Small-bowel imaging in Crohn's disease: a prospective, blinded, 4 ...
Small-bowel imaging in Crohn's disease: a prospective, blinded, 4 ...
Small-bowel imaging in Crohn's disease: a prospective, blinded, 4 ...
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
ORIGINAL ARTICLE: Cl<strong>in</strong>ical Endoscopy<strong>Small</strong>-<strong>bowel</strong> <strong>imag<strong>in</strong>g</strong> <strong>in</strong> Crohn’s <strong>disease</strong>: a <strong>prospective</strong>, bl<strong>in</strong>ded,4-way comparison trialCraig A. Solem, MD, Edward V. Loftus Jr., MD, Joel G. Fletcher, MD, Todd H. Baron, MD,Christopher J. Gostout, MD, Bret T. Petersen, MD, William J. Trema<strong>in</strong>e, MD, Laurence J. Egan, MD,William A. Faubion, MD, Kenneth W. Schroeder, MD, PhD, Darrell S. Pardi, MD, Karen A. Hanson, RN, CNP,Debra A. Jewell, RN, John M. Barlow, MD, Jeff L. Fidler, MD, James E. Huprich, MD, C. Daniel Johnson, MD,W. Scott Harmsen, MS, Alan R. Z<strong>in</strong>smeister, PhD, William J. Sandborn, MDRochester, M<strong>in</strong>nesota, USABackground: With the <strong>in</strong>troduction of new techniques to image the small <strong>bowel</strong>, there rema<strong>in</strong>s uncerta<strong>in</strong>tyabout their role for diagnos<strong>in</strong>g Crohn’s <strong>disease</strong>.Objective: To assess the sensitivity and specificity of capsule endoscopy (CE), CT enterography (CTE), ileocolonoscopy,and small-<strong>bowel</strong> follow-through (SBFT) <strong>in</strong> the diagnosis of small <strong>bowel</strong> Crohn’s <strong>disease</strong>.Methods: Prospective, bl<strong>in</strong>ded trial.Sett<strong>in</strong>g: Inflammatory <strong>bowel</strong> <strong>disease</strong> cl<strong>in</strong>ic at an academic medical center.Patients: Known or suspected Crohn’s <strong>disease</strong>. Exclusion criteria <strong>in</strong>cluded known abdom<strong>in</strong>al abscess and nonsteroidalanti-<strong>in</strong>flammatory drug (NSAID) use. Partial small-<strong>bowel</strong> obstruction (PSBO) at CTE excluded patientsfrom subsequent CE.Interventions: Patients underwent all 4 tests over a 4-day period.Ma<strong>in</strong> Outcome Measurements: Sensitivity, specificity, and accuracy of each test to detect active small-<strong>bowel</strong>Crohn’s <strong>disease</strong>. The criterion standard was a consensus diagnosis based upon cl<strong>in</strong>ical presentation and all4 studies.Results: Forty-one CTE exam<strong>in</strong>ations were performed. Seven patients (17%) had an asymptomatic PSBO. Fortypatients underwent colonoscopy, 38 had SBFT studies, and 28 had CE exam<strong>in</strong>ations. <strong>Small</strong>-<strong>bowel</strong> Crohn’s <strong>disease</strong>was active <strong>in</strong> 51%, absent <strong>in</strong> 42%, <strong>in</strong>active <strong>in</strong> 5%, and suspicious <strong>in</strong> 2% of patients. The sensitivity of CEfor detect<strong>in</strong>g active small-<strong>bowel</strong> Crohn’s <strong>disease</strong> was 83%, not significantly higher than CTE (83%), ileocolonoscopy(74%), or SBFT (65%). However, the specificity of CE (53%) was significantly lower than the other tests(P ! .05). One patient developed a transient PSBO due to CE, but no patients had reta<strong>in</strong>ed capsules.Limitation: Use of a consensus cl<strong>in</strong>ical diagnosis as the criterion standarddbut this is how Crohn’s <strong>disease</strong> isdiagnosed <strong>in</strong> practice.Conclusions: The sensitivity of CE for active small-<strong>bowel</strong> Crohn’s <strong>disease</strong> was not significantly different fromCTE, ileocolonoscopy, or SBFT. However, lower specificity and the need for preced<strong>in</strong>g small-<strong>bowel</strong> radiography(due to the high frequency of asymptomatic PSBO) may limit the utility of CE as a first-l<strong>in</strong>e test for Crohn’s<strong>disease</strong>. (Gastro<strong>in</strong>test Endosc 2008;68:255-66.)Abbreviations: CBC, complete blood count; CE, capsule endoscopy; CRP,C-reactive prote<strong>in</strong>; CTE, CT enterography; NSAID, non-steroidal anti-<strong>in</strong>flammatorydrug; PEG, polyethylene glycol; PSBO, partial small-<strong>bowel</strong>obstruction; SB, small-<strong>bowel</strong>; SBFT, small <strong>bowel</strong> follow-through.Copyright ª 2008 by the American Society for Gastro<strong>in</strong>test<strong>in</strong>al Endoscopy0016-5107/$32.00doi:10.1016/j.gie.2008.02.017Modern cl<strong>in</strong>icians have many options available to themfor small-<strong>bowel</strong> (SB) <strong>imag<strong>in</strong>g</strong> <strong>in</strong> Crohn’s <strong>disease</strong>. Bariumstudies have traditionally been the conventional test forSB radiography <strong>in</strong> this sett<strong>in</strong>g. 1-6 Barium small-<strong>bowel</strong> follow-through(SBFT) exam<strong>in</strong>ations have previously beenshown to be preferable to barium enteroclysis studies <strong>in</strong>a <strong>prospective</strong> study <strong>in</strong>volv<strong>in</strong>g patients with Crohn’swww.giejournal.org Volume 68, No. 2 : 2008 GASTROINTESTINAL ENDOSCOPY 255
<strong>Small</strong>-<strong>bowel</strong> <strong>imag<strong>in</strong>g</strong> <strong>in</strong> Crohn’s <strong>disease</strong>Solem et alprocedure and the will<strong>in</strong>gness to repeat the procedure <strong>in</strong>the future.Consensus reference standardAfter the results of the 4 studies (CTE, ileocolonoscopy,CE, and SBFT) were recorded for each patient, the f<strong>in</strong>d<strong>in</strong>gsof all of the studies were reviewed at the conclusionof the study period by a consensus panel of co-<strong>in</strong>vestigatorsrepresent<strong>in</strong>g each diagnostic modality and a referr<strong>in</strong>ggastroenterologist, to establish a consensus global assessmentof SB Crohn’s <strong>disease</strong>. If there were discordantresults among studies, this discussion necessitated achange of op<strong>in</strong>ion by one or more <strong>in</strong>vestigators about the<strong>in</strong>itial <strong>in</strong>terpretation of the f<strong>in</strong>d<strong>in</strong>gs of one or more studies.More specifically, the <strong>in</strong>vestigator represent<strong>in</strong>g one of thediagnostic modalities had to concede that a mistake hadbeen made <strong>in</strong> the <strong>in</strong>itial <strong>in</strong>terpretation of the SB f<strong>in</strong>d<strong>in</strong>gswith their modality. Thus, the reference standard for assessmentof Crohn’s <strong>disease</strong> activity was the f<strong>in</strong>al determ<strong>in</strong>ationof the consensus panel (ie, active, suspicious foractive, <strong>in</strong>active, or absent). The consensus criterion standardhas previously been used <strong>in</strong> a <strong>prospective</strong> trial oftests evaluat<strong>in</strong>g perianal Crohn’s <strong>disease</strong>. 