevenar® compared to infants receiving Infanrix®-hexa vaccine alone (see section<br />
4.4 for more information).<br />
How to manage fever<br />
• Give the baby extra fluids to drink (more breastfeeds or water).<br />
• Do not overdress the baby if hot.<br />
• Paracetamol may be given for pain relief before immunisation.<br />
Avoid giving PCV7 (Prevenar®) at the same visit as MeNZB vaccine<br />
While no problems are anticipated, either in the immune response or safety, there is no<br />
data to support giving the MeNZB TM vaccine at the same practice visit as Prevenar®.<br />
Therefore, where parents are anxious for their child to receive the MeNZB vaccine<br />
and the doctor agrees, a three-dose course of the MeNZB vaccine could start at six<br />
months of age (doses six weeks apart).<br />
See section 2.4 for more information on the eligibility for the MeNZB vaccine from<br />
1 June <strong>2008</strong>.<br />
How do I enter the PCV7 vaccine on the <strong>National</strong> <strong>Immunisation</strong> Register<br />
From 1 June <strong>2008</strong>, the NIR will record PCV7 vaccine events as part of the <strong>National</strong><br />
<strong>Immunisation</strong> <strong>Schedule</strong> for:<br />
• new babies beginning their immunisations<br />
• babies born from 1 January <strong>2008</strong> on a catch-up schedule.<br />
Note: The above information does not apply to children receiving PCV7 vaccine as part<br />
of the high-risk pneumococcal or pre/post-splenectomy programmes (see section 6 and<br />
Appendix 2). Information for the high risk pneumococcal or pre/post splenectomy<br />
programmes is recorded on the NIR as the ‘Pneumococcal’ programme.<br />
How do I claim the immunisation benefit for the PCV7 vaccine<br />
From 1 June <strong>2008</strong>, immunisation benefit claims for the PCV7 vaccine will be valid if<br />
administered from 1 June <strong>2008</strong>. Note: Any immunisation benefit claims for PCV7<br />
vaccine administered as a schedule vaccine before 1 June <strong>2008</strong> will be rejected.<br />
Note: <strong>Immunisation</strong> benefit claims for the PCV7 vaccine as a schedule vaccine are valid<br />
for babies with a birth date from 1 January <strong>2008</strong>. <strong>Immunisation</strong> benefit claims for the<br />
PCV7 <strong>Schedule</strong> vaccine will be rejected if the vaccine has been administered to babies<br />
with a birth date before 1 January <strong>2008</strong>.<br />
<strong>2008</strong> <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong>: <strong>Health</strong> <strong>Provider</strong> Booklet 11
How is PCV7 vaccine expected to benefit New Zealand<br />
The introduction of PCV7 vaccine to the infant immunisation schedule in the United<br />
States has resulted in a decline in severe pneumococcal disease incidence in young<br />
children and a decline in invasive pneumococcal disease (IPD) in unimmunised adults.<br />
In New Zealand in 2006, there were 151 children aged under five years of age with IPD.<br />
By comparing the pneumococcal strains that caused their disease against the seven<br />
strains in the pneumococcal vaccine, ESR predicted that 83% of pneumococcal disease<br />
in children under five years could have been prevented by using the pneumococcal<br />
vaccine.<br />
Is invasive pneumococcal disease notifiable<br />
It is planned that IPD will be added to the list of infectious diseases to be notified by<br />
medical practitioners and by laboratories before the vaccine programme starts in<br />
June <strong>2008</strong>.<br />
Will there be pneumococcal serotype replacement following the introduction of<br />
PCV7 vaccine<br />
In the United States, surveillance results suggest some serotype replacement had<br />
occurred in the three years after the introduction of PCV7 vaccine to infants. However,<br />
the burden of IPD in young children remained lower than in the years before the<br />
introduction of Prevenar®. See section 5.4.<br />
Therefore, ongoing surveillance of IPD in New Zealand will be important to monitor for<br />
any serotype replacement. Longer term, the development of expanded valency<br />
vaccines will be important.<br />
12 <strong>2008</strong> <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong>: <strong>Health</strong> <strong>Provider</strong> Booklet
2.4 MeNZB TM vaccine<br />
From 1 June <strong>2008</strong>, the meningococcal B vaccine special programme will be stopped.<br />
Babies will no longer routinely be offered the MeNZB vaccine.<br />
Why is the MeNZB TM programme stopping from 1 June <strong>2008</strong><br />
The MeNZB vaccine was introduced to control an epidemic of a specific strain of<br />
Group B meningococcus circulating in New Zealand. The programme started in 2004,<br />
and by the end of December 2006, three doses of MeNZB vaccine had been offered<br />
to all children and young people aged six weeks to 19 years in New Zealand. From<br />
January 2007, the MeNZB vaccine has only been available for children under the age<br />
of five years and to individuals at higher risk.<br />
The programme will be discontinued from 1 June <strong>2008</strong> for the following reasons.<br />
• The incidence of invasive meningococcal disease has decreased from a high of<br />
651 cases in 2001, when 370 cases were found to have the epidemic strain, to<br />
105 cases in 2007, of whom, 47 individuals were confirmed as having the disease<br />
due to the epidemic strain. The Meningococcal B vaccine special programme has<br />
successfully reduced cases of meningococcal disease.<br />
• It is known from the clinical trials that protection from meningococcal disease may not<br />
be long term, suggesting that the vaccine may be best used to stop an epidemic<br />
rather than for a long-term schedule vaccine.<br />
• Coverage data from the NIR shows that only 58% of infants received the fourth dose<br />
of MeNZB vaccine at the age of 10 months (for children enrolled on the NIR from<br />
1 January 2006 to 1 January <strong>2008</strong>).<br />
• There is no data to support the co-administration of MeNZB vaccine with<br />
Prevenar® vaccine, and therefore the timing of administering the vaccines would<br />
have to be changed. Adding more visits to the immunisation programme to give<br />
three doses of MeNZB after the age of six months is unlikely to be popular with<br />
parents or health providers.<br />
Can children who have started the MeNZB TM course finish it<br />
Yes, a child may complete a course of MeNZB vaccine. Parents and children should<br />
be encouraged to complete the course before 31 December <strong>2008</strong>, although the vaccine<br />
will still be available after that date.<br />
Is the MeNZB TM vaccine still available if parents request it for their child<br />
Yes, if the parent of a child or young person up to 19 years of age requests that the<br />
child receives a course of MeNZB vaccine, and the doctor thinks the child is at risk,<br />
the MeNZB vaccine will still be available and funded. A GP may start the child’s<br />
course of MeNZB without further authorisation, and the immunisation benefit may be<br />
claimed.<br />
<strong>2008</strong> <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong>: <strong>Health</strong> <strong>Provider</strong> Booklet 13
Avoid giving MeNZB TM at same visit as the PCV7 (Prevenar®) vaccine<br />
While no problems are anticipated, either in the immune response or safety, there is no<br />
data to support giving the MeNZB TM vaccine at the same practice visit as PCV7<br />
(Prevenar®). Therefore, where parents are anxious for their child to receive the<br />
MeNZB vaccine and the doctor agrees, a three-dose course of the MeNZB vaccine<br />
could start at six months of age (doses six weeks apart).<br />
See sections 2.3 and 5 for more information about the PCV7 (Prevenar®) vaccine.<br />
Is the MeNZB TM vaccine still available for certain occupational groups<br />
Yes, the MeNZB vaccine will still be available for microbiologist and laboratory<br />
workers. See the <strong>Immunisation</strong> Handbook 2006, page 301 (Ministry of <strong>Health</strong> 2006).<br />
Is the MeNZB TM vaccine still available for certain high-risk groups<br />
Yes, the vaccine will still be available for individuals of any age with a high risk of<br />
invasive meningococcal infection and specific conditions (three doses of MeNZB<br />
vaccines at six-week intervals). Specific conditions include:<br />
• actual or functional asplenia (Individuals scheduled for MeNZB vaccine presplenectomy<br />
will need to have completed their MeNZB vaccine course (all three<br />
doses) at least four weeks before the scheduled operation date)<br />
• sickle cell anaemia<br />
• deficiencies of the terminal complement components<br />
• individuals with HIV infection, who may be safely immunised with meningococcal<br />
polysaccharide vaccines.<br />
See the <strong>Immunisation</strong> Handbook 2006, page 302 (Ministry of <strong>Health</strong> 2006).<br />
How effective is the MeNZB TM vaccine<br />
A study looking at the effectiveness of MeNZB vaccine up to the end of December<br />
2006 estimated that the MeNZB vaccine was effective, with an estimated efficacy of<br />
68% (Kelly et al 2007). The estimate will be reassessed using data up to the end of<br />
2007.<br />
Will the MeNZB TM vaccine be recorded on the <strong>National</strong> <strong>Immunisation</strong> Register<br />
after 1 June <strong>2008</strong><br />
It is important to record all MeNZB vaccine doses given those up to 19 years of age.<br />
From 1 June <strong>2008</strong> the <strong>National</strong> <strong>Immunisation</strong> Register will continue to accept<br />
information on MeNZB vaccine doses administered to those up to 19 years of age.<br />
The NIR messaging and scheduling for the MeNZB vaccine will stop for newborns.<br />
14 <strong>2008</strong> <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong>: <strong>Health</strong> <strong>Provider</strong> Booklet
How do I claim for the MeNZB TM vaccine given after 1 June <strong>2008</strong><br />
While no longer recommended for routine use the <strong>Immunisation</strong> Benefit may be claimed<br />
for administration of the MeNZB vaccine, where:<br />
• a doctor assesses there to be an indication of high risk of disease<br />
• parents feel that their child under twenty years of age is at special risk and the doctor<br />
agrees to MeNZB vaccination.<br />
Use claim code IMMB and the applicable indication code.<br />
Will ongoing surveillance of Meningococcal Disease continue<br />
The Ministry of <strong>Health</strong> will continue to monitor meningococcal disease and will consider<br />
reintroducing a meningococcal B immunisation programme if it is needed.<br />
Even though meningococcal B epidemic strain disease rates are low, the disease is still<br />
present. The MeNZB vaccine protects against the strain of meningococcal B causing<br />
the epidemic, but it will not protect against other strains. This is why New Zealanders<br />
should be reminded to watch out for the signs and symptoms of this disease, and seek<br />
medical help immediately if they are concerned. <strong>Health</strong> practitioners need to be aware<br />
of the risk of meningococcal disease in individuals presenting with illness particularly<br />
young children.<br />
<strong>2008</strong> <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong>: <strong>Health</strong> <strong>Provider</strong> Booklet 15
2.5 Expansion of the high risk pneumococcal programme for<br />
children under five years of age with a chronic condition<br />
The table below shows the eligibility criteria for the high-risk pneumococcal programme<br />
for children under five years of age from 1 June <strong>2008</strong>.<br />
Table 2.2: Eligibility criteria for high-risk pneumococcal programme<br />
Children aged under five years with the following conditions:<br />
On immunosuppressive or radiation<br />
therapy<br />
Primary immune deficiencies<br />
HIV<br />
Renal failure or nephrotic syndrome<br />
Organ transplants<br />
Cochlear implants or intracranial shunts<br />
With chronic CSF leaks<br />
On corticosteroid therapy for more than two weeks, at<br />
daily dose of prednisone of 2 mg/kg or greater, or a total<br />
daily dosage of 20 mg or more<br />
Children pre or post splenectomy or with functional<br />
asplenia*<br />
Pre-term infants, born at under 28 weeks’ gestation<br />
Chronic pulmonary disease (including asthma<br />
treated with high-dose corticosteroid therapy)<br />
Cardiac disease with cyanosis or failure<br />
Insulin dependent diabetes<br />
Down’s syndrome<br />
* See Appendix 2 – Pre/post Splenectomy <strong>Immunisation</strong> Programme.<br />
Note: See bold text for the additional funded chronic conditions from 1 June <strong>2008</strong>.<br />
Children who meet the criteria are eligible for:<br />
• PCV7 (pneumococcal conjugate, Prevenar®) vaccine<br />
• 23PPV (pneumococcal polysaccharide, Pneumovax®23) vaccine.<br />
See Table 6.2 for the high risk pneumococcal programme immunisation schedule.<br />
Catch-up schedules for children who have already received one or more doses of<br />
pneumococcal vaccine are found in Appendix 1.<br />
How do I enter the high-risk pneumococcal programme vaccines on the <strong>National</strong><br />
<strong>Immunisation</strong> Register (NIR)<br />
Children born prior to 1 January <strong>2008</strong><br />
Children born prior to 1 January <strong>2008</strong> and identified as meeting the eligibility criteria for<br />
the high-risk pneumococcal programme (see Table 6.1) will continue to have their<br />
pneumococcal vaccines (PCV7 and 23PPV) entered onto the NIR using the<br />
pneumococcal programme.<br />
16 <strong>2008</strong> <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong>: <strong>Health</strong> <strong>Provider</strong> Booklet
