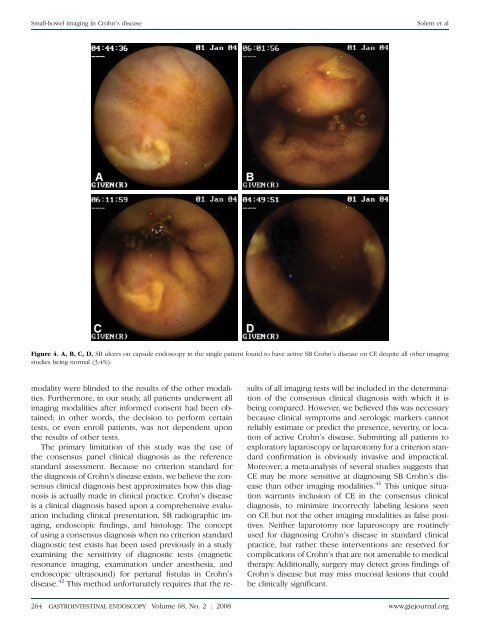
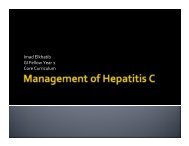
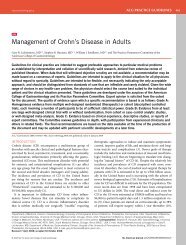
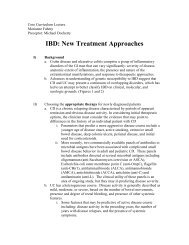
<strong>Small</strong>-<strong>bowel</strong> <strong>imag<strong>in</strong>g</strong> <strong>in</strong> Crohn’s <strong>disease</strong>Solem et alFigure 4. A, B, C, D, SB ulcers on capsule endoscopy <strong>in</strong> the s<strong>in</strong>gle patient found to have active SB Crohn’s <strong>disease</strong> on CE despite all other <strong>imag<strong>in</strong>g</strong>studies be<strong>in</strong>g normal (3.4%).modality were bl<strong>in</strong>ded to the results of the other modalities.Furthermore, <strong>in</strong> our study, all patients underwent all<strong>imag<strong>in</strong>g</strong> modalities after <strong>in</strong>formed consent had been obta<strong>in</strong>ed;<strong>in</strong> other words, the decision to perform certa<strong>in</strong>tests, or even enroll patients, was not dependent uponthe results of other tests.The primary limitation of this study was the use ofthe consensus panel cl<strong>in</strong>ical diagnosis as the referencestandard assessment. Because no criterion standard forthe diagnosis of Crohn’s <strong>disease</strong> exists, we believe the consensuscl<strong>in</strong>ical diagnosis best approximates how this diagnosisis actually made <strong>in</strong> cl<strong>in</strong>ical practice. Crohn’s <strong>disease</strong>is a cl<strong>in</strong>ical diagnosis based upon a comprehensive evaluation<strong>in</strong>clud<strong>in</strong>g cl<strong>in</strong>ical presentation, SB radiographic <strong>imag<strong>in</strong>g</strong>,endoscopic f<strong>in</strong>d<strong>in</strong>gs, and histology. The conceptof us<strong>in</strong>g a consensus diagnosis when no criterion standarddiagnostic test exists has been used previously <strong>in</strong> a studyexam<strong>in</strong><strong>in</strong>g the sensitivity of diagnostic tests (magneticresonance <strong>imag<strong>in</strong>g</strong>, exam<strong>in</strong>ation under anesthesia, andendoscopic ultrasound) for perianal fistulas <strong>in</strong> Crohn’s<strong>disease</strong>. 42 This method unfortunately requires that the resultsof all <strong>imag<strong>in</strong>g</strong> tests will be <strong>in</strong>cluded <strong>in</strong> the determ<strong>in</strong>ationof the consensus cl<strong>in</strong>ical diagnosis with which it isbe<strong>in</strong>g compared. However, we believed this was necessarybecause cl<strong>in</strong>ical symptoms and serologic markers cannotreliably estimate or predict the presence, severity, or locationof active Crohn’s <strong>disease</strong>. Submitt<strong>in</strong>g all patients toexploratory laparoscopy or laparotomy for a criterion standardconfirmation is obviously <strong>in</strong>vasive and impractical.Moreover, a meta-analysis of several studies suggests thatCE may be more sensitive at diagnos<strong>in</strong>g SB Crohn’s <strong>disease</strong>than other <strong>imag<strong>in</strong>g</strong> modalities. 