42 After the modifiedread<strong>in</strong>gs were used to establish the consensus referencestandard for SB <strong>disease</strong>, the orig<strong>in</strong>al <strong>in</strong>terpretationof each study as recorded on the study forms, was usedto estimate the performance characteristics of the tests.In a prespecified primary analysis, the diagnoses of activeand suspicious SB Crohn’s <strong>disease</strong> were grouped together,and the diagnoses of <strong>in</strong>active or absent <strong>disease</strong>were grouped together, for all reported analyses to detectactive SB Crohn’s. A prespecified secondary analysis wasalso performed for detect<strong>in</strong>g the presence of SB Crohn’s<strong>disease</strong> by comb<strong>in</strong><strong>in</strong>g the categories of active, suspicious,and <strong>in</strong>active <strong>disease</strong>, and compar<strong>in</strong>g this group to the absentcategory. (However, the latter results were consistentwith those of active SB Crohn’s, and are therefore not reported<strong>in</strong> the Results.)Statistical analysisFor the primary analysis, the sensitivity of each test wascalculated by divid<strong>in</strong>g the number of patients with positivetest results by the number of patients with active or suspiciousSB Crohn’s <strong>disease</strong> based on the consensus criterionstandard. The specificity of each test was calculated by divid<strong>in</strong>gthe number of patients with negative tests resultsby the number of patients with <strong>in</strong>active or absent SBCrohn’s <strong>disease</strong> based on the consensus criterion standard.The diagnostic accuracy of each test was calculatedby the number of patients with test results <strong>in</strong> agreementwith the consensus criterion standard divided by the numberof tests performed. Exact b<strong>in</strong>omial 95% confidence <strong>in</strong>tervalswere also reported.The operat<strong>in</strong>g characteristics of each SB exam<strong>in</strong>ationwere compared to those of CE <strong>in</strong> the subset of patientshav<strong>in</strong>g both CE and another SB exam<strong>in</strong>ation. The sensitivity,specificity, and accuracy of CTE, ileocolonoscopy, andSBFT were compared to CE by us<strong>in</strong>g McNemar’s test ofpaired proportions. The comb<strong>in</strong>ed sensitivity, specificity,and accuracy of all pairs of tests that could be consideredwere also estimated aga<strong>in</strong>st the consensus criterion standard.McNemar’s test was used to compare the performancesof pairs of tests (CE plus CTE vs ileocolonoscopyplus SBFT, CE plus ileocolonoscopy vs CTE plus SBFT,and CTE plus ileocolonoscopy vs CE plus SBFT). Comparisonsof pairs conta<strong>in</strong><strong>in</strong>g a common diagnostic test were notperformed. The P values were not adjusted for multiplecomparisons.RESULTSForty-two patients enrolled <strong>in</strong> the study (Fig. 1). Onepatient withdrew for personal reasons before any diagnosticstudies were performed and was not <strong>in</strong>cluded <strong>in</strong> theanalysis. The median age of the 41 patients (81% female)participat<strong>in</strong>g <strong>in</strong> the study was 40.1 years (range 18.9-73.5years). Forty-one patients underwent CTE. One patientsubsequently withdrew for personal reasons and had nofurther studies. Ileoscopy was feasible <strong>in</strong> 36 of the 40 colonoscopies.Thirty-eight patients had SBFT exam<strong>in</strong>ationsafter 1 patient exited the study due to a stricture detectedon CTE, and 1 patient underwent surgery for a PSBO.Twenty-eight patients had CE studies after 10 patientswere excluded for PSBO or abscess, and 2 patients leftthe study for personal reasons. One capsule study was repeateddue to a technical malfunction with the <strong>in</strong>itialexam<strong>in</strong>ation (no images were obta<strong>in</strong>ed), and one capsulewas reta<strong>in</strong>ed <strong>in</strong> the stomach for the duration of batterylife, result<strong>in</strong>g <strong>in</strong> no SB images (but the capsule eventuallypassed spontaneously). Twenty-seven capsule studieswere then used for analysis. Table 1 details the comb<strong>in</strong>ationsof the 4 SB exam<strong>in</strong>ations patients received.The study co-<strong>in</strong>vestigators were able to reach a consensusop<strong>in</strong>ion regard<strong>in</strong>g the global assessment of SB Crohn’s<strong>disease</strong> after unbl<strong>in</strong>d<strong>in</strong>g at the conclusion of study <strong>in</strong> all 41patients who had one or more SB studies (Table 2). Thef<strong>in</strong>al cl<strong>in</strong>ical diagnoses for all patients, not limited to theSB, are reported <strong>in</strong> Table 3.Table 4 reports the sensitivity, specificity, and accuracyof the 4 SB tests <strong>in</strong>dividually, with the consensus criterionstandard used to classify patient status as either ‘‘active’’(active plus suspicious) or ‘‘<strong>in</strong>active’’ (<strong>in</strong>active plus absent).The sensitivity for the detection of active SB Crohn’s<strong>disease</strong> was 83% for CE, 82% for CTE, 74% for ileocolonoscopy,and 65% for SBFT. The specificity for SB Crohn’s<strong>disease</strong> was 100% for ileocolonoscopy, 94% for SBFT,89% for CTE, and 53% for CE. The overall accuracy forSB Crohn’s was 86% for ileocolonoscopy, 85% for CTE,79% for SBFT, and 67% for CE.The performance of CTE, ileocolonoscopy, and SBFTwere each compared with that of CE (Table 5). There258 GASTROINTESTINAL ENDOSCOPY Volume 68, No. 2 : 2008 www.giejournal.org