Children born between 1 January <strong>2008</strong> and 31 May <strong>2008</strong><br />
Children born between 1 January <strong>2008</strong> and 31 May <strong>2008</strong> who have commenced the<br />
high-risk pneumococcal programme would have already been entered on the NIR as<br />
part of the pneumococcal programme (PI). They will continue to receive PCV7 under<br />
this programme, and it will not be scheduled for them under NIR Childhood <strong>Schedule</strong><br />
(CI) <strong>2008</strong>.<br />
Children can receive PCV7 under either CI or PI programmes, with a cross-check<br />
making sure that PCV7 is not scheduled under both.<br />
From 1 June <strong>2008</strong>, these high-risk children will automatically transfer to the CI and their<br />
remaining PCV7 doses will recorded as part of this CI schedule.<br />
When the high-risk child turns two years old and receives 23PPV vaccine, the PI<br />
programme takes over for these children (on the basis of the NIR receiving a 23PPV<br />
vaccine, an indicator of high risk).<br />
Children born from 1 June <strong>2008</strong><br />
PCV7 is included on the <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong> from 1 June <strong>2008</strong> for all<br />
children. PCV7 doses given to high-risk children born from 1 June <strong>2008</strong> will be<br />
recorded on the CI schedule of the NIR. When the high-risk child turns two years old<br />
and receives 23 PPV vaccine, the PI programme takes over for these children (on the<br />
basis of the NIR receiving a 23 PPV vaccine, an indicator of high risk).<br />
How do I claim for high-risk pneumococcal programme vaccines<br />
The immunisation benefit can be claimed for vaccines given as part of the high-risk<br />
pneumococcal programme for children under five years of age with a chronic condition.<br />
Claim using the codes as follows:<br />
• Vaccine 100 (PCV7) and indication 12 (at risk, no previous history), 13 (at risk,<br />
previous PCV7) or 14 (at risk, previous 23 PPV).<br />
• Or, if the PCV7 vaccine is given at six weeks, three or five months as part of the<br />
usual <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong> you may claim as a usual <strong>Schedule</strong> vaccine,<br />
and when the child receives a dose of 23PPV vaccine please claim under the high<br />
risk pneumococcal programme<br />
For further details on the High Risk Pneumococcal Programme for children under five<br />
years of age with chronic medical conditions refer to section 6.<br />
<strong>2008</strong> <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong>: <strong>Health</strong> <strong>Provider</strong> Booklet 17
2.6 HPV immunisation programme<br />
More detailed information on the Human Papillomavirus (HPV) <strong>Immunisation</strong><br />
Programme will be provided later in <strong>2008</strong> once discussions with District <strong>Health</strong> Boards<br />
and the Ministry of Education are complete.<br />
What is the HPV <strong>Immunisation</strong> Programme<br />
The HPV <strong>Immunisation</strong> Programme aims to reduce cervical cancer in New Zealand by<br />
protecting girls and young women against HPV infection caused by the HPV types<br />
present in the vaccine. Currently, around 160 New Zealand women each year are<br />
diagnosed with cervical cancer and 60 women per year die from cervical cancer.<br />
Girls and young women aged 12 to 18 years will be offered the HPV vaccine<br />
(Gardasil®) to protect against the two most common infections (HPV types 16 and 18)<br />
that can lead to cervical cancer and the HPV types (6 and 11) that cause most genital<br />
warts.<br />
Who will be eligible for the HPV vaccine<br />
Girls born on or after 1 January 1990 will be eligible for the HPV vaccine. The HPV<br />
immunisation programme will be introduced in stages, beginning with the oldest girls<br />
first.<br />
From 1 September <strong>2008</strong><br />
• Girls aged 17 and 18 years (born in 1990 and 1991) will be able to receive HPV<br />
vaccine from primary care or health clinics.<br />
From 2009<br />
• HPV vaccine will be part of the <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong> for 12 year old girls<br />
(in primary care and health clinics) and girls in school Year 8, see Table 1.1.<br />
• HPV vaccine will be offered to girls aged 13 to 18 years. Delivery of HPV vaccine to<br />
these girls will be phased over 2009 and 2010. More information about cohort<br />
phasing will follow later in <strong>2008</strong>.<br />
What is the HPV vaccine schedule<br />
Three doses of Gardasil® are given over a six month period.<br />
Number of HPV vaccine schedule<br />
doses<br />
1 st dose<br />
2 nd dose 2 months after the 1 st dose<br />
3 rd dose 6 months after the 1 st dose<br />
(4 months after the 2 nd dose)<br />
18 <strong>2008</strong> <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong>: <strong>Health</strong> <strong>Provider</strong> Booklet
What is HPV infection<br />
HPV is a common virus that is spread through skin to skin contact. Some types of HPV<br />
infection can cause cell changes that may lead to cervical cancer, and these types are<br />
spread through sexual contact. Other strains can cause warts but those strains do not<br />
lead to cancer. Most women who develop HPV infections clear the virus naturally and<br />
do not develop cervical cancer. About four out of five people have HPV infection at<br />
some time in their lives.<br />
There is no treatment for HPV infections, but there is treatment for the health problems<br />
that HPV can cause (such as warts, abnormal changes to cervical cells, and cancers).<br />
What is in the Gardasil® vaccine<br />
The vaccine contains HPV virus-like particles (VLPs) of HPV types 16, 18, 6 and 11.<br />
These particles are proteins from the outer shell of the virus. They are a part of the virus<br />
but are not live and cannot cause infection. The particles mimic the HPV structure so<br />
that the immune system makes antibodies against it. The vaccine does not contain<br />
thiomersal. These recombinant types of vaccine have been used around the world for<br />
about 20 years.<br />
For more vaccine information, see the Gardasil® data sheet (refer to the Medsafe data<br />
sheets at: http://www.medsafe.govt.nz/profs/Datasheet/dsform.asp).<br />
How effective is the HPV vaccine, and how long does it last<br />
Gardasil® vaccine targets the types of HPV responsible for most cases of cervical<br />
cancer (types 16 and 18) and genital warts (types 6 and 11). Clinical trials show<br />
Gardasil® is highly effective in preventing these types of HPV in young women who<br />
have not previously been exposed to them.<br />
So far, ongoing studies show the vaccine protects against HPV infection for five years<br />
after immunisation, and suggest protection will last much longer. Research is continuing<br />
to find out how long protection will last.<br />
Gardasil® does not protect against all types of HPV that can cause cervical cancer.<br />
And, as with any vaccine, Gardasil® may not provide protection for everyone who is<br />
vaccinated.<br />
<strong>National</strong> Cervical Screening Programme<br />
There will be no changes to the <strong>National</strong> Cervical Screening Programme. All women<br />
should have regular cervical smear tests every three years from the age of 20 until they<br />
turn 70 if they have been sexually active.<br />
How safe is the HPV vaccine<br />
Vaccine safety was assessed in five clinical trials (four of which were placebo<br />
controlled); 6,160 subjects received Gardasil® and 4,064 received placebo.<br />
<strong>2008</strong> <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong>: <strong>Health</strong> <strong>Provider</strong> Booklet 19
Reported reactions at one to five days post-vaccination included:<br />
• pain at the injection site (81%)<br />
• swelling (24%)<br />
• redness (23%)<br />
• erythema (3%)<br />
• pruritis (3%).<br />
Overall, 94% rated their injection-site adverse experience to be mild or moderate in<br />
intensity.<br />
Ten percent of vaccinees experienced fever. Bronchospasm was reported very rarely.<br />
There have been post-approval reports of fainting (syncope) occurring after vaccination<br />
with Gardasil®. This can follow any vaccination and requires careful observation of the<br />
person being vaccinated for at least 15 minutes after administration.<br />
Other adverse experiences reported during post-approval use have been reported,<br />
however it is difficult to accurately quantify and determine causation. Other reported<br />
adverse experiences include: lymphadenopathy, dizziness, headache, Guillian-Barre<br />
syndrome, nausea, vomiting, arthralgia, myalgia, fatigue, and malaise.<br />
Gardasil has been licensed for use in more than 100 countries, including New Zealand,<br />
Australia, Canada, the United States, and the 27 countries in the European Union<br />
including the United Kingdom.<br />
Will the HPV vaccine be recorded on the <strong>National</strong> <strong>Immunisation</strong> Register<br />
The <strong>National</strong> <strong>Immunisation</strong> Register will record HPV vaccine events given as part of the<br />
HPV <strong>Immunisation</strong> Programme and <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong>.<br />
The School Based Vaccination System (SBVS) will be updated for the introduction of<br />
the HPV vaccine. The SBVS will message HPV vaccine information to the NIR.<br />
Further information on how to record HPV vaccine information on the NIR and SBVS<br />
will be provided later in <strong>2008</strong>.<br />
How do I claim the immunisation benefit for the HPV vaccine<br />
Claiming the immunisation benefit for the HPV vaccine will be through the standard<br />
<strong>Health</strong>PAC claiming process. The immunisation benefit will be the same as that paid<br />
for other <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong> vaccines.<br />
20 <strong>2008</strong> <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong>: <strong>Health</strong> <strong>Provider</strong> Booklet
2.7 New schedule vaccine presentation and administration<br />
Vaccine Packs Cold chain Vaccine reconstitution Vaccine<br />
administration<br />
Boostrix<br />
Boostrix 10-dose box<br />
contains:<br />
10 x 1 – dose pre-filled syringes<br />
Terumo Luer needles:<br />
10 x 25G x 5/8”, 0.5 mm x<br />
16 mm<br />
10x 23G X 1”, 0.6 mm x 25 mm<br />
(Needles not attached)<br />
Box dimensions = 120 x 90 x<br />
120 mm<br />
Boostrix single dose box<br />
contains:<br />
1 x 1-dose pre-filled syringe<br />
Terumo Luer needles:<br />
1 x 25G x 5/8”, 0.5 mm x 16 mm<br />
1 x 23G x 1”, 0.6 mm x 25 mm<br />
(Needles not attached)<br />
Box dimensions = 50 x 40 x<br />
30 mm<br />
dTap vaccine should be<br />
stored between +2°C to<br />
+8°C.<br />
dTap vaccine should not<br />
be frozen. If frozen, dTap<br />
vaccine should be<br />
discarded.<br />
Upon removal from a<br />
refrigerator, the vaccine is<br />
stable for eight hours at<br />
21°C.<br />
Not required as a pre-filled<br />
syringe<br />
Each 0.5 mL dTap<br />
vaccine is administered<br />
by deep intramuscular<br />
injection to the deltoid.<br />
Infanrix®-<br />
Hexa<br />
Infanrix®-hexa box contains:<br />
10 pre-filled syringes, containing<br />
0.5 mL DTap-IPV-HepB<br />
suspension<br />
10 glass vials, containing the<br />
Hib pellet<br />
Terumo Luer needles:<br />
10 x 25G x 5/8" 0.5 mm x 16<br />
mm<br />
10 x 23G x 1" 0.6 mm x 25 mm<br />
(Needles are not attached)<br />
Box dimensions = 116 x 200 x<br />
51 mm<br />
Infanrix®-hexa vaccine<br />
should be stored between<br />
+2°C and +8°C. Protect<br />
from light.<br />
The Infanrix®-hexa<br />
suspension and the<br />
reconstituted vaccine<br />
should not be frozen.<br />
Discard if frozen.<br />
After reconstitution, the<br />
vaccine should be injected<br />
promptly. However, the<br />
vaccine may be kept for up<br />
to eight hours at room<br />
temperature (21°C).<br />
Attach the 25-gauge needle<br />
to the pre-filled syringe.<br />
Transfer the syringe’s liquid<br />
suspension to the vial<br />
containing the Hib pellet.<br />
Shake the vial well to<br />
ensure the Hib pellet is<br />
completely dissolved.<br />
Draw the reconstituted<br />
vaccine back into the<br />
syringe.<br />
Attach the 23-gauge needle<br />
to the syringe for vaccine<br />
administration.<br />
After reconstitution, the<br />
vaccine should be injected<br />
promptly.<br />
However, the vaccine may<br />
be kept for up to eight<br />
hours at room temperature<br />
(21°C).<br />
Each 0.5 mL dose of<br />
the reconstituted<br />
vaccine is given by<br />
deep intramuscular<br />
injection into the thigh.<br />
Note: Infanrix®-hexa<br />
and Prevenar®<br />
vaccines are given in<br />
separate limbs<br />
Prevenar<br />
Packs of 10 x 1-dose pre-filled<br />
syringes<br />
Box dimensions = 150 x 110 x<br />
50 mm (LxWxH)<br />
Note: Needles are not supplied<br />
with the vaccine<br />
PCV7 vaccine should be<br />
stored between +2°C and<br />
+8°C.<br />
PCV7 vaccine should not<br />
be frozen.<br />
If frozen, PCV7 vaccine<br />
should be discarded.<br />
Not required as a pre-filled<br />
syringe.<br />
Each 0.5mL PCV7 dose<br />
is given intramuscularly.<br />
The preferred injection<br />
sites are:<br />
• the anterolateral<br />
aspect of the thigh<br />
of infants and young<br />
children<br />
• the deltoid muscles<br />
of the upper arm of<br />
older children<br />
Note: Infanrix®-hexa<br />
and Prevenar®<br />
vaccines are given in<br />
separate limbs.<br />
<strong>2008</strong> <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong>: <strong>Health</strong> <strong>Provider</strong> Booklet 21
Vaccine Packs Cold chain Vaccine reconstitution Vaccine<br />
administration<br />
Gardasil®<br />
Packs of 10 x 1-dose pre-filled<br />
syringes<br />
Box dimensions = 95 x 87 x<br />
150mm<br />
Note: Needles are not supplied<br />
