Portal Hypertension-Pola 060810
Portal Hypertension-Pola 060810
Portal Hypertension-Pola 060810

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
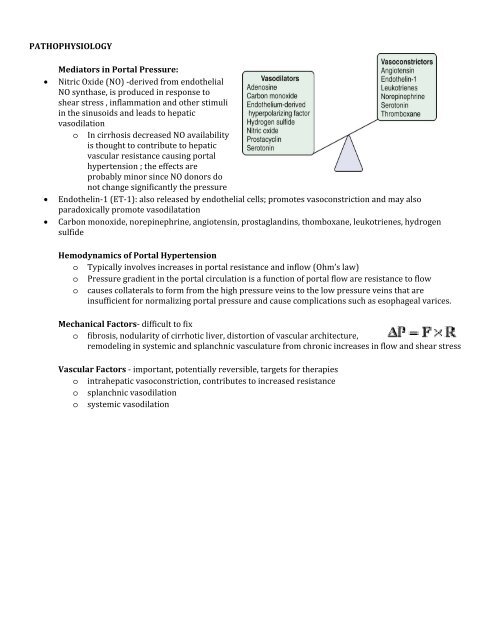
PATHOPHYSIOLOGY<br />
Mediators in <strong>Portal</strong> Pressure:<br />
• Nitric Oxide (NO) ‐derived from endothelial<br />
NO synthase, is produced in response to<br />
shear stress , inflammation and other stimuli<br />
in the sinusoids and leads to hepatic<br />
vasodilation<br />
o In cirrhosis decreased NO availability<br />
is thought to contribute to hepatic<br />
vascular resistance causing portal<br />
hypertension ; the effects are<br />
probably minor since NO donors do<br />
not change significantly the pressure<br />
• Endothelin‐1 (ET‐1): also released by endothelial cells; promotes vasoconstriction and may also<br />
paradoxically promote vasodilatation<br />
• Carbon monoxide, norepinephrine, angiotensin, prostaglandins, thomboxane, leukotrienes, hydrogen<br />
sulfide<br />
Hemodynamics of <strong>Portal</strong> <strong>Hypertension</strong><br />
o Typically involves increases in portal resistance and inflow (Ohm’s law)<br />
o Pressure gradient in the portal circulation is a function of portal flow are resistance to flow<br />
o causes collaterals to form from the high pressure veins to the low pressure veins that are<br />
insufficient for normalizing portal pressure and cause complications such as esophageal varices.<br />
Mechanical Factors‐ difficult to fix<br />
o fibrosis, nodularity of cirrhotic liver, distortion of vascular architecture,<br />
remodeling in systemic and splanchnic vasculature from chronic increases in flow and shear stress<br />
Vascular Factors ‐ important, potentially reversible, targets for therapies<br />
o intrahepatic vasoconstriction, contributes to increased resistance<br />
o splanchnic vasodilation<br />
o systemic vasodilation