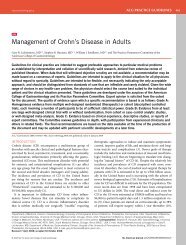
Solem et al<strong>Small</strong>-<strong>bowel</strong> <strong>imag<strong>in</strong>g</strong> <strong>in</strong> Crohn’s <strong>disease</strong>Figure 1. A graphic representation of patient movement throughout the course of the study.TABLE 1. Comb<strong>in</strong>ations of the 4 SB exam<strong>in</strong>ationsundergone by 42 participants <strong>in</strong>itially enrolled <strong>in</strong>the studyCE(n Z 27)Ileocolonoscopy(n Z 36)SBFT(n Z 38)CTE(n Z 41)No.patientsNo No No No 1No No No Yes 1No No Yes Yes 3No Yes No Yes 2No Yes Yes Yes 8Yes No Yes Yes 1Yes Yes Yes Yes 26CE, Capsule endoscopy; SBFT, small <strong>bowel</strong> follow-through; CTE,computed tomographic enterography.were 12 patients <strong>in</strong> each of 3 sensitivity comparisons, andfor specificity there were 15 patients, except to compareCE versus SBFT, where only 14 received both exam<strong>in</strong>ations.The sensitivity of CE (83%) was not significantly differentfrom that of CTE (67%, P Z .63), ileocolonoscopy(67%, P Z .69), or SBFT (50%, P Z .22). However, thespecificity of CE (53%) was significantly lower than thatfor either CTE (100%, P Z .02) or SBFT (100%, P Z.02). The specificity of CE (43%) was also significantlylower among the 14 patients hav<strong>in</strong>g ileocolonoscopy(100%, P Z .03). The lower specificity of CE was due toTABLE 2. F<strong>in</strong>al consensus diagnosis for small-<strong>bowel</strong>Crohn’s <strong>disease</strong> <strong>in</strong> 41 patients who underwent at least 1diagnostic test, and <strong>in</strong> 26 patients who underwent all 4tests<strong>Small</strong>-<strong>bowel</strong> Crohn’s<strong>disease</strong> diagnosisAll patients,n (%)*Patients withall 4 tests, n (%)yActive 21 (51) 11 (42)Absent 17 (42) 12 (46)Inactive 2 (5) 2 (8)Suspicious 1 (2) 1 (4)Total 41 (100) 26 (100)*Percentage of the group undergo<strong>in</strong>g at least 1 SB <strong>imag<strong>in</strong>g</strong> test.yPercentage of the group undergo<strong>in</strong>g all 4 tests.the fact that, <strong>in</strong> 7 patients, there were f<strong>in</strong>d<strong>in</strong>gs that ledthe CE reader to deem the exam<strong>in</strong>ation either suspicious(n Z 5) or ‘‘def<strong>in</strong>ite’’ (n Z 2) for active Crohn’s <strong>disease</strong>,but accord<strong>in</strong>g to the consensus criterion standard, thesepatients had either no evidence of Crohn’s <strong>disease</strong> (n Z5) or only <strong>in</strong>active <strong>disease</strong> (n Z 2).The performance characteristics of pairs of SB exam<strong>in</strong>ationsaga<strong>in</strong>st the consensus criterion standard were estimated(Table 4). A patient was classified positive foractive SB Crohn’s <strong>disease</strong> if either of the 2 exam<strong>in</strong>ations<strong>in</strong>dicated active <strong>disease</strong>. The sensitivity for comb<strong>in</strong>ationsof exam<strong>in</strong>ations ranged from a high of 100% for the CEand ileocolonoscopy comb<strong>in</strong>ation to a low of 78% forwww.giejournal.org Volume 68, No. 2 : 2008 GASTROINTESTINAL ENDOSCOPY 259
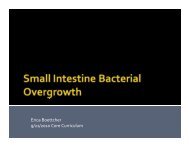
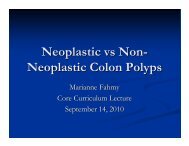
<strong>Small</strong>-<strong>bowel</strong> <strong>imag<strong>in</strong>g</strong> <strong>in</strong> Crohn’s <strong>disease</strong>Solem et alTABLE 3. F<strong>in</strong>al overall cl<strong>in</strong>ical diagnosis (not limited tothe small <strong>in</strong>test<strong>in</strong>e) <strong>in</strong> all 41 patients who underwent atleast 1 diagnostic test, and <strong>in</strong> 26 patients whounderwent all 4 testsCl<strong>in</strong>icaldiagnosisAllpatients,n (%)*Patientswith all 4tests, n (%)yCrohn’s <strong>disease</strong> 30 (73%) 19 (73%)Indeterm<strong>in</strong>ate abdom<strong>in</strong>al pa<strong>in</strong> 3 (7%) 3 (11%)Irritable <strong>bowel</strong> syndrome 2 (5%) 2 (8%)Ulcerative colitis 1 (2%) 0 (0%)Indeterm<strong>in</strong>ate colitis 1 (2%) 0 (0%)Carc<strong>in</strong>oid 1 (2%) 0 (0%)Submucosal mass, small <strong>bowel</strong> 1 (2%) 1 (4%)Gastroparesis 1 (2%) 1 (4%)Indeterm<strong>in</strong>ate diarrhea 1 (2%) 0 (0%)Total 41 (100%) 26 (100%)*Percentage of the group undergo<strong>in</strong>g at least 1 SB <strong>imag<strong>in</strong>g</strong> test.yPercentage of the group undergo<strong>in</strong>g all 4 tests.the ileocolonoscopy and SBFT comb<strong>in</strong>ation. The specificityof exam<strong>in</strong>ation comb<strong>in</strong>ations aga<strong>in</strong>st the criterion standardranged from a high of 100% for SBFT plusileocolonoscopy to a low of 53% for both the CE plusSBFT and CE plus CTE comb<strong>in</strong>ations. The overall accuracyof exam<strong>in</strong>ation comb<strong>in</strong>ations aga<strong>in</strong>st the criterion standardranged from 89% for both the CTE plus ileocolonoscopyand CTE plus SBFT comb<strong>in</strong>ations to 70% for theCE plus CTE and CE plus SBFT comb<strong>in</strong>ations.No pair of SB exam<strong>in</strong>ations was significantly more sensitivethan the comb<strong>in</strong>ation conta<strong>in</strong><strong>in</strong>g the other two exam<strong>in</strong>ations(among the 4 SB exam<strong>in</strong>ations), P O .05(Table 6). However, each comb<strong>in</strong>ation of exam<strong>in</strong>ationsthat <strong>in</strong>cluded CE had a significantly lower specificity(57%) than did the opposite pair of exam<strong>in</strong>ations (P Z.03 for each of the 3 comparisons, unadjusted).Patients completed a questionnaire at the end of thestudy. All patients swallowed the capsule easily. N<strong>in</strong>etytwopercent of patients did not experience any pa<strong>in</strong> dur<strong>in</strong>gthe CE study, significantly better than colonoscopy(P ! .05), but no better than CTE or SBFT (P O .05).N<strong>in</strong>ety-three percent of patients stated they would undergoa CE study aga<strong>in</strong>, which was not significantly differentthan the other tests (P O .05).Even though all patients with obstructive symptomswere excluded from study enrollment, we detected anasymptomatic PSBO <strong>in</strong> 7 patients (17%) on CTE (Fig. 2),exclud<strong>in</strong>g them from CE. Soon after capsule <strong>in</strong>gestion,one patient with a very long segment of active <strong>disease</strong>but without PSBO on CTE (3.4%) experienced a highlysymptomatic PSBO requir<strong>in</strong>g hospitalization, but the capsulepassed with<strong>in</strong> a few days follow<strong>in</strong>g medical therapywith corticosteroids and <strong>in</strong>fliximab, with symptoms resolv<strong>in</strong>g(Fig. 3). Unlike the higher capsule retention rates seen<strong>in</strong> other studies, we had no reta<strong>in</strong>ed capsules (confirmedby radiograph) us<strong>in</strong>g our diagnostic algorithm.Chyme significantly limited study quality <strong>in</strong> 4 patientswho underwent CE (14%) despite efforts to cleanse with1 L PEG solution prior to the study. The term<strong>in</strong>al ileumwas exam<strong>in</strong>ed completely <strong>in</strong> only 75% of studies. One capsulestudy had a technical malfunction result<strong>in</strong>g <strong>in</strong> no images.In a s<strong>in</strong>gle patient with suspected Crohn’s <strong>disease</strong>,CE demonstrated multiple SB erosions when the other 3SB tests were normal (Fig. 4).DISCUSSIONIn this <strong>prospective</strong>, bl<strong>in</strong>ded trial, we compared 4 primarysmall-<strong>in</strong>test<strong>in</strong>al <strong>imag<strong>in</strong>g</strong> modalities <strong>in</strong> the diagnosisof SB Crohn’s <strong>disease</strong>. In contrast to the other studies exam<strong>in</strong><strong>in</strong>gthe utility of CE <strong>in</strong> patients with known or suspectedCrohn’s <strong>disease</strong>, 22,27,29,33-40 we believe this is theonly <strong>prospective</strong>, bl<strong>in</strong>ded trial compar<strong>in</strong>g all 4 primarySB <strong>imag<strong>in</strong>g</strong> modalities over a short time period, avoid<strong>in</strong>gboth treatment and natural history effects. Unlike the ‘‘diagnosticyield’’ reported <strong>in</strong> most published CE studies, weestablished a surrogate criterion standard, allow<strong>in</strong>g us tocalculate the sensitivity, specificity, and accuracy of eachtest for diagnos<strong>in</strong>g SB Crohn’s <strong>disease</strong>. We found thatthere was no significant difference among CTE, CE, ileocolonoscopy,and SBFT for the sensitivity or accuracy of diagnos<strong>in</strong>gSB Crohn’s <strong>disease</strong>. CTE and CE demonstratedsimilarly high sensitivity for SB Crohn’s, which was numericallysuperior to SBFT and ileocolonoscopy. Although thenumerical superiority of CTE and CE was not statisticallysignificant, this may have been due to the limited samplesize and potential lack of power to detect a significant difference.Comb<strong>in</strong><strong>in</strong>g diagnostic tests may improve sensitivity,and this is commonly used <strong>in</strong> cl<strong>in</strong>ical practice. Wefound that the specificity of CE for SB Crohn’s <strong>disease</strong>was significantly lower than other SB <strong>imag<strong>in</strong>g</strong> modalities,which lowered its overall accuracy. Our study also <strong>in</strong>directlysuggests that SB radiologic <strong>imag<strong>in</strong>g</strong> may be neededprior to CE <strong>in</strong> suspected or known Crohn’s <strong>disease</strong> patients,due to the high frequency (17%) of asymptomaticPSBO. When we used an algorithm of perform<strong>in</strong>g CTEprior to CE and us<strong>in</strong>g a f<strong>in</strong>d<strong>in</strong>g of stricture with proximal<strong>bowel</strong> dilation to preclude <strong>in</strong>gestion of the endoscopycapsule, we observed no capsule retention.The f<strong>in</strong>d<strong>in</strong>g of a lower specificity of CE for SB Crohn’s<strong>disease</strong> is not entirely unexpected. ‘‘Diagnostic yield’’ asa measure of the operat<strong>in</strong>g performance of a diagnostictest is less than idealdit merely reports the prevalenceof abnormalities detected by a particular <strong>imag<strong>in</strong>g</strong> modalityand does not attempt to determ<strong>in</strong>e whether those260 GASTROINTESTINAL ENDOSCOPY Volume 68, No. 2 : 2008 www.giejournal.org
Solem et al<strong>Small</strong>-<strong>bowel</strong> <strong>imag<strong>in</strong>g</strong> <strong>in</strong> Crohn’s <strong>disease</strong>TABLE 4. Individual performance estimates of 4 diagnostic tests and all pairs of these tests for active small-<strong>bowel</strong> Crohn’s <strong>disease</strong>*SB test Patients tested, n Sensitivity (%) 95% CI Specificity (%) 95% CI Accuracy (%) 95% CIIndividual testCE 27 10/12 (83) 52-98 8/15 (53) 27-79 18/27 (67) 46-83CTE 41 18/22 (82) 60-95 17/19 (89) 67-99 35/41 (85) 71-94Ileocolonoscopy 36 14/19 (74) 49-91 17/17 (100) 80-100 31/36 (86) 71-95SBFT 38 13/20 (65) 41-8 17/18 (94) 73-100 30/38 (79) 63-90Pairs of TestsCE & CTE 27 11/12 (92) 62-100 8/15 (53) 27-79 19/27 (70) 50-86CE & ileocolonoscopy 26 12/12 (100) 74-100 8/14 (57) 29-82 20/26 (77) 56-91CE & SBFT 27 11/12 (92) 62-100 8/15 (53) 27-79 19/27 (70) 50-86SBFT & ileocolonoscopy 34 14/18 (78) 52-94 16/16 (100) 79-100 30/34 (88) 73-97CTE & ileocolonoscopy 36 16/19 (84) 60-97 16/17 (94) 71-100 32/36 (89) 74-97CTE & SBFT 38 17/20 (85) 62-97 17/18 (94) 73-100 34/38 (89) 75-97CTE, CT enterography; CE, capsule endoscopy; SBFT, small-<strong>bowel</strong> follow-through; 95% CI, 95% confidence <strong>in</strong>tervals.*Criterion standard is based on consensus diagnosis of active Crohn’s <strong>disease</strong> or suspicious for Crohn’s <strong>disease</strong>.TABLE 5. Comparison of sensitivity and specificitybetween capsule endoscopy and 3 other diagnostictests for active small-<strong>bowel</strong> Crohn’s <strong>disease</strong>*SB testSensitivity(%)P-valueySpecificity(%)P-valueyCE 10/12 (83) ref 8/15 (53) refCTE 8/12 (67) .63 15/15 (100) .02Ileocolonoscopy 8/12 (67) .69 14/14 (100) .03SBFT 6/12 (50) .22 15/15 (100) .02CTE, CT enterography; CE, capsule endoscopy; SBFT, small-<strong>bowel</strong>follow-through; 95% CI, 95% confidence <strong>in</strong>tervals.