with the vacccine<br />
Gardasil vaccine should<br />
be stored between +2°C<br />
and +8°C.<br />
Gardasil vaccine should<br />
not be frozen.<br />
Protect Gardasil from light.<br />
Gardasil should be<br />
administered as soon as<br />
possible after being<br />
removed from<br />
refrigeration. Gardasil can<br />
be out of refrigeration at<br />
temperatures, at or below<br />
25°C, for a total time of not<br />
more than 72 hours.<br />
Not required as a pre-filled<br />
syringe<br />
Shake well before use.<br />
Thorough agitation<br />
immediately before<br />
administration is necessary<br />
to maintain suspension of<br />
the vaccine.<br />
After thorough agitation,<br />
Gardasil is a white, cloudy<br />
liquid. Parenteral drug<br />
products should be<br />
inspected visually for<br />
particulate matter and<br />
discolouration prior to<br />
administration. Discard the<br />
product of particulates are<br />
present or if it appears<br />
discoloured.<br />
Each 0.5 mL Gardasil<br />
dose should be<br />
administered<br />
intramuscularly.<br />
The preferred injection<br />
sites are:<br />
• In the deltoid region<br />
of the upper arm<br />
• In the higher<br />
anterolateral area of<br />
the thigh.<br />
22 <strong>2008</strong> <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong>: <strong>Health</strong> <strong>Provider</strong> Booklet
3 dTap (Boostrix) Vaccine and Pertussis<br />
Epidemiology<br />
3.1 dTap (Boostrix TM ) vaccine schedule<br />
From 1 January <strong>2008</strong>, 11 year olds (or school-aged year 7 students) receive one dose<br />
of the adult diphtheria, tetanus, adult acellular pertussis (dTap, Boostrix TM ) vaccine.<br />
Note: dTap vaccine is delivered as a school-based (year 7) immunisation programme in<br />
the North Island and Nelson Marlborough DHBs and by primary health care services in<br />
the remainder of the South Island.<br />
3.2 Rationale for introducing the dTap vaccine<br />
Previous schedule changes<br />
From 1 January <strong>2008</strong>, year 7 students (11 years of age) are offered dTap (Boostrix TM )<br />
vaccine. From <strong>2008</strong> (due to previous schedule changes), all 11-year-old students will<br />
have already received the recommended four doses of polio vaccine in childhood.<br />
Therefore dTap-IPV (Boostrix®-IPV) vaccine is no longer required (see the<br />
<strong>Immunisation</strong> Handbook 2006, chapter 8, page 199 (Ministry of <strong>Health</strong> 2006).<br />
3.3 Pertussis epidemiology<br />
Pertussis-containing vaccine was added to the schedule in 2006 because children at<br />
11 years of age had only received pertussis vaccine in their first year of life. These<br />
children are at risk from pertussis due to:<br />
• variable immunisation coverage<br />
• the whole-cell pertussis vaccine used before 2000 was around 80% effective after<br />
three doses<br />
• a child’s immunity wanes over time.<br />
If immunity is not boosted either with vaccine or natural infection, the population<br />
gradually becomes increasingly susceptible to pertussis infection, and eventually an<br />
epidemic occurs. In New Zealand, the most recent epidemic of pertussis was in 2004/5,<br />
see Figure 3.1. As can be seen in Figure 3.2, in 2004, older children, and many<br />
adolescents and adults developed pertussis – and they are known to have passed the<br />
pertussis infection on to babies and infants.<br />
The acellular pertussis vaccine booster (as dTap, Boostrix TM ) given at age 11 years<br />
provides protection against the disease during adolescence.<br />
<strong>2008</strong> <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong>: <strong>Health</strong> <strong>Provider</strong> Booklet 23
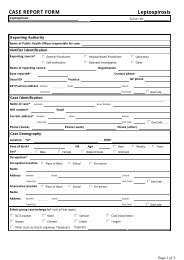
Figure 3.1: Notifications of pertussis in New Zealand (all ages), 2001–2007<br />
Pertussis notifications by month Sept 2001 to Sept 2007<br />
650<br />
600<br />
550<br />
500<br />
Number of notifications<br />
450<br />
400<br />
350<br />
300<br />
250<br />
200<br />
4th dose of<br />
pertussis vaccine<br />
at age 4 years<br />
Pertussis vaccine<br />
to 11 year olds<br />
150<br />
100<br />
50<br />
0<br />
Sep-01<br />
Dec-01<br />
Mar-02<br />
Jun-02<br />
Sep-02<br />
Dec-02<br />
Mar-03<br />
Jun-03<br />
Sep-03<br />
Dec-03<br />
Mar-04<br />
Jun-04<br />
Sep-04<br />
Dec-04<br />
Mar-05<br />
Jun-05<br />
Sep-05<br />
Dec-05<br />
Mar-06<br />
Jun-06<br />
Sep-06<br />
Dec-06<br />
Mar-07<br />
Jun-07<br />
Sep-07<br />
Month<br />
Source: ESR monthly surveillance reports<br />
http://www.surv.esr.cri.nz/surveillance/monthly_surveillance.php<br />
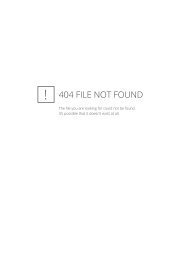
Figure 3.2: Age-specific rates of pertussis in New Zealand 2000–2006<br />
Age specific rates of pertussis notifications (expansion of Fig 6.2 page 166 Imm<br />
Handbook) http://www.surv.esr.cri.nz/surveillance/annual_surveillance.php<br />
800<br />
700<br />
600<br />
Rate per 100,000<br />
500<br />
400<br />
300<br />
200<br />
2000<br />
2004<br />
2005<br />
2006<br />
100<br />
0<br />
3.4 dTap (Boostrix TM ) vaccine information<br />
For detailed dTap (Boostrix TM ) vaccine information refer to:<br />
• the Boostrix TM data sheet (refer to the Medsafe data sheets at:<br />
http://www.medsafe.govt.nz/profs/Datasheet/dsform.asp)<br />
• the <strong>Immunisation</strong> Handbook 2006 (Ministry of <strong>Health</strong> 2006).<br />
dTap (Boostrix TM ) vaccine presentation<br />
Pack 10-dose syringe Single-dose syringe<br />
Dimensions (L x W x H) 120 x 90 x 120 mm 50 x 40 x 30 mm<br />
Contents 10 x 1-dose pre-filled syringes 1 x 1-dose pre-filled syringe<br />
Needle size<br />
(gauge and length)<br />
Needle not attached<br />
10 x Terumo Luer:<br />
25G x 5/8”, 0.5 mm x 16 mm<br />
23G X 1”, 0.6 mm x 25 mm<br />
1 s Terumo Luer<br />
25G x 5/8”, 0.5 mm x 16 mm<br />
23G x 1”, 0.6 mm x 25 mm<br />
The 10-dose packs are mainly distributed to school-based programmes. However, if a<br />
GP orders large quantities, then the 10-dose packs will be sent.<br />
Cold chain management<br />
• dTap vaccine should be stored between +2°C to +8°C.<br />
• dTap vaccine should not be frozen. If frozen, dTap vaccine should be discarded.<br />
• Upon removal from a refrigerator, the vaccine is stable for eight hours at 21°C.<br />
dTap vaccine administration<br />
Each 0.5 mL dTap vaccine is administered by deep intramuscular injection to the<br />
deltoid.<br />
dTap vaccine immunogenicity and expected efficacy<br />
Based on the results of immunogenicity studies using dTap, the likely protective effect<br />
of dTap can be inferred by comparing these results to studies of the immunogenicity of<br />
DTaP (Infanrix) and Td vaccine.<br />
Anti-diphtheria and anti-tetanus antibody titres of above 0.01 IU/mL are generally<br />
accepted to be protective against tetanus and diphtheria (Wharton & Vitek 2004). In two<br />
adolescent studies, dTap was highly immunogenic for the diphtheria and tetanus toxoid<br />
components, with all participants having post-vaccination anti-tetanus and antidiphtheria<br />
antibody titres of at least 0.1 IU/mL and 93 to100% with titres of at least 1.0<br />
IU/mL (Minh et al 1999).<br />
<strong>2008</strong> <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong>: <strong>Health</strong> <strong>Provider</strong> Booklet 25
No equivalent serological correlate of protection has been identified for pertussis.<br />
Therefore, the evaluation of the immunogenicity of the pertussis component of dTap<br />
(Boostrix TM ) is based on:<br />
• the ability of Boostrix TM to induce a response to each of the pertussis components<br />
(defined as seroconversion in initially seronegative people or a minimum of two-fold<br />
rise in antibody titre in initially seropositive people)<br />
• the immunogenicity of the pertussis components in the combined vaccine compared<br />
with the monovalent acellular pertussis vaccine in comparative studies<br />
• antibody studies compared with those obtained in infants given Infanrix (DTaP<br />
vaccine, GSK) at three, four and five months, in whom the protective efficacy of<br />
Infanrix against WHO-defined pertussis was 88.7% (95% confidence interval [CI]:<br />
76.6–94.6%) (Schmitt et al 1997).<br />
In the adolescent studies with Boostrix TM , a response of more than 92% was recorded<br />
for each of the pertussis antigens, and 97% of the adolescents were seropositive<br />
30 days after vaccination.<br />
There were no differences between the response to the pertussis components of<br />
Boostrix TM and responses to a monovalent acellular pertussis vaccine. Current expert<br />
opinion therefore suggests that the efficacy of a primary acellular pertussis vaccine can<br />
serve as basis for efficacy of that vaccine when administered as a booster to older age<br />
groups at the same or a lower dose.<br />
The duration of protection against tetanus and diphtheria after Boostrix TM is expected to<br />
be the same as after Td vaccine.<br />
There are so far few published studies of the efficacy of dTap (Boostrix TM ) in preventing<br />
pertussis in adolescent and adult age groups. However, a randomised controlled trial in<br />
the United States of dTap (Boostrix TM , GSK) and a control vaccine enrolled 2781<br />
adolescents and adults aged between 15 and 65 years. Safety, immunogenicity and<br />
efficacy were studied after a single dose of dTap or a control vaccine during a 2½-year<br />
follow-up (Ward et al 2005). During follow-up, there were nine cases of pertussis<br />
fulfilling the primary case definition in the control group and one case of pertussis in the<br />
group that received the acellular pertussis vaccine, giving an overall efficacy of 92%<br />
(95% CI 32–99%) when adjusted for the duration of illness and 89% (95% CI 19–99%)<br />
unadjusted for the duration of illness. During the two years of follow-up, the rate of<br />
pertussis in the control group was 370 cases per 100,000 person-years.<br />
A booster dose of dTap (Boostrix TM ) is expected to protect adolescents against<br />
pertussis. A booster of dTap, if given to the immediate close contacts of newborn<br />
infants, such as to parents, grandparents and health care workers, is expected to<br />
reduce exposure of pertussis to newborn infants and infants not yet adequately<br />
protected through immunisation.<br />
26 <strong>2008</strong> <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong>: <strong>Health</strong> <strong>Provider</strong> Booklet
Expected responses (ER) and adverse events following immunisation with dTap<br />
vaccine<br />
The dTap vaccine was assessed as safe and immunogenic during clinical trials. The<br />
following may be the expected local responses (ERs) following immunisation after<br />
Boostrix TM (CDC 2006):<br />
• pain in 75% of recipients, of which 2% were severe (defined as spontaneously painful<br />
and/or preventing normal everyday activities)<br />
• swelling in 21% (of which 2.5% ≥ 50 mm) at injection site<br />
• redness in 23% (of which 1.7% ≥ 50 mm).<br />
All these local ERs are greater if tetanus vaccine were received from three to less than<br />
five years previously compared with a longer gap. Other expected reactions include:<br />
• limitation of movement<br />
• headaches (in 16%; 0.7% severe)<br />
• body ache<br />
• sore joints.<br />
Expected reactions after Boostrix TM are at least equal to those expected after Td<br />
vaccination. The incidence of clinically significant adverse events after vaccination with<br />
Boostrix TM are as low as those after Td booster.<br />
Rare events after Boostrix TM , in 1/100 to 1/1000 patients, include:<br />
• pruritis<br />
• sweating<br />
• myalgia<br />
• arthrosis<br />
• hypertonia<br />
• lymphadenopathy.<br />
dTap vaccine contraindications<br />
Contraindications to dTap vaccine include: known hypersensitivity to any component of<br />
the vaccine or individuals who have shown signs of hypersensitivity after a previous<br />
administration of diphtheria, tetanus or pertussis vaccines.<br />
3.5 Other recommendations<br />
What if Tetanus-diphtheria vaccine has been given in the past two years<br />
The 11-year-old dTap vaccine should be delayed until two years after receipt of a tetanusdiphtheria<br />
vaccine (for example, Td booster after an injury). This delay in administering<br />
dTap aims to decrease the risk and severity of a local reaction at the injection site. This<br />
precaution may be waived if a pertussis epidemic is beginning and the student lives in a<br />
household with an unimmunised younger sibling or a pregnant woman.<br />
<strong>2008</strong> <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong>: <strong>Health</strong> <strong>Provider</strong> Booklet 27
If the student received a Td vaccine booster three to five years ago, dTap immunisation<br />
is recommended.<br />
School-based programmes: referral to GPs<br />
Students who have received a Td vaccine in the past two years should be referred to<br />
their GP for follow-up and recall. The dTap vaccine should be offered to these students<br />
before they reach 16 years of age.<br />
Primary care<br />
Students who have received Td in the past two years should be followed up and<br />
recalled for dTap immunisation before they reach 16 years of age.<br />
Polio vaccine history<br />
Students at age 11 years who have an unknown immunisation history for polio vaccine<br />
or who have received three or less polio vaccine doses should complete a four-dose<br />
series of IPV vaccine from their GP.<br />
Note: The polio vaccine history will not be checked in school programmes.<br />
Incomplete tetanus, diphtheria pertussis vaccination history<br />
Two doses of Td plus one of dTap are recommended, one month apart (see the<br />
<strong>Immunisation</strong> Handbook 2006, Appendix 2, pages 395–6; Ministry of <strong>Health</strong> 2006).<br />
Alternatively, three doses of dTap, one month apart, may be given, although as yet<br />