41 This unique situationwarrants <strong>in</strong>clusion of CE <strong>in</strong> the consensus cl<strong>in</strong>icaldiagnosis, to m<strong>in</strong>imize <strong>in</strong>correctly label<strong>in</strong>g lesions seenon CE but not the other <strong>imag<strong>in</strong>g</strong> modalities as false positives.Neither laparotomy nor laparoscopy are rout<strong>in</strong>elyused for diagnos<strong>in</strong>g Crohn’s <strong>disease</strong> <strong>in</strong> standard cl<strong>in</strong>icalpractice, but rather these <strong>in</strong>terventions are reserved forcomplications of Crohn’s that are not amenable to medicaltherapy. Additionally, surgery may detect gross f<strong>in</strong>d<strong>in</strong>gs ofCrohn’s <strong>disease</strong> but may miss mucosal lesions that couldbe cl<strong>in</strong>ically significant.264 GASTROINTESTINAL ENDOSCOPY Volume 68, No. 2 : 2008 www.giejournal.org
Solem et al<strong>Small</strong>-<strong>bowel</strong> <strong>imag<strong>in</strong>g</strong> <strong>in</strong> Crohn’s <strong>disease</strong>As a result of our study, we have adopted the follow<strong>in</strong>gdiagnostic algorithm for evaluat<strong>in</strong>g SB Crohn’s <strong>disease</strong>.CTE and ileocolonoscopy are first-l<strong>in</strong>e comb<strong>in</strong>ed tests,with a comb<strong>in</strong>ed sensitivity of 84% and specificity of94% for active Crohn’s <strong>disease</strong>. CTE has high sensitivity,similar to CE, but with superior specificity. Furthermore,CTE detects extralum<strong>in</strong>al <strong>in</strong>test<strong>in</strong>al complications (eg, fistulasand abscesses) and may help dist<strong>in</strong>guish <strong>in</strong>flammatoryfrom fibrostenotic strictures, facilitat<strong>in</strong>g therapeuticdecisions while avoid<strong>in</strong>g potential risks of reta<strong>in</strong>ed capsules.Ileocolonoscopy stages the extent of <strong>disease</strong> andobta<strong>in</strong>s necessary histology. SBFT should be consideredas an alternative to CTE based upon local expertise orother extenuat<strong>in</strong>g circumstances such as iod<strong>in</strong>e allergyor renal <strong>in</strong>sufficiency. CE should subsequently be performedif the cl<strong>in</strong>ical suspicion for Crohn’s <strong>disease</strong> rema<strong>in</strong>shigh despite a negative evaluation.DISCLOSUREThe follow<strong>in</strong>g authors report that they have no disclosuresrelevant to this publication: C. A. Solem,T. H. Baron, C. J. Gostout, B. T. Petersen, W. J. Trema<strong>in</strong>e,L. J. Egan, W. A. Faubion, K. W. Schroeder, D. S. Pardi,K. A. Hanson, D. A. Jewell, J. M. Barlow, J. E. Huprich,W. S. Harmsen, A. R. Z<strong>in</strong>smeister, W. J. Sandborn. Thefollow<strong>in</strong>g authors report actual or potential conflicts:E. V. Loftus, Jr, received consult<strong>in</strong>g fees from Given Imag<strong>in</strong>g<strong>in</strong> the 12 months prior to implementation of the trial.J. G. Fletcher and C. D. Johnson receive grant supportfrom GE Healthcare, the manufacturer of the multidetectorCT scanner and the iod<strong>in</strong>ated <strong>in</strong>travenous contrastused for CT enterography exams. J. L. Fidler has an NIHgrant, <strong>in</strong> which GE Healthcare is an external collaborator.Supported <strong>in</strong> part by Given Imag<strong>in</strong>g and the MayoFoundation for Medical Education and Research.REFERENCES1. Goldberg H, Caruthers S, Nelson J, et al. Radiographic f<strong>in</strong>d<strong>in</strong>gs of theNational Cooperative Crohn’s <strong>disease</strong> study. Gastroenterology1979;77:925-37.2. Nolan D, Gourtsoyiannis N. Crohn’s <strong>disease</strong> of the small <strong>in</strong>test<strong>in</strong>e: a reviewof the radiological appearances <strong>in</strong> 100 consecutive patients exam<strong>in</strong>edby a barium <strong>in</strong>fusion technique. Cl<strong>in</strong> Radiol 980;31:597–603.3. Nolan D, Piris J. Crohn’s <strong>disease</strong> of the small <strong>in</strong>test<strong>in</strong>e: a comparativestudy of the radiological and pathological appearances. Cl<strong>in</strong> Radiol1980;31:591-6.4. D<strong>in</strong>er W, Hosk<strong>in</strong>s E, Navab F. Radiologic exam<strong>in</strong>ation of the small <strong>in</strong>test<strong>in</strong>e:review of 402 cases and discussion of <strong>in</strong>dications andmethods. South Med J 1984;77:68-74.5. Carlson H. Perspective: the small <strong>bowel</strong> exam<strong>in</strong>ation <strong>in</strong> the diagnosisof Crohn’s <strong>disease</strong>. AJR Am J Roentgenol 1986;147:63-5.6. Bernste<strong>in</strong> C, Boult I, Greenberg H, et al. A <strong>prospective</strong> randomizedcomparison between small <strong>bowel</strong> enteroclysis and small <strong>bowel</strong> follow-through<strong>in</strong> Crohn’s <strong>disease</strong>. Gastroenterology 1997;113:390-8.7. Coremans G, Rutgeerts P, Geboes K, et al. The value of ileoscopy withbiopsy <strong>in</strong> the diagnosis of <strong>in</strong>test<strong>in</strong>al Crohn’s <strong>disease</strong>. Gastro<strong>in</strong>test Endosc1984;30:167-72.8. Lorenz-Meyer H, Malchow H, Miller B, et al. European CooperativeCrohn’s <strong>disease</strong> study (ECCDS): colonoscopy. Digestion 1985;31:109-19.9. Gomes P, Boulay C, Smith C, et al. Relationship between <strong>disease</strong> activity<strong>in</strong>dices and colonoscopic f<strong>in</strong>d<strong>in</strong>gs <strong>in</strong> patients with colonic <strong>in</strong>flammatory<strong>bowel</strong> <strong>disease</strong>. Gut 1986;27:92-5.10. Modigliani R, Mary J. Reproducibility of colonoscopic f<strong>in</strong>d<strong>in</strong>gs <strong>in</strong>Crohn’s <strong>disease</strong>: a <strong>prospective</strong> multicenter study of <strong>in</strong>terobserver variation.Dig Dis Sci 1987;32:1370-9.11. Pera A, Bellando P, Caldera D, et al. Colonoscopy <strong>in</strong> <strong>in</strong>flammatory<strong>bowel</strong> <strong>disease</strong>. Gastroenterology 1987;92:181-5.12. Mary J, Modigliani R. Development and validation of an endoscopic<strong>in</strong>dex of the severity for Crohn’s <strong>disease</strong>: a <strong>prospective</strong> multicentrestudy. Gut 1989;30:983-9.13. Landi B, Anh T, Cortot A, et al. Endoscopic monitor<strong>in</strong>g of Crohn’s <strong>disease</strong>treatment: a <strong>prospective</strong>, randomized cl<strong>in</strong>ical trial. Gastroenterology1992;102:1647-53.14. Marshall J, Barthel J. The frequency of total colonoscopy and term<strong>in</strong>alileal <strong>in</strong>tubation <strong>in</strong> the 1990s. Gastro<strong>in</strong>test Endosc 1993;39:518-20.15. Rob<strong>in</strong>son A, Wolfe P. A <strong>prospective</strong> evaluation of successful term<strong>in</strong>alileum <strong>in</strong>tubation dur<strong>in</strong>g rout<strong>in</strong>e colonoscopy. Gastro<strong>in</strong>test Endosc1994;40:544-6.16. Leighton JA, Shen B, Baron TH, et al. ASGE guidel<strong>in</strong>e: endoscopy <strong>in</strong> thediagnosis