*Criterion standard is based on consensus diagnosis of activeCrohn’s <strong>disease</strong> or suspicious for Crohn’s <strong>disease</strong>.yUs<strong>in</strong>g Mc Nemar’s test for paired proportions, test<strong>in</strong>g performancecompared to the CE exam<strong>in</strong>ation, unadjusted for multiplecomparisons.abnormal f<strong>in</strong>d<strong>in</strong>gs are cl<strong>in</strong>ically significant. Most studiesreport<strong>in</strong>g ‘‘diagnostic yield’’ do so because the test isnot be<strong>in</strong>g compared aga<strong>in</strong>st a reference standard. CE isan extremely sensitive tool for direct visualization ofthe SB mucosa. As <strong>in</strong> most diagnostic tests, improvedsensitivity typically comes at the cost of decreased specificity.43 Goldste<strong>in</strong> et al 44 found that 22% of asymptomaticcontrol patients who denied recent NSAID <strong>in</strong>gestion hadSB abnormalities at CE, with an average of 4 lesions persubject. As several CE f<strong>in</strong>d<strong>in</strong>gs, such as mucosal erythema,are nonspecific, and do not <strong>in</strong>dicate a diagnosisof active Crohn’s <strong>disease</strong> by themselves, their <strong>in</strong>clusionTABLE 6. Selected comparisons of sensitivity andspecificity between pairs of small-<strong>bowel</strong> exam<strong>in</strong>ations*CE &ileocolonoscopySensitivity(%)P- Specificityvaluey (%)12/12 (100) 8/14 (57)P-valueyCTE & SBFT 9/12 (75) .25 14/14 (100) .03CE & CTE 11/12 (92) 8/14 (57)SBFT &ileocolonoscopy9/12 (75) .63 14/14 (100) .03CE & SBFT 11/12 (92) 8/14 (57)CTE &ileocolonoscopy9/12 (75) .63 14/14 (100) .03CTE, CT enterography; CE, capsule endoscopy; SBFT, small-<strong>bowel</strong>follow-through; 95% CI, 95% confidence <strong>in</strong>tervals.*Criterion standard is based on consensus diagnosis of activeCrohn’s <strong>disease</strong> or suspicious for Crohn’s <strong>disease</strong>.yUs<strong>in</strong>g McNemar’s test for paired proportions, unadjusted formultiple comparisons.<strong>in</strong>to reference standard assessments of <strong>disease</strong> activity<strong>in</strong> SB <strong>imag<strong>in</strong>g</strong> trials may result <strong>in</strong> confirmation bias favor<strong>in</strong>gCE.Buchman et al 36 used SBFT as a method to detect SBstrictures that may lead to reta<strong>in</strong>ed capsules, and founda 29% <strong>in</strong>cidence of SB strictures <strong>in</strong> Crohn’s patients, whichprecluded capsule endoscopy. By us<strong>in</strong>g SBFT as a screen<strong>in</strong>gexam<strong>in</strong>ation, they observed 2 episodes of capsule retention(7%). Voderholzer et al 27 compared CE and CTEwww.giejournal.org Volume 68, No. 2 : 2008 GASTROINTESTINAL ENDOSCOPY 261
<strong>Small</strong>-<strong>bowel</strong> <strong>imag<strong>in</strong>g</strong> <strong>in</strong> Crohn’s <strong>disease</strong>Solem et alFigure 2. A, B, C, Computed tomography enterography <strong>in</strong> a 43-year-old woman with Crohn’s <strong>disease</strong>, depict<strong>in</strong>g asymptomatic PSBO due to multiplesegments of actively <strong>in</strong>flamed jejunum, preclud<strong>in</strong>g <strong>in</strong>gestion of endoscopy capsule. Axial and 2D multiplanar reformatted images depict both lum<strong>in</strong>alnarrow<strong>in</strong>g caused by active <strong>in</strong>flammation (with segmental hyperenhancement mural stratification, arrows) and prestenotic <strong>bowel</strong> dilation(arrowheads).<strong>in</strong> 56 patients with known Crohn’s <strong>disease</strong>. 27 CTE was performedprior to CE, and 27% of patients were precludedfrom CE because of strictures. 27 They used stricter criteriafor exclud<strong>in</strong>g patients from CE (ie, stricture !1-cm lum<strong>in</strong>al diameter with no proximal SB dilation required),but still experienced one episode of capsuleretention (2%) requir<strong>in</strong>g removal from the jejunum withpush enteroscopy, and one episode of symptomaticPSBO requir<strong>in</strong>g high-dose corticosteroid therapy beforespontaneous passage.Our results are somewhat at variance with other studiescompar<strong>in</strong>g CE and CTE <strong>in</strong> patients with known or suspectedCrohn’s <strong>disease</strong>. 22,27,29 A meta-analysis of these 3studies suggested that the prevalence of abnormalities detectedon CE was 38% higher than that of CTE. 41 However,this value was significantly higher than CTE only for thesubgroup of patients with known Crohn’s <strong>disease</strong>. We believethe differences <strong>in</strong> study results are due to a numberof factors. In one of these studies, 22 the enteric contrastused apparently was a positive agent (30% Telebrix), not262 GASTROINTESTINAL ENDOSCOPY Volume 68, No. 2 : 2008 www.giejournal.org
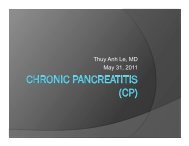
Solem et al<strong>Small</strong>-<strong>bowel</strong> <strong>imag<strong>in</strong>g</strong> <strong>in</strong> Crohn’s <strong>disease</strong>Figure 3. A, B, C, D, SB ulceration and stenosis <strong>in</strong> the patient who experienced a highly symptomatic PSBO shortly after capsule <strong>in</strong>gestion, result<strong>in</strong>g <strong>in</strong>hospitalization for several days. E, CTE demonstrated approximately 50 cm of actively <strong>in</strong>flamed ileum with mural enhancement and stratification (arrows),but without any proximal SB dilation (arrowhead). The symptoms resolved and the capsule eventually passed after steroid and <strong>in</strong>fliximabtreatment.a negative/neutral contrast agent, as used <strong>in</strong> our study. Useof a positive contrast would dim<strong>in</strong>ish the operat<strong>in</strong>g characteristicsof CTE, as it would not take advantage of thedifferences <strong>in</strong> attenuation between the <strong>bowel</strong> lumen and<strong>bowel</strong> wall. Furthermore, our study was the only one ofthese that met both of the follow<strong>in</strong>g criteria: there existeda range of diagnostic uncerta<strong>in</strong>ty (recruitment of bothknown and suspected Crohn’s), and the readers of eachwww.giejournal.org Volume 68, No. 2 : 2008 GASTROINTESTINAL ENDOSCOPY 263
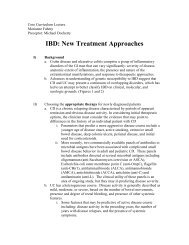