there are no studies looking at the effectiveness of Boostrix TM used in this way.<br />
See the <strong>Immunisation</strong> Handbook 2006, chapter 6, pages 171–2; Ministry of <strong>Health</strong><br />
2006) for non-funded pertussis vaccine recommendations for other groups.<br />
3.6 <strong>National</strong> <strong>Immunisation</strong> Register and School Based Vaccination<br />
System<br />
The SBVS has been updated for the use of the dTap vaccine in the Year 7 School<br />
<strong>Immunisation</strong> Programme. The SBVS will not provide information of dTap vaccine<br />
events to the NIR.<br />
In primary health care services dTap vaccine will not be recorded on the NIR because<br />
11-year-old students are not in the birth cohort registered on the NIR.<br />
28 <strong>2008</strong> <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong>: <strong>Health</strong> <strong>Provider</strong> Booklet
4 DTaP-IPV-HepB/Hib (INFANRIX ® -hexa)<br />
4.1 Early introduction of DTaP-IPV-HepB/Hib from March <strong>2008</strong><br />
Due to Hib-HepB (Comvax®) vaccine manufacturing problems, New Zealand is not able<br />
to secure further supplies of Comvax® vaccine.<br />
Stocks of Comvax® vaccine have run out, and therefore DTaP-IPV-HepB/Hib<br />
(Infanrix®-hexa) vaccine is now available.<br />
4.2 DTaP-IPV-HepB/Hib vaccine schedule – from 1 June <strong>2008</strong><br />
DTaP-IPV-HepB/Hib vaccine will replace the 2006 schedule vaccine combinations given<br />
at six weeks, three months and five months of age.<br />
The introduction of Infanrix®-hexa vaccine means there will be two injections given at<br />
six weeks and three and five months of age (Prevenar® and Infanrix®-hexa).<br />
A change of vaccine within a primary series is safe and expected to be effective.<br />
Giving alternative vaccines to the DTaP-IPV-HepB/Hib vaccine<br />
When a child has a genuine contraindication to a component of the Infanrix®-hexa<br />
vaccine, alternative vaccines (if available) may be given and the immunisation benefit<br />
claimed.<br />
4.3 Change in type of Hib vaccine<br />
Using Infanrix®-hexa vaccine changes the Hib vaccine component from Hib-PRP-OMP<br />
(polyribosylribitol phosphate outer membrane protein) to Hib-PRP-T (polyribosylribitol<br />
phosphate chemically conjugated to tetanus toxoid).<br />
Hib-PRP-OMP vaccine was previously used as a schedule vaccine because it offers<br />
protection after a single dose – as early as six weeks of age. There is a small risk that<br />
Hib disease will re-emerge with a change to Hib-PRP-T vaccine. However, the<br />
incidence of Hib disease in New Zealand has significantly declined since Hib vaccine<br />
was introduced in 1994, with 5 to 10 cases occurring every year in unimmunised or<br />
incompletely immunised children. Hib disease will be monitored carefully using the<br />
surveillance systems following the change of vaccine to Hib-PRP-T.<br />
4.4 DTaP-IPV-HepB/Hib vaccine information<br />
For detailed DTaP-IPV-HepB/Hib vaccine information, refer to the Infanrix®-hexa<br />
vaccine data sheet (refer to the Medsafe data sheets at:<br />
http://www.medsafe.govt.nz/profs/Datasheet/dsform.asp)<br />
<strong>2008</strong> <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong>: <strong>Health</strong> <strong>Provider</strong> Booklet 29
Pack and needle information<br />
The DTaP-IPV-HepB/Hib vaccine (Infanrix®-hexa) box contains:<br />
• 10 pre-filled syringes, containing 0.5 mL DTap-IPV-HepB suspension<br />
• 10 glass vials, containing the Hib pellet.<br />
Box dimensions = 116 x 200 x 51 mm (L x W x H).<br />
Brand needle size (gauge and length):<br />
• 10 x Terumo Luer 25G x 5/8” 0.5 mm x 16 mm.<br />
• 10 x Terumo Luer 23G x 1” 0.6 mm x 25 mm.<br />
Needles are not attached.<br />
Cold chain management<br />
Infanrix®-hexa vaccine should be stored between +2°C and +8°C. Protect from light.<br />
The DTap-IPV-HepB suspension and the reconstituted vaccine should not be frozen.<br />
Discard if frozen.<br />
After reconstitution, the vaccine should be injected promptly. However, the vaccine may<br />
be kept for up to eight hours at room temperature (21°C).<br />
Infanrix®-hexa vaccine reconstitution<br />
Infanrix®-hexa must be reconstituted prior to use as follows:<br />
• Attach the 25-gauge needle to the pre-filled syringe.<br />
• Transfer the syringe’s liquid suspension to the vial containing the Hib pellet.<br />
• Shake the vial well to ensure the Hib pellet is completely dissolved.<br />
• Draw the reconstituted vaccine back into the syringe.<br />
• Attach the 23-gauge needle to the syringe for vaccine administration.<br />
• After reconstitution, the vaccine should be injected promptly.<br />
• However, the vaccine may be kept for up to eight hours at room temperature (21°C).<br />
DTaP-IPV-HepB/Hib vaccine administration<br />
Each 0.5 mL dose of the reconstituted vaccine is given by deep intramuscular injection<br />
into the thigh. Infanrix®-hexa and Prevenar® vaccines are given in separate limbs.<br />
30 <strong>2008</strong> <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong>: <strong>Health</strong> <strong>Provider</strong> Booklet
DTaP-IPV-HepB/Hib vaccine efficacy<br />
Immunological data<br />
One month after a three-dose primary course of Infanrix®-hexa:<br />
• 98.5 to 100% of infants had antibody titres of ≥ 0.1 IU/mL for both tetanus and<br />
diphtheria<br />
• the response rate for each of the pertussis antigens (pertussis toxoid, filamentous<br />
haemaglutinin and pertactin) was between 97.2 and 99.3%, 95.2 and 100%, and 95.9<br />
and 99.3% respectively<br />
• there are no correlates of protection for the pertussis components. However,<br />
protective efficacy of Infanrix®-hexa may be inferred from the DTaP (Infanrix) trials<br />
where the DTaP vaccine was found to be 88.7% effective against WHO defined<br />
pertussis (21 days of typical paroxysmal cough) (German study). In an Italian study<br />
using Infanrix, an efficacy of 84% was confirmed at 60 months after completion of the<br />
primary series (Italy)<br />
• Hepatitis B component: 98.5 to 100% of infants developed protective antibody titres<br />
of ≥ 10 mIU/mL<br />
• Inactivated poliovirus (IPV) component: the seroprotection rates for each of the three<br />
serotypes (types 1, 2 and 3) were 99.2 to 100%, 94.5 to 99% and 98.8 to 100%<br />
respectively<br />
• Hib: the Geometric Mean Concentration (GMC) of antibodies ranged from 1.52 to<br />
3.53 μg/mL, with 93.5 to 100% of subjects reaching antibody titres of ≥ 0.15 μg/mL<br />
• Hib: the GMCs are lower than that elicited by the separate Hib component but are not<br />
different from those elicited by the licensed DTaP/Hib vaccine.<br />
A recent study from Germany (Kalies <strong>2008</strong>) showed there were no cases of<br />
haemophilus influenzae type b invasive disease following a four-dose hexavalent<br />
vaccine series in a five-year follow-up in Germany. The hexavalent vaccines (including<br />
Infanrix®-hexa) were highly effective 10% in this study.<br />
Post-marketing surveillance has shown that over a two-year follow-up period, the<br />
effectiveness of a three-dose primary series of DTaP/Hib or DTaP-IPV/Hib was 98.8%.<br />
Interference with other vaccines<br />
Data on concomitant administration of Infanrix®-hexa with Prevenar® have shown no<br />
clinically relevant interference in the antibody response to each of the individual<br />
antigens when given as a three-dose primary vaccination.<br />
Premature babies<br />
Limited data in 169 premature infants indicate that Infanrix®-hexa can be given to<br />
premature children. However, a lower immune response may be observed, and the<br />
level of clinical protection remains unknown.<br />
<strong>2008</strong> <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong>: <strong>Health</strong> <strong>Provider</strong> Booklet 31
Expected responses and adverse events following immunisation with DTaP-IPV-<br />
HepB/Hib vaccine<br />
In ≥ 10% of vaccine recipients:<br />
• loss of appetite<br />
• irritability<br />
• restlessness<br />
• abnormal crying<br />
• pain, redness and swelling at the injection site<br />
• fever (> 38°C)<br />
• fatigue.<br />
In ≥ 1% and < 10% of vaccine recipients:<br />
• vomiting<br />
• diarrhoea<br />
• local swelling and induration at injection site (≥ 50 mm)<br />
• fever > 39.5°C.<br />
Infanrix®-hexa and Prevenar®<br />
A higher incidence of fever (> 39.5°C) was reported in infants receiving Infanrix®-hexa<br />
and Prevenar® compared to infants receiving Infanrix®-hexa vaccine alone. 1.2% after<br />
the first dose of Infanrix®-hexa and PCV7 compared with 0.6 after Infanrix®-hexa alone.<br />
Of infants with a temperature > 39.5°C after the first dose 4.6 had received Infanrix®hexa<br />
and PCV7 compared with 1.8 with Infanrix®-hexa alone. After the third dose of<br />
Infanrix®-hexa and PCV7 2.4% had a fever > 39.5°C (Tichmann-Schumann, 2005).<br />
How to manage fever<br />
• Give the baby extra fluids to drink (more breastfeeds or water).<br />
• Do not overdress the baby if hot.<br />
• Paracetamol may be given for pain relief prior to immunisation.<br />
DTaP-IPV-HepB/Hib vaccine contraindications<br />
DTaP-IPV-HepB/Hib vaccine should not be administered to subjects with known<br />
hypersensitivity to the active substances or to any of the excipients or residuals or to<br />
subjects having shown signs of hypersensitivity after previous administration of<br />
diphtheria, tetanus, pertussis, hepatitis B, polio or Hib vaccines.<br />
DTaP-IPV-HepB/Hib vaccine is contraindicated if the child has experienced an<br />
encephalopathy of unknown aetiology, occurring within seven days following previous<br />
vaccination with pertussis containing vaccine. In these circumstances, pertussis<br />
vaccination should be discontinued and the vaccination course should be continued with<br />
diphtheria-tetanus, hepatitis B, inactivated polio and Hib vaccines.<br />
32 <strong>2008</strong> <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong>: <strong>Health</strong> <strong>Provider</strong> Booklet
4.5 DTaP-IPV-HepB/Hib vaccine and the <strong>National</strong> <strong>Immunisation</strong><br />
Register<br />
PMS and NIR upgrades for Infanrix®-hexa are expected from 1 June <strong>2008</strong>.<br />
Before 1 June <strong>2008</strong>, enter Infanrix®-hexa into the Patient Management System (PMS)<br />
as two separate vaccines (two events). Therefore:<br />
• enter Hib-HepB (or HepB) and then enter DTaP-IPV as separate events (as you<br />
currently do with the 2006 <strong>National</strong> Childhood <strong>Immunisation</strong> <strong>Schedule</strong>)<br />
• enter the same Infanrix®-hexa batch number and expiry date into both events’ batch<br />
number and expiry field.<br />
Note: Prior to 1 June <strong>2008</strong>, this will be recorded in your PMS and the NIR as if two<br />
separate vaccinations were given.<br />
From 1 June <strong>2008</strong>, the NIR will record DTaP-IPV-HepB/Hib vaccine events as part of<br />
the <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong>.<br />
4.6 DTaP-IPV-HepB/Hib vaccine and claiming the immunisation<br />
benefit<br />
<strong>Health</strong>PAC payment systems will not be updated for Infanrix®-hexa until 1 June <strong>2008</strong>.<br />
Before 1 June <strong>2008</strong>, for the six-week, three and five-months events claim as though<br />
DTaP-IPV and Hib-HepB or HepB vaccines were given, that is, record the DTaP-IPV-<br />
HepB/Hib (Infanrix®-hexa) vaccination event as if two separate vaccinations were<br />
given.<br />
From 1 June <strong>2008</strong>, <strong>Health</strong>PAC payment systems will accept claims for the DTaP-IPV-<br />
HepB/Hib (Infanrix®-hexa) vaccine.<br />
<strong>2008</strong> <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong>: <strong>Health</strong> <strong>Provider</strong> Booklet 33
5 Pneumococcal Conjugate Vaccine (PCV7,<br />
Prevenar ® ) and Pneumococcal Epidemiology<br />
5.1 PCV7 vaccine schedule – from 1 June <strong>2008</strong><br />
From 1 June <strong>2008</strong>, all new babies beginning their childhood immunisations will be<br />
offered PCV7 vaccine. These babies will receive four doses of PCV7 vaccine at the<br />
same time as other <strong>Schedule</strong> vaccines – at six weeks and three, five and 15 months of<br />
age (see the <strong>2008</strong> <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong> table in section 1).<br />
In addition, from 1 June <strong>2008</strong>, all babies born from 1 January <strong>2008</strong> are eligible to<br />
receive PCV7 vaccine. For these babies, a catch-up schedule applies – see Table 5.1<br />
below.<br />
Table 5.1: PCV7 vaccine schedule<br />
Age of baby at PCV7 dose 1<br />
PCV7 vaccine schedule<br />
6 weeks to 6 months 6 weeks, 3 months, 5 months, 15 months of age three doses 6 to 8<br />
weeks apart + one dose at age 15 months<br />
7 months to 11 months of age* Two doses 6 weeks apart + one dose at age 15 months<br />
12 to 23 months* Two doses of PCV7 given 6 to 8 weeks apart<br />
* Applies only to babies born from 1 January <strong>2008</strong>.<br />
5.2 Pneumococcal disease<br />
Streptococcus pneumoniae (pneumococcus) is a lance shaped gram-positive<br />
diplococcus. It is ubiquitous, with many asymptomatic individuals carrying the organism<br />
in the upper respiratory tract.<br />
There are some 90 identifiable serotypes of S. pneumoniae. Some, more commonly<br />
affect children, while others are of greater significance in adults.<br />
Transmission of the pneumococcus is from person to person, usually by droplet contact.<br />
The emergence of antibiotic-resistant strains of S. pneumoniae has become an<br />
increasing concern both in New Zealand and internationally for the management of IPD.<br />
ESR analysis of S. pneumoniae isolates from invasive pneumococcal disease (IPD) in<br />