and treatment of <strong>in</strong>flammatory <strong>bowel</strong> <strong>disease</strong>. Gastro<strong>in</strong>testEndosc 2006;63:558-65.17. Reittner P, Goritschnig T, Petritsch W, et al. Multiplanar spiral CT enterography<strong>in</strong> patients with Crohn’s <strong>disease</strong> us<strong>in</strong>g a negative oral contrastmaterial: <strong>in</strong>itial results of a non<strong>in</strong>vasive <strong>imag<strong>in</strong>g</strong> approach. EurRadiol 2002;12:2253-7.18. Turetschek K, Schober E, Wunderbald<strong>in</strong>ger P, et al. F<strong>in</strong>d<strong>in</strong>gs at helicalCT-enteroclysis <strong>in</strong> symptomatic patients with Crohn <strong>disease</strong>: correlationwith endoscopic and surgical f<strong>in</strong>d<strong>in</strong>gs. J Comput Assisted Tomogr2002;26:488-92.19. Doerfler OC, Ruppert-Kohlmayr AJ, Reittner P, et al. Helical CT of thesmall <strong>bowel</strong> with an alternative oral contrast material <strong>in</strong> patientswith Crohn <strong>disease</strong>. Abdom Imag<strong>in</strong>g 2003;28:313-8.20. Hassan C, Cerro P, Zullo A, et al. Computed tomography enteroclysis<strong>in</strong> comparison with ileoscopy <strong>in</strong> patients with Crohn’s <strong>disease</strong>. Int JColorectal Dis 2003;18:121-5.21. Wold PB, Fletcher JG, Johnson CD, et al. Assessment of small <strong>bowel</strong>Crohn <strong>disease</strong>: non<strong>in</strong>vasive peroral CT enterography compared withother <strong>imag<strong>in</strong>g</strong> methods and endoscopy–feasibility study. Radiology2003;229:275-81.22. Eliakim R, Suissa A, Yass<strong>in</strong> K, Katz D, Fischer D. Wireless capsule videoendoscopy compared to barium follow-through and computerised tomography<strong>in</strong> patients with suspected Crohn’s <strong>disease</strong> - f<strong>in</strong>al report. DigestLiver Dis 2004;36:519-22.23. Buchman AL, Miller F, Wall<strong>in</strong> A, et al. Videocapsule endoscopy versusbarium contrast studies for diagnosis of Crohn’s <strong>disease</strong> [abstract].Gastroenterology 2004;126:A459.24. Hara AK, Leighton JA, Sharma VK, et al. <strong>Small</strong> <strong>bowel</strong>: Prelim<strong>in</strong>ary comparisonof capsule endoscopy with barium study and CT. Radiology2004;230:260-5.25. Schreyer AG, Seitz J, Feuerbach S, et al. Modern <strong>imag<strong>in</strong>g</strong> us<strong>in</strong>g computertomography and magnetic resonance <strong>imag<strong>in</strong>g</strong> for <strong>in</strong>flammatory<strong>bowel</strong> <strong>disease</strong> (IBD) AU1. Inflammatory Bowel Dis 2004;10:45-54.26. Sailer J, Peloschek P, Schober E, et al. Diagnostic value of CT enteroclysiscompared with conventional enteroclysis <strong>in</strong> patients with Crohn’s<strong>disease</strong>. AJR Am J Roentgenol 2005;185:1575-81.27. Voderholzer WA, Be<strong>in</strong>hoelzl J, Rogalla P, et al. <strong>Small</strong> <strong>bowel</strong> <strong>in</strong>volvement<strong>in</strong> Crohn’s <strong>disease</strong>: a <strong>prospective</strong> comparison of wireless capsuleendoscopy and computed tomography enteroclysis. Gut 2005;54:369-73.28. Bodily KD, Fletcher JG, Solem CA, et al. Crohn <strong>disease</strong>: mural attenuationand thickness at contrast-enhanced CT enterography –www.giejournal.org Volume 68, No. 2 : 2008 GASTROINTESTINAL ENDOSCOPY 265