<strong>Small</strong>-<strong>bowel</strong> <strong>imag<strong>in</strong>g</strong> <strong>in</strong> Crohn’s <strong>disease</strong>Solem et alFigure 4. A, B, C, D, SB ulcers on capsule endoscopy <strong>in</strong> the s<strong>in</strong>gle patient found to have active SB Crohn’s <strong>disease</strong> on CE despite all other <strong>imag<strong>in</strong>g</strong>studies be<strong>in</strong>g normal (3.4%).modality were bl<strong>in</strong>ded to the results of the other modalities.Furthermore, <strong>in</strong> our study, all patients underwent all<strong>imag<strong>in</strong>g</strong> modalities after <strong>in</strong>formed consent had been obta<strong>in</strong>ed;<strong>in</strong> other words, the decision to perform certa<strong>in</strong>tests, or even enroll patients, was not dependent uponthe results of other tests.The primary limitation of this study was the use ofthe consensus panel cl<strong>in</strong>ical diagnosis as the referencestandard assessment. Because no criterion standard forthe diagnosis of Crohn’s <strong>disease</strong> exists, we believe the consensuscl<strong>in</strong>ical diagnosis best approximates how this diagnosisis actually made <strong>in</strong> cl<strong>in</strong>ical practice. Crohn’s <strong>disease</strong>is a cl<strong>in</strong>ical diagnosis based upon a comprehensive evaluation<strong>in</strong>clud<strong>in</strong>g cl<strong>in</strong>ical presentation, SB radiographic <strong>imag<strong>in</strong>g</strong>,endoscopic f<strong>in</strong>d<strong>in</strong>gs, and histology. The conceptof us<strong>in</strong>g a consensus diagnosis when no criterion standarddiagnostic test exists has been used previously <strong>in</strong> a studyexam<strong>in</strong><strong>in</strong>g the sensitivity of diagnostic tests (magneticresonance <strong>imag<strong>in</strong>g</strong>, exam<strong>in</strong>ation under anesthesia, andendoscopic ultrasound) for perianal fistulas <strong>in</strong> Crohn’s<strong>disease</strong>. 42 This method unfortunately requires that the resultsof all <strong>imag<strong>in</strong>g</strong> tests will be <strong>in</strong>cluded <strong>in</strong> the determ<strong>in</strong>ationof the consensus cl<strong>in</strong>ical diagnosis with which it isbe<strong>in</strong>g compared. However, we believed this was necessarybecause cl<strong>in</strong>ical symptoms and serologic markers cannotreliably estimate or predict the presence, severity, or locationof active Crohn’s <strong>disease</strong>. Submitt<strong>in</strong>g all patients toexploratory laparoscopy or laparotomy for a criterion standardconfirmation is obviously <strong>in</strong>vasive and impractical.Moreover, a meta-analysis of several studies suggests thatCE may be more sensitive at diagnos<strong>in</strong>g SB Crohn’s <strong>disease</strong>than other <strong>imag<strong>in</strong>g</strong> modalities. 41 This unique situationwarrants <strong>in</strong>clusion of CE <strong>in</strong> the consensus cl<strong>in</strong>icaldiagnosis, to m<strong>in</strong>imize <strong>in</strong>correctly label<strong>in</strong>g lesions seenon CE but not the other <strong>imag<strong>in</strong>g</strong> modalities as false positives.Neither laparotomy nor laparoscopy are rout<strong>in</strong>elyused for diagnos<strong>in</strong>g Crohn’s <strong>disease</strong> <strong>in</strong> standard cl<strong>in</strong>icalpractice, but rather these <strong>in</strong>terventions are reserved forcomplications of Crohn’s that are not amenable to medicaltherapy. Additionally, surgery may detect gross f<strong>in</strong>d<strong>in</strong>gs ofCrohn’s <strong>disease</strong> but may miss mucosal lesions that couldbe cl<strong>in</strong>ically significant.264 GASTROINTESTINAL ENDOSCOPY Volume 68, No. 2 : 2008 www.giejournal.org
Solem et al<strong>Small</strong>-<strong>bowel</strong> <strong>imag<strong>in</strong>g</strong> <strong>in</strong> Crohn’s <strong>disease</strong>As a result of our study, we have adopted the follow<strong>in</strong>gdiagnostic algorithm for evaluat<strong>in</strong>g SB Crohn’s <strong>disease</strong>.CTE and ileocolonoscopy are first-l<strong>in</strong>e comb<strong>in</strong>ed tests,with a comb<strong>in</strong>ed sensitivity of 84% and specificity of94% for active Crohn’s <strong>disease</strong>. CTE has high sensitivity,similar to CE, but with superior specificity. Furthermore,CTE detects extralum<strong>in</strong>al <strong>in</strong>test<strong>in</strong>al complications (eg, fistulasand abscesses) and may help dist<strong>in</strong>guish <strong>in</strong>flammatoryfrom fibrostenotic strictures, facilitat<strong>in</strong>g therapeuticdecisions while avoid<strong>in</strong>g potential risks of reta<strong>in</strong>ed capsules.Ileocolonoscopy stages the extent of <strong>disease</strong> andobta<strong>in</strong>s necessary histology. SBFT should be consideredas an alternative to CTE based upon local expertise orother extenuat<strong>in</strong>g circumstances such as iod<strong>in</strong>e allergyor renal <strong>in</strong>sufficiency. CE should subsequently be performedif the cl<strong>in</strong>ical suspicion for Crohn’s <strong>disease</strong> rema<strong>in</strong>shigh despite a negative evaluation.DISCLOSUREThe follow<strong>in</strong>g authors report that they have no disclosuresrelevant to this publication: C. A. Solem,T. H. Baron, C. J. Gostout, B. T. Petersen, W. J. Trema<strong>in</strong>e,L. J. Egan, W. A. Faubion, K. W. Schroeder, D. S. Pardi,K. A. Hanson, D. A. Jewell, J. M. Barlow, J. E. Huprich,W. S. Harmsen, A. R. Z<strong>in</strong>smeister, W. J. Sandborn. Thefollow<strong>in</strong>g authors report actual or potential conflicts:E. V. Loftus, Jr, received consult<strong>in</strong>g fees from Given Imag<strong>in</strong>g<strong>in</strong> the 12 months prior to implementation of the trial.J. G. Fletcher and C. D. Johnson receive grant supportfrom GE Healthcare, the manufacturer of the multidetectorCT scanner and the iod<strong>in</strong>ated <strong>in</strong>travenous contrastused for CT enterography exams. J. L. Fidler has an NIHgrant, <strong>in</strong> which GE Healthcare is an external collaborator.Supported <strong>in</strong> part by Given Imag<strong>in</strong>g and the MayoFoundation for Medical Education and Research.REFERENCES1. Goldberg