2004 found that 16.4% of isolates were resistant to penicillin, and 12.1% were resistant<br />
to cefotaxime. Ninety-eight percent of penicillin-resistant serotypes and 94% of the<br />
serotypes resistant to third-generation cephalosporins would be covered by the PCV7<br />
vaccine (Heffernan et al 2006). This suggests that introduction of the PCV7 vaccine will<br />
reduce disease caused by antibiotic resistant S. pneumoniae isolates.<br />
The spectrum of disease caused by pneumococcal bacteria<br />
Pneumococcal disease can cause otitis media at the mildest (but most frequent) end of<br />
the disease spectrum and pneumococcal meningitis and death at the most severe (but<br />
34 <strong>2008</strong> <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong>: <strong>Health</strong> <strong>Provider</strong> Booklet
less frequent) end of the spectrum (see Figure 5.1). PCV7 vaccine is most effective<br />
against severe pneumococcal disease.<br />
Figure 5.1: Pneumococcal disease spectrum (for use as a guide only)<br />
Disease frequency<br />
Otitis media<br />
Pneumococcal<br />
pneumonia<br />
Pneumococcal<br />
bacteraemia<br />
Pneumococcal<br />
meningitis<br />
PCV 7<br />
effect on<br />
disease<br />
Increasing disease severity<br />
Increasing PCV7 vaccine effectiveness<br />
against disease<br />
The pneumococcus may also cause endocarditis, and, less commonly, sites such as<br />
joints, the peritoneal cavity and the fallopian tubes are affected.<br />
IPD is defined as isolation of Streptococcus pneumoniae from a normally sterile site,<br />
usually blood or cerebrospinal fluid (CSF) but also from pleural tissue or other sterile<br />
sites. The major clinical syndromes of IPD include pneumonia with bacteraemia,<br />
meningitis and bacteraemia without focus.<br />
Non-invasive pneumococcal diseases include otitis media, sinusitis and (nonbacteraemic)<br />
pneumonia.<br />
The incubation period of S. pneumoniae infection is variable but may be as short as one<br />
to three days. Illness usually occurs within one month of acquiring a new serotype in<br />
the upper respiratory tract and does not usually result in prolonged carriage of the<br />
organism.<br />
See the <strong>Immunisation</strong> Handbook 2006, chapter 16: Pneumococcal Disease for more<br />
information (Ministry of <strong>Health</strong> 2006).<br />
<strong>2008</strong> <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong>: <strong>Health</strong> <strong>Provider</strong> Booklet 35
5.3 Epidemiology<br />
Pneumococcal disease occurs throughout the year but is more common in the autumn<br />
and winter months (Kelly et al 2007).<br />
The risk of IPD is much higher in infants and elderly people and more frequent in<br />
individuals with predisposing conditions such as viral upper respiratory tract infections<br />
or underlying conditions such as immune deficiency states. Mortality is highest in<br />
patients with underlying medical conditions.<br />
These conditions include:<br />
• congenital or acquired immune deficiency<br />
• splenic dysfunction or asplenia<br />
• sickle cell anaemia<br />
• Hodgkin’s disease<br />
• human immunodeficiency virus (HIV) infection<br />
• cochlear implants or intracranial shunts<br />
• chronic cerebrospinal fluid leaks<br />
• following organ transplantation.<br />
Other conditions/factors that increase the risk of pneumococcal infection include:<br />
• diabetes mellitus<br />
• congestive heart failure<br />
• chronic pulmonary disease<br />
• renal failure<br />
• pre-term infants<br />
• children attending early childhood services<br />
• Māori and Pacific children.<br />
Patients with CSF leakage due to a fracture at the base of the skull or following a<br />
neurosurgical procedure are at risk of recurrent pneumococcal meningitis.<br />
New Zealand epidemiology<br />
ESR serotyping and antibiotic resistance testing<br />
Pneumococcal invasive disease caused by S. pneumoniae is monitored in New Zealand<br />
through ESR testing of laboratory isolates from cases of invasive disease. All<br />
laboratories send isolates of S. pneumoniae from cases of IPD, that is blood, CSF and<br />
isolates from other usually sterile sites, to ESR for serotyping and antibiotic resistance<br />
testing. It is thought that almost all isolates are sent to ESR, but this will be confirmed<br />
with laboratories in <strong>2008</strong>.<br />
In 2006, ESR received 151 isolates from children under the age of five years with IPD,<br />
and 126 (83.44%) of these were serotypes found in the seven-valent conjugate vaccine<br />
(PCV7).<br />
36 <strong>2008</strong> <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong>: <strong>Health</strong> <strong>Provider</strong> Booklet
New Zealand <strong>Health</strong> Information Service data on hospitalisations<br />
Information is also available from the New Zealand <strong>Health</strong> Information Service (NZHIS)<br />
on hospitalisations for pneumococcal infections associated with meningitis and<br />
septicaemia. However, this information is likely to underestimate the burden of disease<br />
caused by IPD infection because of how the illness is coded on discharge.<br />
From the NZHIS data, Figure 5.2 shows the number of cases from 1999 to 2006<br />
hospitalised with pneumococcal meningitis in children under the age of two years, and<br />
Figure 5.3 shows the number of children hospitalised with pneumococcal septicaemia.<br />
Figure 5.2: Hospitalisations from pneumococcal meningitis in children under two years of age,<br />
1999–2006<br />
Number of cases<br />
40<br />
35<br />
30<br />
25<br />
20<br />
15<br />
10<br />
5<br />
0<br />
1999/00 2000/01 2001/2 2002/3 2003/4 2004/5 2005/6<br />
Year<br />
under 12 months<br />
12–23 months<br />
Source: NZHIS.<br />
<strong>2008</strong> <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong>: <strong>Health</strong> <strong>Provider</strong> Booklet 37
Figure 5.3: Hospitalisations from pneumococcal septicaemia in children under two years of<br />
age, 1999–2006<br />
16<br />
14<br />
12<br />
Number<br />
10<br />
8<br />
6<br />
4<br />
2<br />
0<br />
1999/00 2000/01 2001/2 2002/3 2003/4 2004/5 2005/6<br />
Year<br />
septicaemia under 12 months<br />
septicaemia 12–23 months<br />
Source: NZHIS.<br />
New Zealand Paediatric Surveillance Unit study<br />
A two-year study took place, from May 2005 until April 2007, through the New Zealand<br />
Paediatric Surveillance Unit to monitor the number of children under 15 years of age<br />
diagnosed with pneumococcal meningitis (Lennon and Webb 2007).<br />
During the study period, 38 children were identified who fitted the case definition of<br />
confirmed pneumococcal meningitis with either a bacterial culture (34 cases) or PCR<br />
analysis (four cases), a national incidence rate of 2.2 cases per 100,000 per year in<br />
children under the age of 15 years.<br />
Of the 38 children with confirmed pneumococcal meningitis:<br />
• 28 (73.7%) were males<br />
• 33 (86.8%) were children under 24 months of age, an age-specific rate of 15.7 cases<br />
per 100,000 per year in children under the age of two years<br />
• 28 (73.7%) came from the four DHBs of: Auckland, Counties Manukau, Capital and<br />
Coast, and Canterbury<br />
• four died from pneumococcal meningitis, a case fatality rate of 10.5%<br />
• six (17.6%) suffered from a persisting neurodisability.<br />
38 <strong>2008</strong> <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong>: <strong>Health</strong> <strong>Provider</strong> Booklet
Of the 33 children under the age of two years with pneumococcal meningitis:<br />
• 10 were babies aged 0–6 months<br />
• 13 were infants aged 6–11 months<br />
• 10 were young children aged 12–23 months<br />
• 13 were Māori; an annual Māori age-specific rate of 23.6 per 100,000 per year<br />
• seven were Pacific children; an age and ethnicity specific rate of 39.2 per 100,000<br />
year<br />
• 13 were of other ethnicities; a rate of 13.6 per 100,000 per year.<br />
Hearing impairment following pneumococcal meningitis was reported in nine children<br />
out of the 30 where audiology results were available.<br />
The serotype of S. pneumoniae was identified for 31 of 34 culture positive cases. Of<br />
these, 25 of 31 (80.6%) were of the serotypes contained in the PCV7 vaccine.<br />
Information on antimicrobial sensitivity was available for the culture positive cases, and<br />
of these, eight isolates showed reduced penicillin susceptibility, (Minimum Inhibitory<br />
Concentration (MIC) to penicillin ≥ 0.06 mg/L). In addition, four of the isolates with<br />
reduced penicillin susceptibility also demonstrated reduced susceptibility to third<br />
generation cephalosporins (MIC ≥ 0.5 mg/L).<br />
Monitoring the effect of PCV7 vaccine<br />
Following introduction of PCV7 vaccine onto the New Zealand Childhood <strong>Immunisation</strong><br />
<strong>Schedule</strong>, ongoing monitoring of IPD in all age groups will be essential to monitor for<br />
changes in disease serotypes and antimicrobial sensitivity.<br />
It is expected that IPD will be added to the list of infectious diseases to be notified by<br />
medical practitioners and by laboratories before the vaccine programme starts in June<br />
<strong>2008</strong>.<br />
5.4 Effects of introducing pneumococcal vaccine onto the infant<br />
immunisation programme<br />
Pneumococcal conjugate vaccine has been included on the immunisation schedules of<br />
over 14 countries, including the United States, the United Kingdom, Canada and<br />
Australia.<br />
Decline in severe pneumococcal disease incidence in young children and effect<br />
on invasive pneumococcal disease rates in older age groups<br />
Introduction of PCV7 vaccine to the United States infant immunisation schedule has<br />
resulted in a decline in severe pneumococcal disease incidence in young children and a<br />
decline in invasive pneumococcal disease (IPD) in unimmunised adults.<br />
<strong>2008</strong> <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong>: <strong>Health</strong> <strong>Provider</strong> Booklet 39
Figure 5.4: Rate of vaccine-type (VT) invasive pneumococcal disease (IPD) before and after<br />
introduction of pneumococcal conjugate vaccine (PCV7), by age group and year;<br />
Active Bacterial Core surveillance, United States, 1998–2003<br />
Source: http://www.cdc.gov/mmwr/PDF/wk/mm5436.pdf<br />
Notes:<br />
* Per 100,000 population.<br />
† For each age group, the decrease in VT IPD rate for 2003 compared with the 1998–1999 baseline is<br />
statistically significant (p
Follow-up reports from the United States Centers for Disease Control and Prevention<br />
(CDC) Active Bacterial Core surveillance estimated that, in 2005, the rates of IPD were<br />
77% lower in children aged under five years compared with 1998/99. This means there<br />
were 13,000 fewer cases of IPD during 2005 (Reingold et al <strong>2008</strong>). Since the vaccine’s<br />
introduction, there has been a shift in IPD serotypes in children aged under five years,<br />
with only 7% of disease caused by PCV7 serotypes in 2005 compared with 80% during<br />
1998/99. Serotype 19A was the most common serotype causing IPD among children in<br />
2005, and the increase in non-vaccine serotypes is estimated to be small compared<br />
with the overall decrease in PCV7 serotype IPD.<br />
A review of data reports that the herd effect of immunising children aged 2–23 months<br />
resulted in decreased IPD in infants too young to be immunised or who had only<br />
received one dose (Center 2007). In those aged 0–90 days, all IPD decreased from<br />
11.8/100,000 live births to 7.2/100,000; and rates of vaccine serotype IPD decreased<br />
significantly from 7.3/100,000 live births to 2.4.100,000 (p < 0.001). In the United States<br />
prior to PCV7 introduction, IPD was higher in blacks, however, the rates are now<br />
similar, and the disparity has been reduced.<br />
In Australia, Prevenar® was introduced for Aboriginal children in 2001, and by 2004, the<br />
incidence of IPD in Aboriginal children less than two years of age was 91.5 per 100,000,<br />
compared with 219.2 cases of IPD per 100,000 children in 2001 (Center 2007).<br />
PCV7 vaccine effects on incidence of otitis media<br />
The conjugate pneumococcal vaccine is recommended to protect against IPD.<br />
However, S. pneumoniae is the most common bacterial cause of otitis media in<br />
children, and therefore, the PCV7 vaccine studies have examined whether the vaccine<br />
has any effect on the incidence of otitis media.<br />
Finnish study<br />
In a Finnish study by Eskola et al (2001), children were followed up between 6.5 and<br />
24 months of age for episodes of otitis media after receiving heptavalent pneumococcal<br />
conjugate vaccine at two, four, six and 12 months of age. It was estimated that the<br />
vaccine reduced the incidence of acute otitis media from any cause by 6% (95% CI: -4<br />
to 16%), and of culture-confirmed pneumococcal episodes by 34% (95% CI: 21 to 45%).<br />
The incidence of acute otitis media from vaccine serotypes was reduced by 57% (95%<br />
CI: 44 to 67%), and there was a 51% reduction in episodes of vaccine related/crossreactive<br />
serotype otitis media. Significant efficacy was shown against vaccine<br />
serotypes 6B, 14 and 23F, whereas efficacy against otitis caused by 19F was poorer.<br />
However, there was an increase of 33% in the number of episodes due to all other<br />
serotypes (non-vaccine and non-related serotypes).<br />
Kaiser Permanente trial<br />
Infants participating in the Kaiser Permanente PCV7 vaccine trial from 1995–1998 were<br />
followed up to 3.5 years post trial (Fireman et al 2003). The 37,868 infants enrolled in<br />
<strong>2008</strong> <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong>: <strong>Health</strong> <strong>Provider</strong> Booklet 41
the double blind trial received either PCV7 vaccine or a control vaccine at two, four and<br />