H, Caruthers S, Nelson J, et al. Radiographic f<strong>in</strong>d<strong>in</strong>gs of theNational Cooperative Crohn’s <strong>disease</strong> study. Gastroenterology1979;77:925-37.2. Nolan D, Gourtsoyiannis N. Crohn’s <strong>disease</strong> of the small <strong>in</strong>test<strong>in</strong>e: a reviewof the radiological appearances <strong>in</strong> 100 consecutive patients exam<strong>in</strong>edby a barium <strong>in</strong>fusion technique. Cl<strong>in</strong> Radiol 980;31:597–603.3. Nolan D, Piris J. Crohn’s <strong>disease</strong> of the small <strong>in</strong>test<strong>in</strong>e: a comparativestudy of the radiological and pathological appearances. Cl<strong>in</strong> Radiol1980;31:591-6.4. D<strong>in</strong>er W, Hosk<strong>in</strong>s E, Navab F. Radiologic exam<strong>in</strong>ation of the small <strong>in</strong>test<strong>in</strong>e:review of 402 cases and discussion of <strong>in</strong>dications andmethods. South Med J 1984;77:68-74.5. Carlson H. Perspective: the small <strong>bowel</strong> exam<strong>in</strong>ation <strong>in</strong> the diagnosisof Crohn’s <strong>disease</strong>. AJR Am J Roentgenol 1986;147:63-5.6. Bernste<strong>in</strong> C, Boult I, Greenberg H, et al. A <strong>prospective</strong> randomizedcomparison between small <strong>bowel</strong> enteroclysis and small <strong>bowel</strong> follow-through<strong>in</strong> Crohn’s <strong>disease</strong>. Gastroenterology 1997;113:390-8.7. Coremans G, Rutgeerts P, Geboes K, et al. The value of ileoscopy withbiopsy <strong>in</strong> the diagnosis of <strong>in</strong>test<strong>in</strong>al Crohn’s <strong>disease</strong>. Gastro<strong>in</strong>test Endosc1984;30:167-72.8. Lorenz-Meyer H, Malchow H, Miller B, et al. European CooperativeCrohn’s <strong>disease</strong> study (ECCDS): colonoscopy. Digestion 1985;31:109-19.9. Gomes P, Boulay C, Smith C, et al. Relationship between <strong>disease</strong> activity<strong>in</strong>dices and colonoscopic f<strong>in</strong>d<strong>in</strong>gs <strong>in</strong> patients with colonic <strong>in</strong>flammatory<strong>bowel</strong> <strong>disease</strong>. Gut 1986;27:92-5.10. Modigliani R, Mary J. Reproducibility of colonoscopic f<strong>in</strong>d<strong>in</strong>gs <strong>in</strong>Crohn’s <strong>disease</strong>: a <strong>prospective</strong> multicenter study of <strong>in</strong>terobserver variation.Dig Dis Sci 1987;32:1370-9.11. Pera A, Bellando P, Caldera D, et al. Colonoscopy <strong>in</strong> <strong>in</strong>flammatory<strong>bowel</strong> <strong>disease</strong>. Gastroenterology 1987;92:181-5.12. Mary J, Modigliani R. Development and validation of an endoscopic<strong>in</strong>dex of the severity for Crohn’s <strong>disease</strong>: a <strong>prospective</strong> multicentrestudy. Gut 1989;30:983-9.13. Landi B, Anh T, Cortot A, et al. Endoscopic monitor<strong>in</strong>g of Crohn’s <strong>disease</strong>treatment: a <strong>prospective</strong>, randomized cl<strong>in</strong>ical trial. Gastroenterology1992;102:1647-53.14. Marshall J, Barthel J. The frequency of total colonoscopy and term<strong>in</strong>alileal <strong>in</strong>tubation <strong>in</strong> the 1990s. Gastro<strong>in</strong>test Endosc 1993;39:518-20.15. Rob<strong>in</strong>son A, Wolfe P. A <strong>prospective</strong> evaluation of successful term<strong>in</strong>alileum <strong>in</strong>tubation dur<strong>in</strong>g rout<strong>in</strong>e colonoscopy. Gastro<strong>in</strong>test Endosc1994;40:544-6.16. Leighton JA, Shen B, Baron TH, et al. ASGE guidel<strong>in</strong>e: endoscopy <strong>in</strong> thediagnosis and treatment of <strong>in</strong>flammatory <strong>bowel</strong> <strong>disease</strong>. Gastro<strong>in</strong>testEndosc 2006;63:558-65.17. Reittner P, Goritschnig T, Petritsch W, et al. Multiplanar spiral CT enterography<strong>in</strong> patients with Crohn’s <strong>disease</strong> us<strong>in</strong>g a negative oral contrastmaterial: <strong>in</strong>itial results of a non<strong>in</strong>vasive <strong>imag<strong>in</strong>g</strong> approach. EurRadiol 2002;12:2253-7.18. Turetschek K, Schober E, Wunderbald<strong>in</strong>ger P, et al. F<strong>in</strong>d<strong>in</strong>gs at helicalCT-enteroclysis <strong>in</strong> symptomatic patients with Crohn <strong>disease</strong>: correlationwith endoscopic and surgical f<strong>in</strong>d<strong>in</strong>gs. J Comput Assisted Tomogr2002;26:488-92.19. Doerfler OC, Ruppert-Kohlmayr AJ, Reittner P, et al. Helical CT of thesmall <strong>bowel</strong> with an alternative oral contrast material <strong>in</strong> patientswith Crohn <strong>disease</strong>. Abdom Imag<strong>in</strong>g 2003;28:313-8.20. Hassan C, Cerro P, Zullo A, et al. Computed tomography enteroclysis<strong>in</strong> comparison with ileoscopy <strong>in</strong> patients with Crohn’s <strong>disease</strong>. Int JColorectal Dis 2003;18:121-5.21. Wold PB, Fletcher JG, Johnson CD, et al. Assessment of small <strong>bowel</strong>Crohn <strong>disease</strong>: non<strong>in</strong>vasive peroral CT enterography compared withother <strong>imag<strong>in</strong>g</strong> methods and endoscopy–feasibility study. Radiology2003;229:275-81.22. Eliakim R, Suissa A, Yass<strong>in</strong> K, Katz D, Fischer D. Wireless capsule videoendoscopy compared to barium follow-through and computerised tomography<strong>in</strong> patients with suspected Crohn’s <strong>disease</strong> - f<strong>in</strong>al report. DigestLiver Dis 2004;36:519-22.23. Buchman AL, Miller F, Wall<strong>in</strong> A, et al. Videocapsule endoscopy versusbarium contrast studies for diagnosis of Crohn’s <strong>disease</strong> [abstract].Gastroenterology 2004;126:A459.24. Hara AK, Leighton JA, Sharma VK, et al. <strong>Small</strong> <strong>bowel</strong>: Prelim<strong>in</strong>ary comparisonof capsule endoscopy with barium study and CT. Radiology2004;230:260-5.25. Schreyer AG, Seitz J, Feuerbach S, et al. Modern <strong>imag<strong>in</strong>g</strong> us<strong>in</strong>g computertomography and magnetic resonance <strong>imag<strong>in</strong>g</strong> for <strong>in</strong>flammatory<strong>bowel</strong> <strong>disease</strong> (IBD) AU1. Inflammatory Bowel Dis 2004;10:45-54.26. Sailer J, Peloschek P, Schober E, et al. Diagnostic value of CT enteroclysiscompared with conventional enteroclysis <strong>in</strong> patients with Crohn’s<strong>disease</strong>. AJR Am J Roentgenol 2005;185:1575-81.27. Voderholzer WA, Be<strong>in</strong>hoelzl J, Rogalla P, et al. <strong>Small</strong> <strong>bowel</strong> <strong>in</strong>volvement<strong>in</strong> Crohn’s <strong>disease</strong>: a <strong>prospective</strong> comparison of wireless capsuleendoscopy and computed tomography enteroclysis. Gut 2005;54:369-73.28. Bodily KD, Fletcher JG, Solem CA, et al. Crohn <strong>disease</strong>: mural attenuationand thickness at contrast-enhanced CT enterography –www.giejournal.org Volume 68, No. 2 : 2008 GASTROINTESTINAL ENDOSCOPY 265
<strong>Small</strong>-<strong>bowel</strong> <strong>imag<strong>in</strong>g</strong> <strong>in</strong> Crohn’s <strong>disease</strong>Solem et alcorrelation with endoscopic and histologic f<strong>in</strong>d<strong>in</strong>gs of <strong>in</strong>flammation.Radiology 2006;238:505-16.29. Hara AK, Leighton JA, Heigh RI, et al. Crohn <strong>disease</strong> of the small <strong>bowel</strong>:prelim<strong>in</strong>ary comparison among CT enterography, capsule endoscopy,small-<strong>bowel</strong> follow-through, and ileoscopy. Radiology 2006;238:128-34.30. Rajesh A, Magl<strong>in</strong>te DDT. Multislice CT enteroclysis: technique and cl<strong>in</strong>icalapplications. Cl<strong>in</strong> Radiol 2006;61:31-9.31. La Seta F, Buccellato A, Tese L, et al. Multidetector-row CT enteroclysis:<strong>in</strong>dications and cl<strong>in</strong>ical applications. Radiol Med 2006;111:141-58.32. Paulsen SR, Huprich JE, Fletcher JG, et al. CT enterography as a diagnostictool <strong>in</strong> evaluat<strong>in</strong>g small <strong>bowel</strong> disorders: review of cl<strong>in</strong>ical experiencewith over 700 cases. Radiographics 2006;26:641-57, discussion657–62.33. Eliakim R, Fischer D, Suissa A, et al. Wireless capsule video endoscopyis a superior diagnostic tool <strong>in</strong> comparison to barium follow-throughand computerized tomography <strong>in</strong> patients with suspected Crohn’s<strong>disease</strong>. Eur J Gastroenterol Hepatol 2003;15:363-7.34. Fireman Z, Mahajna E, Broide E, et al. Diagnos<strong>in</strong>g small <strong>bowel</strong> Crohn’s<strong>disease</strong> with wireless capsule endoscopy. Gut 2003;52:390-2.35. Herrerias JM, Caunedo A, Rodriguez-Tellaz M, et al. Capsule endoscopy<strong>in</strong> patients with suspected Crohn’s <strong>disease</strong> and negative endoscopy.Endoscopy 2003;35:564-8.36. Buchman AL, Miller FH, Wall<strong>in</strong> A, et al. Videocapsule endoscopy versusbarium contrast studies for the diagnosis of Crohn’s <strong>disease</strong> recurrence<strong>in</strong>volv<strong>in</strong>g the small <strong>in</strong>test<strong>in</strong>e. Am J Gastroenterol 2004;99:2171-7.37. Ge ZZ, Hu YB, Xiao SD. Capsule endoscopy and push enteroscopy <strong>in</strong>the diagnosis of obscure gastro<strong>in</strong>test<strong>in</strong>al bleed<strong>in</strong>g. Ch<strong>in</strong> Med J2004;117:1045-9.38. Chong AKH, Taylor A, Miller A, et al. Capsule endoscopy vs. push enteroscopyand enteroclysis <strong>in</strong> suspected small-<strong>bowel</strong> Crohn’s <strong>disease</strong>.Gastro<strong>in</strong>test Endosc 2005;61:255-61.39. Marmo R, Rotondano G, Piscopo R, et al. Capsule endoscopy versusenteroclysis <strong>in</strong> the detection of small-<strong>bowel</strong> <strong>in</strong>volvement <strong>in</strong> Crohn’s<strong>disease</strong>: a <strong>prospective</strong> trial. Cl<strong>in</strong> Gastroenterol Hepatol 2005;3:772-6.40. Golder SK, Schreyer AG, Endlicher E, et al. Comparison of capsule endoscopyand magnetic resonance (MR) enteroclysis <strong>in</strong> suspected small<strong>bowel</strong> <strong>disease</strong>. Int J Colorectal Dis 2006;21:97-104.41. Triester SL, Leighton JA, Leontiadis GI, et al. A meta-analysis of theyield of capsule endoscopy compared to other diagnostic modalities<strong>in</strong> patients with non-strictur<strong>in</strong>g small <strong>bowel</strong> Crohn’s <strong>disease</strong>. Am JGastroenterol 2006;101:954-64.42. Schwartz D, Wiersema M, Dudiak K, et al. A comparison of endoscopicultrasound, magnetic resonance <strong>imag<strong>in</strong>g</strong>, and exam under anesthesiafor evaluation of Crohn’s perianal fistulas. Gastroenterology 2001;121:1064-72.43. Lashner BA. Sensitivity-specificity trade-off for capsule endoscopy <strong>in</strong>IBD: is it worth it? Am J Gastroenterol 2006;101:965-6.44. Goldste<strong>in</strong> JL, Eisen GM, Lewis B, et al. Video capsule endoscopy to <strong>prospective</strong>lyassess small <strong>bowel</strong> <strong>in</strong>jury with celecoxib, naproxen plusomeprazole, and placebo. Cl<strong>in</strong> Gastroenterol Hepatol 2005;3:133-41.Received September 20, 2007. Accepted February 4, 2008.Current affiliations: Division of Gastroenterology and Hepatology (E.V.L.,T.H.B., C.J.G., B.T.P., W.J.T., W.A.F., K.W.S., D.S.P., K.A.H., D.A.J., W.J.S.),Department of Radiology (J.G.F., J.M.B., J.L.F., J.E.H., C.D.J.), and Division ofBiostatistics (W.S.H, A.R.Z.), Mayo Cl<strong>in</strong>ic College of Medic<strong>in</strong>e, Rochester,M<strong>in</strong>nesota, Park-Nicollet Cl<strong>in</strong>ic (C.A.S.), Sa<strong>in</strong>t Louis Park, M<strong>in</strong>nesota, USA,Cl<strong>in</strong>ical Pharmacology Unit (L.J.E.), University College Hospital, Galway,Ireland, Department of Radiology (C.D.J.), Mayo Cl<strong>in</strong>ic, Scottsdale, Arizona,USA.Presented <strong>in</strong> part at the 106th Annual Meet<strong>in</strong>g of the AmericanGastroenterological Association, Digestive Disease Week, May 14-19,2005, Chicago, Ill<strong>in</strong>ois (Gastroenterology 2005;128[Suppl 2]:A74).Repr<strong>in</strong>t requests: Edward V. Loftus, Jr., MD, Division of Gastroenterologyand Hepatology, Mayo Cl<strong>in</strong>ic, 200 First Street SW, Rochester, MN 55905.266 GASTROINTESTINAL ENDOSCOPY Volume 68, No. 2 : 2008 www.giejournal.org