six months of age, plus a booster at age 12–15 months. Follow-up continued until April<br />
1999, when the study was unblended and the control group children received PCV7<br />
vaccine.<br />
The clinical records of all children were assessed for episodes of otitis media, and after<br />
adjustment of rates of otitis visits for age and season, the effect of PCV7 vaccine was<br />
assessed.<br />
Control children had an average of 1.8 otitis visits per year. Children who received<br />
PCV7 vaccine had:<br />
• a 7.8% (95% CI: 5.4 to 10.1%) reduction in otitis visits<br />
• a 5.4% reduction in antibiotic prescriptions.<br />
Overall, PCV7 vaccine reduced the risk of tympanostomy tubes by 24%.<br />
In the control group, the otitis visits peaked at age 8 to 12 months, and visits were 17%<br />
higher in boys and 50% higher in the influenza season.<br />
Recurrent otitis media<br />
A study of 383 children aged one to seven years examined whether PCV7 vaccine<br />
followed by pneumococcal polysaccharide vaccine was effective in preventing otitis<br />
media in children who had had two or more episodes of otitis media in the two years<br />
before entry to the study (Veenhoven 2003). The median length of follow-up post<br />
vaccination was 18 months.<br />
Results showed no reduction in the number of episodes of acute otitis media in the<br />
pneumococcal vaccine group compared with controls. Although the nasopharyngeal<br />
carriage of pneumococci of vaccine serotypes decreased, there was an increase in the<br />
nasopharyngeal carriage of non-vaccine serotypes.<br />
Pneumococcal conjugate vaccine is not effective in reducing otitis media in young<br />
children with a history of previous otitis media who receive vaccine at ages greater than<br />
one year.<br />
Effects of the pneumococcal conjugate vaccine on the prevention of pneumonia<br />
Streptococcus pneumoniae is a common cause of bacterial pneumonia associated with<br />
both bacteraemia-invasive pneumococcal disease and pneumonia without bacteraemia.<br />
In order to look at the effect of PCV7 on the incidence of pneumonia, following<br />
development of a WHO standard for interpretation of chest radiographs, the X-rays from<br />
children developing pneumonia who participated in the Kaiser Permanente study were<br />
reviewed (Hansen et al 2006).<br />
In this study, the efficacy of PCV7 vaccine against first-episode radiograph-confirmed<br />
pneumonia, calculated by trial radiologists, was 17.7% in the intent-to-treat group and<br />
20.5% in the per protocol (95% CI: 4.4 to 34%).<br />
42 <strong>2008</strong> <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong>: <strong>Health</strong> <strong>Provider</strong> Booklet
Using the WHO standard, the efficacy against first-episode radiograph-confirmed<br />
pneumonia was 25.5% for the intent-to-treat group and 30.3% (95% CI: 10.7 to 45.7%)<br />
for per protocol.<br />
Serotype replacement<br />
Long-term surveillance is necessary to monitor any changes in the Streptococcus<br />
pneumoniae serotypes following introduction of conjugate pneumococcal vaccine to<br />
infants.<br />
Surveillance results suggest some serotype replacement occurs three years after the<br />
introduction of PCV7 vaccine to infants. Therefore surveillance and the development of<br />
expanded valency vaccines are important. Some of the increase in 19A and other nonvaccine<br />
serotypes (NVT) may be due to serotype switching within certain vaccine<br />
strains.<br />
Massachusetts study<br />
In Massachusetts, after PCV7 was introduced, IPD due to NVT increased from 73.7% of<br />
all cases in children under the age of five years in 2001 to 90.6% in 2005 (Hsu et al<br />
2005).<br />
As has been noted in other studies, the number and proportion of NVT serotype 19A<br />
increased over time. In Massachusetts from 2002 to 2005, overall 19A was found in<br />
27% of all IPD in children under the age of five years but had increased in 2005 to be<br />
found in 44% of cases of IPD.<br />
However, the number of cases of IPD due to 19F, a vaccine serotype, remained stable.<br />
Examination of the 19A isolates by multilocus sequence typing (MLST) showed that the<br />
diversity of the 19A types increased over time from five MLST types in 2001/02 to<br />
11 MLST types in 2004/05. Cross protection of the vaccine 19F type for the 19A<br />
appears to be limited.<br />
From 2002 to 2004, the majority of isolates of 19A demonstrated intermediate sensitivity<br />
to penicillin and full sensitivity to ceftriaxone and amoxicillin. However, in 2005 a small<br />
number of isolates of 19A were multi-drug resistant and of a sequence type not<br />
previously identified in Massachusetts.<br />
Alaskan study<br />
A study among Alaskan native children (Singleton et al 2007) showed that in the first<br />
three years after PCV7 was introduced, the rate of IPD in children younger than two<br />
years of age fell from 403.2 per 100,000 between 1995 and 2000 to 134.3 per 100,000<br />
per year between 2001 and 2003.<br />
However, from 2001 to 2006, the rate of IPD in Alaskan native children increased to<br />
244.6 per 100,000 in children under the age of two years, an increase of 82%, mainly<br />
because of the increase in NVT.<br />
<strong>2008</strong> <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong>: <strong>Health</strong> <strong>Provider</strong> Booklet 43
Since 2004, the NVT serotypes have increased by 140%. The NVT rate between 1995<br />
and 2000 in children under two years of age was 95 per 100,000 and 228.6 between<br />
2004 and 2006. In the same time period, disease due to the vaccine serotypes has<br />
decreased by 96%, compared with the prevaccine period.<br />
IPD due to serotype 19A was found in 28.3% of IPD in Alaskan native children under<br />
two years of age during the period 2004 to 2006. There was no increase in NVT in nonnative<br />
Alaskan children.<br />
Increase in disease was accompanied by an increase in nasopharyngeal colonisation<br />
with NVT over this time. In particular, 19A increased in all age groups from 0.5% of<br />
colonised persons in the period 1998 to 2000 to 3% in 2003 and 15% in 2004. Overall<br />
41% of all persons were colonised with Streptococcus pneumoniae in 2004.<br />
Effects of introducing PCV7 on nasopharyngeal carriage of pneumococci and<br />
disease due to antibiotic resistant serotypes<br />
In the Alaskan study discussed above, the researchers looked for any change in<br />
disease presentation with the changes to NVT disease. The illnesses among Alaskan<br />
native children due to IPD NVT replacement were similar to IPD cases before PCV7<br />
introduction, except for an increase in the proportion of hospitalised IPD, pneumonia<br />
and empyema.<br />
An increase in empyema associated particularly with serotype 1 has been reported in<br />
other studies, but this type was not found in any of the Alaskan native children under the<br />
age of two years (Singleton et al 2007).<br />
In France, after the introduction of PCV7 onto the routine infant schedule, a study<br />
examined the nasopharyngeal carriage of pneumococci in children age six to 24 months<br />
presenting with acute otitis media (AOM) (Cohen et al 2006).<br />
Over the three years of the study, the proportion of infants receiving one or more doses<br />
of PCV7 increased from 8.2% in year 1 to 61.4% in year 3. The proportion of children<br />
who had received antibiotics in the three months before enrolment in the study<br />
decreased from 51.8% in year 1 to 40.9% in year 3.<br />
Overall, pneumococcal carriage and carriage of PCV7 serotypes decreased over the<br />
three-year period by 16% (p < 0.001). However, there was an increase in non-vaccine<br />
serotypes from 9.6% in year 1 to 15.8% of children in year 3. In addition, the rates of<br />
highly penicillin resistant strains of pneumococci decreased each year from 15.4% in<br />
year 1 to 10.6% in year 2 and 6.7% in year 3.<br />
Children who had received PCV7 vaccine and had not received antibiotics in the three<br />
months before they presented with AOM had the lowest rate of penicillin resistant<br />
strains. In France, implementation of PCV7 vaccine together with a planned reduction<br />
in antibiotic use had an impact of reducing the carriage of penicillin non-susceptible<br />
pneumococci.<br />
44 <strong>2008</strong> <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong>: <strong>Health</strong> <strong>Provider</strong> Booklet
5.5 Immunogenicity and efficacy of pneumococcal conjugate<br />
vaccine<br />
See also the <strong>Immunisation</strong> Handbook 2006, chapter 16, page 316 (Ministry of <strong>Health</strong><br />
2006).<br />
Polysaccharide vaccines are poorly immunogenic in children under the age of two years<br />
because the polysaccharide antigens are T cell-independent.<br />
Covalent coupling of a polysaccharide antigen to an immunogenic protein carrier<br />
converts the polysaccharide to a T cell-dependent antigen. Conversion to a T celldependent<br />
antigen enhances the antibody response and elicits immune memory and<br />
stronger booster responses on re-exposure in infants and young children.<br />
Prevenar®, a 7-valent conjugate pneumococcal vaccine uses CRM 197 , a mutant nontoxic<br />
diphtheria toxin , as the carrier protein. Prevenar® contains the purified<br />
polysaccharides of the capsular antigens of seven Streptococcus pneumoniae<br />
serotypes (4, 9V, 14, 18C, 19F, 23F and 6B) individually conjugated to CRM 197 .<br />
The minimum titre of circulating antibody necessary for protection against IPD and otitis<br />
media has not been determined for any particular serotype. In the Kaiser Permanente<br />
trial (Black et al 2000), over 97% of PCV7 recipients achieved antibody levels of<br />
≥ 0.15 mg/mL for all serotypes after a three-dose primary series (at two, four and six<br />
months of age), and this correlated with the observed protective efficacy against IPD of<br />
97%.<br />
The serum antibody responses to some of the conjugate vaccine types are substantial<br />
after one or two doses, whereas others require completion of three doses. Three doses<br />
of conjugate vaccine in infants induced functional antibodies and a strong, rapid<br />
anamnestic response on boosting with conjugate or polysaccharide vaccine six to<br />
12 months after the primary series (<strong>National</strong> Advisory Committee on <strong>Immunisation</strong><br />
2002).<br />
Efficacy of Prevenar® in special groups<br />
Children with HIV infection<br />
Infants and young children with HIV infection are at greater risk of IPD than children<br />
without HIV infection.<br />
In a randomised controlled trial, 30 infants with HIV infection, aged 56 to 180 days at<br />
entry, received PCV7 vaccine at weeks zero, eight and 16 after enrolment, and<br />
15 infants in the control group received a placebo. Few infants were receiving<br />
antiretroviral therapy at the beginning of the study (Nachman et al 2003).<br />
The safety was monitored and the children followed until the age of two years. The<br />
vaccine was well tolerated, although more severe local reactions were seen in children<br />
who were symptomatic due to HIV infection. The PCV7 vaccine was immunogenic in all<br />
infants receiving PCV7 vaccine, although longevity of the immune response and the<br />
efficacy of the vaccine could not be measured in this small study.<br />
<strong>2008</strong> <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong>: <strong>Health</strong> <strong>Provider</strong> Booklet 45
Low birth weight and pre-term infants<br />
In the Kaiser Permanente trial, a large randomised controlled trial of 37,868 infants,<br />
there were 1756 low birth weight (LBW) infants, under 2500 gm, including three with<br />
birth weights under 750 gm (Shinefield et al 2002). There were also 4340 pre-term<br />
infants (PT) born at gestation 32 to < 38 weeks.<br />
The LBW and PT infants were randomised and received either PCV7 or<br />
meningococcal C conjugate vaccine. The vaccine course was started at the time the<br />
infant was discharged home.<br />
In both LBW and PT infants, the PCV7 vaccine was well tolerated, safe and<br />
immunogenic.<br />
5.6 PCV7 vaccine information<br />
For further PCV7 vaccine information, refer to:<br />
• the Prevenar® data sheet (refer to the Medsafe data sheets at:<br />
http://www.medsafe.govt.nz/profs/Datasheet/dsform.asp)<br />
• the <strong>Immunisation</strong> Handbook 2006 (Ministry of <strong>Health</strong> 2006).<br />
PCV7 vaccine presentation<br />
• Pack dimensions = 150 x 110 x 50 mm (L x W x H).<br />
• Packs of 10 x 1-dose pre-filled syringes.<br />
• Needles are not supplied with the vaccine.<br />
Cold chain management<br />
• PCV7 vaccine should be stored between +2°C and +8°C.<br />
• PCV7 vaccine should not be frozen. If frozen, PCV7 vaccine should be discarded.<br />
PCV7 vaccine administration<br />
Each 0.5 mL PCV7 dose is given intramuscularly. The preferred injection sites are:<br />
• the anterolateral aspect of the thigh of infants and young children<br />
• the deltoid muscle of the upper arm of older children.<br />
Prevenar® and Infanrix®-hexa vaccines are administered in separate limbs.<br />
PCV7 vaccine efficacy<br />
See section 5.5.<br />
46 <strong>2008</strong> <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong>: <strong>Health</strong> <strong>Provider</strong> Booklet
Expected responses and adverse events following immunisation with PCV7<br />
vaccine<br />
Local reactions (redness and swelling). In trials 10% of children had erythema after<br />
PCV7 (refer to the <strong>Immunisation</strong> Handbook 2006 page 328).<br />
Rare events (≥ 0.01% and < 0.1%) include:<br />
• febrile seizures<br />
• hypotonic, hyporesponsive episodes.<br />
Very rare events (< 0.01%) include:<br />
• urticaria<br />
• angioneurotis oedema<br />
• erythema multiforme<br />
• hypersensitivity, including anaphylaxis.<br />
Infanrix®-hexa and Prevenar®<br />
A higher incidence of fever (> 39.5°C) was reported in infants receiving Infanrix®-hexa<br />
and Prevenar® compared to infants receiving Infanrix®-hexa vaccine alone. See<br />
section 4.4 for more information.<br />
How to manage fever<br />
• Give the baby extra fluids to drink (more breastfeeds or water).<br />
• Do not overdress the baby if hot.<br />
• Paracetamol may be given for pain relief prior to immunisation.<br />
Interference with other vaccines<br />
Data on concomitant administration of Infanrix®-hexa with Prevenar® have shown no<br />
clinically relevant interference in the antibody response to each of the individual<br />
antigens when given as a three-dose primary vaccination.<br />
Avoid giving MeNZB TM vaccine at same visit as PCV7 (Prevenar®)<br />
While no problems are anticipated, either in the immune response or safety, there is no<br />
data to support giving the MeNZB TM vaccine at the same practice visit as Prevenar®.<br />
Therefore, where parents are anxious for their child to receive the MeNZB vaccine<br />
and the doctor agrees, a three-dose course of the MeNZB vaccine could start at six<br />
months of age (doses six weeks apart).<br />
See section 2.4 for more information on the eligibility for the MeNZB vaccine from<br />
1 June <strong>2008</strong>.<br />
PCV7 vaccine contraindications<br />
Contraindications include:<br />
<strong>2008</strong> <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong>: <strong>Health</strong> <strong>Provider</strong> Booklet 47
• hypersensitivity to any component of the PCV7 vaccine, including diphtheria toxoid<br />
• allergic reaction or anaphylactoid reaction following prior administration of PCV7<br />
vaccine.<br />
5.7 PCV7 vaccine and the <strong>National</strong> <strong>Immunisation</strong> Register – <strong>National</strong><br />
<strong>Immunisation</strong> <strong>Schedule</strong> only<br />
From 1 June <strong>2008</strong>, the NIR will record PCV7 vaccine events as part of the <strong>National</strong><br />
<strong>Immunisation</strong> <strong>Schedule</strong> for:<br />
• new babies beginning their immunisations<br />
• babies born from 1 January <strong>2008</strong> on a catch-up schedule.<br />
Note: The information above does not apply to children receiving PCV7 vaccine as part<br />
of the high-risk pneumococcal or pre/post-splenectomy programmes (see section 6 and<br />
Appendix 2). Information for the high risk pneumococcal or pre/post splenectomy<br />
programmes is recorded on the NIR as the ‘Pneumococcal’ programme.<br />
5.8 PCV7 vaccine and claiming the immunisation benefit –<br />
Childhood <strong>Immunisation</strong> <strong>Schedule</strong> only<br />
Note: The following does not apply to babies or children receiving PCV7 vaccine as part<br />
of the high-risk pneumococcal programme.<br />
• Vaccine administration date – from 1 June <strong>2008</strong>.<br />
• <strong>Immunisation</strong> benefit claims for PCV7 given as a schedule vaccine will be valid if the<br />
vaccine is administered from 1 June <strong>2008</strong>.<br />
• <strong>Immunisation</strong> benefit claims for the PCV7 as a schedule vaccine will be rejected if the<br />
vaccine is administered before 1 June <strong>2008</strong>.<br />
• <strong>Immunisation</strong> benefits for PCV7 as a schedule vaccine are valid for babies with a<br />
birth date from 1 January <strong>2008</strong>. <strong>Immunisation</strong> benefit claims for PCV7 as a schedule<br />
vaccine will be rejected if the vaccine is administered to babies with a birth date<br />
before 1 January <strong>2008</strong>.<br />
48 <strong>2008</strong> <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong>: <strong>Health</strong> <strong>Provider</strong> Booklet
6 Expansion of the High Risk Pneumococcal<br />
Programme for Children under Five Years of Age<br />
with a Chronic Condition<br />
6.1 Addition of new eligible groups<br />
From 1 June <strong>2008</strong>, the high-risk pneumococcal programme will be expanded to include<br />
funding for children under five years with the following chronic conditions:<br />
• pre-term infants, born at under 28 weeks gestation<br />
• chronic pulmonary disease<br />
• cardiac disease with cyanosis or failure<br />
• insulin dependant diabetes<br />
• Down’s syndrome.<br />
Table 6.1 below shows the eligibility criteria for the high-risk pneumococcal programme<br />
for children under five years of age from 1 June <strong>2008</strong>.<br />
Table 6.1: Eligibility criteria for high-risk pneumococcal programme<br />
Children aged under five years with the following conditions:<br />
On immunosuppressive or radiation<br />
therapy<br />
Primary immune deficiencies<br />
HIV<br />
Renal failure or nephrotic syndrome<br />
Organ transplants<br />
Cochlear implants or intracranial<br />
shunts<br />
With chronic CSF leaks<br />
On corticosteroid therapy for more than two weeks, at daily<br />
dose of prednisone of 2 mg/kg or greater, or a total daily<br />
dosage of 20 mg or more<br />
Children pre or post splenectomy or with functional asplenia*<br />
Pre-term infants, born at under 28 weeks’ gestation<br />
Chronic pulmonary disease (including asthma treated with<br />
high-dose corticosteroid therapy)<br />
Cardiac disease with cyanosis or failure<br />
Insulin dependent diabetes<br />
Down’s syndrome<br />
* See Appendix 2 – Pre/post Splenectomy <strong>Immunisation</strong> Programme.<br />
Note: See bold text for the additional funded chronic conditions from 1 June <strong>2008</strong>.<br />
6.2 High risk pneumococcal programme immunisation schedule<br />
Children who meet the criteria are eligible for:<br />
• PCV7 (pneumococcal conjugate, Prevenar®) vaccine<br />
• 23PPV (pneumococcal polysaccharide, Pneumovax®23) vaccine.<br />
See Table 6.2 below (reproduced from the <strong>Immunisation</strong> Handbook 2006: Table 16.6,<br />
page 325; Ministry of <strong>Health</strong> 2006) for the high-risk pneumococcal programme<br />
immunisation schedule.<br />
<strong>2008</strong> <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong>: <strong>Health</strong> <strong>Provider</strong> Booklet 49
Table 6.2: <strong>Schedule</strong> for pneumococcal vaccines for children at higher risk of pneumococcal<br />
disease with no prior history of pneumococcal vaccines<br />
Age of child at start<br />
of course<br />
Conjugate pneumococcal vaccine<br />
(PCV7)<br />
Polysaccharide pneumococcal<br />
vaccine (23PPV)<br />
6 weeks to 6 months Three doses PCV7 at least 6–8 weeks<br />
apart, or at same time as the usual<br />
schedule; plus a fourth dose at age<br />
15 months<br />
7–11 months Two doses of PCV7 at least 6–8<br />
weeks apart; plus a third dose at age<br />
15 months<br />
12–59 months Two doses of PCV7 given at 6–8<br />
weeks apart<br />
One dose of 23PPV at age 2 years<br />
and a second dose at age 4–5 years<br />
One dose of 23PPV at age 2 years<br />
and a second dose at age 4–5 years<br />
One dose of 23PPV at age 2 years<br />
and a second dose at age 4–5 years<br />
Older children up to<br />
the age of 16 years<br />
in high risk groups*<br />
One dose of PCV7<br />
One dose of 23PPV 6–8 weeks after<br />
PCV7<br />
Note: Prevenar® is approved by Medsafe only for children up to nine years of age. If a specialist<br />
recommends Prevenar® for older children, informed consent should be obtained.<br />
Catch-up schedules for children who have already received one or more doses of<br />
pneumococcal vaccine are found in Appendix 1.<br />
For children pre or post splenectomy or with functional asplenia, see Appendix 2:<br />
Pre/post Splenectomy <strong>Immunisation</strong> Programme, and for vaccine dosage, see the<br />
<strong>Immunisation</strong> Handbook 2006: Table 16.5, page 323 (Ministry of <strong>Health</strong> 2006).<br />
6.3 Entering high-risk pneumococcal programme vaccines on the<br />
<strong>National</strong> <strong>Immunisation</strong> Register<br />
Children born prior to 1 January <strong>2008</strong><br />
Children born prior to 1 January <strong>2008</strong> and identified as meeting the eligibility criteria for<br />
the high-risk pneumococcal programme (see table 6.1) will continue to have their<br />
pneumococcal vaccines (PCV7 and 23PPV) entered onto the NIR using the<br />
pneumococcal programme.<br />
Children born between 1 January <strong>2008</strong> and 31 May <strong>2008</strong><br />
Children born between 1 January <strong>2008</strong> and 31 May <strong>2008</strong> who have commenced the<br />
high-risk pneumococcal programme would have already been entered on the NIR as<br />
part of the pneumococcal programme (PI).<br />
From 1 June <strong>2008</strong>, these high-risk children will automatically transfer to the NIR<br />
Childhood <strong>Schedule</strong> (CI) and their remaining PCV7 doses will recorded as part of this<br />
CI schedule.<br />
50 <strong>2008</strong> <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong>: <strong>Health</strong> <strong>Provider</strong> Booklet
When the high-risk child turns two years old and receives 23PPV vaccine, the PI<br />
programme takes over for these children (on the basis of the NIR receiving a 23PPV<br />
vaccine, an indicator of high risk).<br />
Children born from 1 June <strong>2008</strong><br />
PCV7 is included on the <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong> from 1 June <strong>2008</strong> for all<br />
children. PCV7 doses given to high-risk children born from 1 June <strong>2008</strong> will be recorded<br />
on the CI schedule of the NIR. When the high-risk child turns two years old and receives<br />
23PPV vaccine, the PI programme takes over for these children (on the basis of the NIR<br />
receiving a 23PPV vaccine, an indicator of high risk).<br />
6.4 Claiming for high-risk pneumococcal programme vaccines<br />
The immunisation benefit can be claimed for vaccines given as part of the high-risk<br />
pneumococcal programme for children under five years of age with a chronic condition.<br />
Claim using the codes as follows.<br />
• Vaccine 100 (PCV7) and indication 12 (at risk, no previous history), 13 (at risk,<br />
previous PCV7) or 14 (at risk, previous 23 PPV).<br />
• Or, if the PCV7 vaccine is given at six weeks, three or five months as part of the<br />
usual <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong> you may claim as a usual schedule vaccine,<br />
and when the child receives a dose of 23 PPV vaccine please claim under the high<br />
risk pneumococcal programme.<br />
<strong>2008</strong> <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong>: <strong>Health</strong> <strong>Provider</strong> Booklet 51
Appendix 1: <strong>Immunisation</strong> Catch-up <strong>Schedule</strong>s<br />
The following tables are for use from 1 June <strong>2008</strong>. These tables replace Appendix 2 of<br />
the <strong>Immunisation</strong> Handbook 2006 (Ministry of <strong>Health</strong> 2006).<br />
1.1 <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong> catch-up schedules<br />
Note: PCV7 is available from 1 June <strong>2008</strong> only for healthy infants born after 1 January<br />
<strong>2008</strong>. See Section 2.2 below for catch-up schedules for infants with chronic medical<br />
conditions who are eligible for funded pneumococcal vaccines.<br />
First dose at 3–5 months<br />
First dose DTaP-IPV-HepB/Hib PCV7<br />
6 week interval DTaP-IPV-HepB/Hib PCV7<br />
6 week interval DTaP-IPV-HepB/Hib PCV7<br />
At age 15 months Hib PCV7 MMR<br />
At age 4 years DTaP-IPV MMR<br />
At age 11 years<br />
dTap<br />
First dose at age 6 months<br />
First dose DtaP-IPV-HepB/Hib PCV7<br />
6 week interval DtaP-IPV-HepB/Hib PCV7<br />
6 week interval DtaP-IPV-HepB/Hib PCV7<br />
At age 15 months Hib PCV7 MMR<br />
At age 4 years DtaP-IPV MMR<br />
At age 11 years<br />
dTap<br />
First dose at 7–11 months<br />
First dose DTaP-IPV-HepB/Hib PCV7<br />
6 week interval DTaP-IPV-HepB/Hib PCV7<br />
6 week interval DTaP-IPV-HepB/Hib<br />
At age 15 months* Hib PCV7 MMR<br />
At age 4 years DTaP-IPV MMR<br />
At age 11 years<br />
dTap<br />
* The fourth dose of Hib vaccine and the third dose of PCV7 should be two months after the prior dose.<br />
However, this should not delay the administration of MMR at 15 months. If the third dose of Hib<br />
vaccine is given at 15 months or older the fourth dose can be omitted.<br />
52 <strong>2008</strong> <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong>: <strong>Health</strong> <strong>Provider</strong> Booklet
First dose at 12–14 months<br />
First dose DTaP-IPV-HepB/Hib MMR<br />
6 week interval* DTaP-IPV-HepB/Hib HepB<br />
6 week interval* DTaP-IPV HepB<br />
At age 4 years DTaP-IPV MMR<br />
At age 11 years<br />
dTap<br />
For children born after 1 January <strong>2008</strong>, two doses of PCV7 should be given at least six<br />
weeks apart. PCV7 should be given as a third injection at a scheduled visit.<br />
* Alternatively, at the third visits, DTaP-IPV-HepB/Hib vaccine may be given.<br />
First dose at 15 months–3 years<br />
First dose DTaP-IPV-HepB/Hib MMR<br />
6 week interval DTaP-IPV HepB<br />
6 week interval DTaP-IPV HepB<br />
At age 4 years DTaP-IPV MMR<br />
At age 11 years<br />
dTap<br />
Children born after 1 January <strong>2008</strong> are eligible for funded PCV7 vaccine from 1 June<br />
<strong>2008</strong>.<br />
For children aged 15–23 months, two doses of PCV7 should be given at least six weeks<br />
apart. PCV7 should be given as a third injection at visits one and two, but can be given<br />
at an additional visit. Alternatively, at the second visit and third visits, a DTaP-IPV-<br />
HepB/Hib and a PCV7 vaccine may be given. For ease of delivery though, additional<br />
doses of hib vaccine beyond 15 months are not required.<br />
For children aged 24–35 months, one dose of PCV7 should be given as a third injection<br />
at a scheduled visit but can be given at an additional visit. Alternatively, at the second<br />
visit, DTaP-IPV-HepB/Hib and a PCV7 vaccine may be given.<br />
First dose at 4 years<br />
First dose DTaP-IPV-Hep/Hib MMR<br />
6 week interval DTaP-IPV Hep B<br />
6 week interval DTaP-IPV Hep B<br />
6 month interval DTaP-IPV MMR<br />
At age 11 years<br />
dTap<br />
Children born after 1 January <strong>2008</strong> are eligible for funded PCV7 vaccines.<br />
For children age 24–48months, one dose of PCV7 should be given as a third injection at<br />
the first visit. Alternatively, at the second visit, DTaP-IPV-HepB/Hib and a PCV7<br />
vaccine may be given.<br />
<strong>2008</strong> <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong>: <strong>Health</strong> <strong>Provider</strong> Booklet 53
First dose at 5–7 years<br />
First dose DTaP-IPV HepB MMR<br />
1 month interval DTaP-IPV HepB<br />
1 month interval DTaP-IPV HepB<br />
6 months interval DTaP-IPV (or Td and IPV > 7 years) MMR<br />
At age 11 years<br />
dTap<br />
First dose at 7 years and older*<br />
First dose dTap* and IPV HepB MMR<br />
1 month interval Td and IPV HepB<br />
1 month interval Td and IPV HepB MMR<br />
10 year interval dTap* and IPV<br />
* dTap may be considered for all three doses of the primary series. See note 9 below.<br />
Notes<br />
1. There is considerable flexibility in these schedules, and the recommended intervals between doses<br />
are not sacrosanct. Vaccines may be given simultaneously and/or the schedule shortened to monthly<br />
intervals if this is deemed necessary to ensure the required numbers of doses are administered.<br />
2. If the schedule is interrupted, it is not necessary to repeat prior doses; simply resume the schedule as<br />
if no dose had been missed.<br />
3. If the immunisation status of a vaccine recipient is uncertain or unknown, then the vaccine provider<br />
should err on the side of giving rather than not giving the vaccine.<br />
4. If a child attends infrequently and failure to return for future immunisation is of concern, it is prudent to<br />
administer as many antigens as possible at the first visit.<br />
5. In the catch-up schedule for children 12–14 months of age, the third hepatitis B vaccine dose may be<br />
moved to a six-month interval if the MMR dose at 15 months coincides with the third catch-up visit and<br />
three injections are not accepted.<br />
6. MMR, Hib and pertussis are given as a priority for children 15 months of age and over because these<br />
diseases pose the greatest immediate risk.<br />
7. MMR should be given either at 15 months, or if the child/adult is older than 15 months, at the first<br />
immunisation visit.<br />
8. A single dose of Hib vaccine administered at 15 months of age and over is sufficient to induce<br />
immunity.<br />
9. After the seventh birthday, Td should be used. The dTap vaccine is given at age 11 years as a<br />
booster. As at <strong>2008</strong>, dTap and dTap-IPV are licensed for distribution for booster doses only.<br />
However, there are expected to be no safety concerns to giving three doses of dTap to previously<br />
unimmunised older children and adults. Therefore, using dTap should be considered for all catch-up<br />
and adult schedules for primary and booster immunisations.<br />
54 <strong>2008</strong> <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong>: <strong>Health</strong> <strong>Provider</strong> Booklet
1.2 High risk pneumococcal immunisation programme catch-up<br />
schedules<br />
Following are recommendations for pneumococcal vaccines for children at higher risk of<br />
pneumococcal disease who have received a dose of a pneumococcal vaccine<br />
previously.<br />
Age of child<br />
Previous dose(s) of any<br />
pneumococcal vaccine<br />
Recommendations<br />
23 months or<br />
under<br />
Any or none As in the <strong>Immunisation</strong> Handbook 2006, chapter 16,<br />
Table 16.6, page 325 (Ministry of <strong>Health</strong> 2006)<br />
24–59 months Four doses of PCV7<br />
vaccine<br />
24–59 months 1–3 doses of PCV7<br />
vaccine<br />
One dose of 23PPV vaccine at 24 months of age, 6–8<br />
weeks after the last dose of PCV7 vaccine; and one<br />
dose of 23PPV vaccine 3–5 years after the first dose<br />
One dose of PCV7 vaccine; one dose of 23PPV<br />
vaccine 6–8 weeks after the last dose of PCV7 vaccine;<br />
and one dose of 23PPV vaccine 3–5 years after the first<br />
dose<br />
24–59 months 1 dose of 23PPV Two doses of PCV7 vaccine, 6–8 weeks apart,<br />
beginning at 6–8 weeks after the dose of 23PPV<br />
vaccine; one dose of 23PPV vaccine 3–5 years after<br />
the first dose of 23PPV vaccine<br />
24–59 months No previous dose of PCV7<br />
or 23PPV vaccine<br />
Two doses of PCV7 vaccine 6–8 weeks apart; one<br />
dose of 23PPV vaccine 6–8 weeks after the last dose of<br />
PCV7 vaccine; and one dose of 23PPV vaccine 3–5<br />
years after the first dose of 23PPV vaccine<br />
PCV7 – 7 valent-conjugate pneumococcal vaccine (Prevenar®)<br />
23 PPV – 23 valent polysaccharide pneumococcal vaccine (Pneumovax®23)<br />
<strong>2008</strong> <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong>: <strong>Health</strong> <strong>Provider</strong> Booklet 55
Appendix 2: Pre/Post Splenectomy <strong>Immunisation</strong><br />
Programme<br />
The following groups are eligible for the pre/post splenectomy immunisation<br />
programme:<br />
• Children (0–16 years) pre* or post splenectomy or with functional asplenia.<br />
• Adults pre* or post splenectomy.<br />
These groups are eligible for the following funded vaccines.<br />
Eligibility criteria<br />
Children (0–16 years)<br />
pre* or post<br />
splenectomy or with<br />
functional asplenia<br />
Adults pre*- or postsplenectomy<br />
Funded vaccine (trade<br />
name)<br />
PCV7 (Prevenar®)<br />
23PPV (Pneumovax®23)<br />
Meningococcal ACYW135<br />
(Menomune®)<br />
Meningococcal B<br />
(MeNZB)<br />
Hib (Hiberix)<br />
23PPV (Pneumovax®23)<br />
Meningococcal ACYW135<br />
(Menomune®)<br />
Meningococcal B<br />
(MeNZB)<br />
Hib (Hiberix)<br />
Vaccine schedule<br />
See the <strong>Immunisation</strong> Handbook 2006, Table<br />
16.5, page 323, PCV7 vaccine schedule.<br />
See the <strong>Immunisation</strong> Handbook 2006, Table<br />
16.5, page 323, 23PPV vaccine schedule.<br />
Five-yearly 23PPV boosters are also funded.<br />
One dose<br />
Five-yearly Meningococcal ACYW135 boosters<br />
are also funded if still indicated (ie, risk)<br />
If the first dose is given at age ≥ 6 months: three<br />
doses 6 weeks apart.<br />
If the first dose is given age 6 weeks to 5 months<br />
give three doses at 6 weeks apart and a fourth<br />
dose at age 10 months.<br />
One dose<br />
Five-yearly boosters are also funded<br />
One dose<br />
Five-yearly Meningococcal ACYW135 boosters<br />
are also funded if still indicated (ie, risk)<br />
Three doses 6 weeks apart<br />
One dose<br />
* Where possible the vaccines should be administered at least 14 days before splenectomy – with the<br />
exception of MeNZB, where the vaccine course should be completed at least four weeks before<br />
splenectomy.<br />
Claiming for the Pre/Post Splenectomy <strong>Immunisation</strong> Programme vaccines<br />
PCV7 should be claimed as noted in the section 6.4, that is using the codes Vaccine<br />
100 (PCV7) and indication 12 (at risk, no previous history), 13 (at risk, previous PCV7)<br />
or 14 (at risk, previous 23PPV).<br />
56 <strong>2008</strong> <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong>: <strong>Health</strong> <strong>Provider</strong> Booklet
The remaining pre/post-splenectomy vaccines should be claimed using their usual claim<br />
code (IMMB for MeNZB TM , IMOA for the others) and usual vaccine code and indication<br />
11 (pre/post-splenectomy).<br />
For more details refer to the Ministry’s Frequently Asked Questions webpage at:<br />
http://www.moh.govt.nz/moh.nsf/indexmh/healthpac-faq-immunisation<br />
<strong>2008</strong> <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong>: <strong>Health</strong> <strong>Provider</strong> Booklet 57
References<br />
Black S, Shinefield H, Fireman B, et al. 2000. Efficacy, safety and immunogenicity of<br />
heptavalent pneumococcal conjugate vaccine in children. Northern California Kaiser<br />
Permanente Vaccine Study Center Group. Pediatr Infect Dis Journal 19: 187–95.<br />
Center KJ. 2007. Prevenar® vaccination: Review of the global data, 2007. Vaccine 25:<br />
3085–89.<br />
Centers for Disease Control and Prevention (CDC). 2006. Preventing tetanus, diphtheria, and<br />
pertussis among adolescents: Use of tetanus toxoid, reduced diphtheria toxoid and acellular<br />
pertusis vaccines. Recommendations of the Advisory Committee on Immunization Practices<br />
(ACIP). MMWR 55 (23 February).<br />
Cohen R, Levy C, de La Rocque F, et al. 2006. Impact of pneumococcal conjugate vaccine<br />
and of reduction of antibiotic resistance in nasopharyngeal carriage of nonsusceptible<br />
pneumococci in children with otitis media. Pediatrics Infect Dis Journal 25(11): 1001–7.<br />
Eskola J, Kilpi T, Palmu A, et al. 2001. Efficacy of a pneumococcal conjugate vaccine against<br />
acute otitis media. New England Journal of Medicine 344: 403–9.<br />
Fireman B, Black SB, Shinefield HR, et al. 2003. Impact of the pneumococcal conjugate<br />
vaccine on otitis media. Pediatrics Infect Dis Journal 22(1): 10–16.<br />
Hansen J, Black S, Shinefield H, et al. 2006. Effectiveness of heptavalent pneumococcal<br />
conjugate vaccine in children younger than five years for prevention of pneumonia: Updated<br />
analysis using WHO standard interpretation of chest radiographs. Pediatrics Inf Dis Journal<br />
25(9): 779–81.<br />
Heffernan HM, Blackmore TK, Martin DR. 2006. Invasive Pneumococcal Disease in New<br />
Zealand 1998–2005: Capsular serotypes and antimicrobial resistance.<br />
Hsu K, Pelton S, Karumuri S, et al. 2005. Population-based surveillance for childhood invasive<br />
pneumococcal disease in the era of conjugate vaccine. Pediatr Infect Dis J 24: 17–23.<br />
Kalies H, Grote V, Siedler A, et al. <strong>2008</strong>. Effectiveness of hexavalent vaccines against invasive<br />
Haemophilus influenzae type b disease: Germany’s experience after five years of licensure.<br />
Vaccine 26: 2545–52.<br />
Kelly C, Arnold R, Galloway Y, O’Hallahan J. 2007. A prospective study of the effectiveness of<br />
New Zealand meningococcal B vaccine. American Journal of Epidemiology 166: 817–23.<br />
Lennon D, Webb R. 2007. Final report for completed studies: Pneumococcal meningitis. From<br />
New Zealand Paediatric Surveillance Unit: Annual report 2006. Retrieved from:<br />
http://www.paediatrics.org.nz.<br />
Minh NH, He Q, Ramalho A, et al. 1999. Acellular vaccines containing reduced quantities of<br />
pertussis antigens as a booster in adolescents. Pediatrics 104: e70.<br />
Ministry of <strong>Health</strong>. 2006. <strong>Immunisation</strong> Handbook 2006. Wellington: Ministry of <strong>Health</strong>.<br />
Nachman S, Kim S, King J, et al. 2003. Safety and immunogenicity of a heptavalent<br />
pneumococcal conjugate vaccine in infants with human immunodeficiency virus type 1 infection.<br />
Pediatrics 112: 66–73.<br />
<strong>National</strong> Advisory Committee on <strong>Immunisation</strong>. 2002. An Advisory Committee Statement<br />
(ACS). Statement on recommended use of pneumococcal conjugate vaccine. Canadian<br />
Communicable Disease Report 28: ACS-2.<br />
58 <strong>2008</strong> <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong>: <strong>Health</strong> <strong>Provider</strong> Booklet
Reingold A, et al. <strong>2008</strong>. Invasive pneumococcal disease in children five years after conjugate<br />
vaccine introduction – eight states, 1998–2005. MMWR 57 (15 February).<br />
Shinefield H, Black S, Ray P, et al. 2002. Efficacy, immunogenicity and safety of heptavalent<br />
pneumococcal conjugate vaccine in low birth weight and preterm infants. Pediatr Infect Dis<br />
Journal 21: 182–6.<br />
Schmitt HJ, Wirsing von König CH, Neiss A, et al. 1997. Efficacy of acellullar pertussis vaccine<br />
in early childhood after household exposure. JAMA 275: 37–41.<br />
Singleton RJ, Hennessy TW, Bulkow LR, et al. 2007. Invasive pneumococcal disease caused<br />
by nonvaccine serotypes among Alaska native children with high levels of 7-valent<br />
pneumococcal conjugate vaccine coverage. JAMA 297: 1784–92.<br />
Tichmann-Schumann I, Soemantri P, Behre U, et al. 2005. Immunogenicity and reactogenicity<br />
of four doses of diphtheria-tetanus-three-component acellular pertussus-hepatitis B-inactivated<br />
polio virus-Haemophilus influenzae type b vaccine coadministered with 7-valent pneumococcal<br />
conjugate vaccine. Pediatr Infect Dis Journal 24: 70–7.<br />
Veenhoven R, Bogaert D, Uiterwaal C, et al. 2003. Effect of conjugate pneumococcal vaccine<br />
followed by polysaccharide pneumococcal vaccine on recurrent acute otitis media: a<br />
randomised study. Lancet 361: 2189–95.<br />
Ward JI, Cherry JD, Chang S, et al. 2005. Efficacy of an acellular pertussis vaccine among<br />
adolescents and adults. New England Journal of Medicine 353: 1555–63.<br />
Wassilak S, Roper M, Murphy T. 2004. Tetanus toxoid. In: SA Plotkin, WA Orienstein (eds).<br />
Vaccines (4th edition). Philadelphia: WB Saunders Company.<br />
Wharton M, Vitek C. 2004. Diphtheria toxoid. In: SA Plotkin, WA Orienstein (eds). Vaccines<br />
(4th edition). Philadelphia: WB Saunders Company.<br />
Whitney CG, Farley MM, Hadler J, et al. 2003. Decline in invasive pneumococcal disease after<br />
the introduction of protein – polysaccharide conjugate vaccine. New England Journal of<br />
Medicine 348(18): 1737–46.<br />
<strong>2008</strong> <strong>National</strong> <strong>Immunisation</strong> <strong>Schedule</strong>: <strong>Health</strong> <strong>Provider</strong> Booklet 59